Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
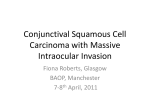
Case Report DOI: 10.17354/cr/2016/197 Management and Treatment of Ocular Surface Neoplasia Ashjan Y Bamahfouz1, Hanan M Abd El-Moneim2, Mohammed Abdulqadir Bachal3, Khaled Mohammed Bahubaishi4 Assistant Professor, Department of Ophthalmology, Umm al-Qura University, Mecca, Kingdom of Saudi Arabia, 2Professor, Department of Pathology, Umm al-Qura University, Mecca, Kingdom of Saudi Arabia, 3Assistant Consultant, Ophthalmology Center, King Abdullah Medical City, Mecca, Kingdom of Saudi Arabia, 4Intern, Department of Medicine, King Abdul Aziz University, Jeddah, Kingdom of Saudi Arabia 1 Conjunctival squamous cell carcinoma (CSCC) is an invasive ocular surface neoplasia ranging from dysplasia to carcinoma in situ to invasive squamous cell carcinoma, which is identified as premalignant and malignant epithelial lesions. Often, it is seen in males in tropical countries lying close to the equator where there is excessive exposure to sunlight. Clinical diagnosis requires close examination with a degree of high suspicion. Appropriate and definitive diagnosis of conjunctival squamous neoplasia by ocular pathologists and the need for future detailed clinicopathologic studies is recommended. Appropriate and definitive diagnosis requires histopathology. We describe a case of CSCC underlying dysplasia with intraepithelial squamous cell neoplasia, where the case was confirmed by histopathological examination. The treatment modality involving surgery and medication and follow-up is described. There was no evidence of recurrence, complication, or metastasis. Keywords: Cornea, Mitomycin-C, Ocular surface squamous neoplasia, Squamous cell carcinoma of conjunctiva INTRODUCTION Ocular carcinomas termed as ocular surface squamous neoplasia (OSSN) are the most common tumor of conjunctival epithelium. They carry a high risk of visual impairment which can be devastating and permanent. However, 4 conjunctival squamous cell carcinomas (CSCC) are considered to be rare.1,2 More aggressive course recognized among patients in tropical/thermal regions due to environmental factors. All suspicious ocular lesions should undergo biopsy for early diagnosis.2,3 CSCC in situ which arises from limbal stem cells of the conjunctival epithelium is a malignant neoplasm that invades through epithelial basement membrane into the corneal stroma through the conjunctiva or rarely to the interior of eye or orbit.4,5 Over a period of 10-year in Saudi Arabia about conjunctival SCC were found to have invaded the orbit. Many factors contribute to the aggressiveness of CSCC in this geographic location; these factors are continual exposure to ultraviolet Access this article online Month of Submission Month of Peer Review Month of Acceptance Month of Publishing : : : : 01-2016 02-2016 03-2016 03-2016 www.ijsscr.com rays, genetic factors, and chronic irritation. Often, delay in presentation and inadequate initial resection are factors contributing to orbital invasion.6-9 The spectrum in OSSN includes mild dysplasia on one end and invasive squamous cell carcinoma on the other end. Diagnosis of CSCC depends on the histopathological examination.9 Although the clinical diagnosis of in situ disease is often high (86%), invasive carcinoma is much less (35%). Preoperatively, correctly diagnosed lesions are much larger ones and are those with hyperkeratosis.10 It is often difficult to distinguish invasive OSSN from other common lesions such as pinguecula and pterygium due to similarities in clinical features.11 The initial therapeutic approach to this disease is surgery. In addition, cryotherapy and mitomycin-C (MMC) are also potentially good therapeutic approaches.12 Orbital invasion and loss of the eye are usually due to delay in presentation. Successful treatment of these tumors is often very challenging. It also requires advanced diagnostic and therapeutic tools for improving treatment outcomes.13 Superficial excision remains the important initial step in management, as it is impossible to exclude invasive disease on clinical grounds. Hence, excision allows tissue for immediate histopathological diagnosis, resulting in surgical debulking, and hence removes lifethreatening consequences. The disadvantage of primary excision alone is the high recurrence rate, which ranges from 15% to 52%. Therefore, several adjunctive treatments Corresponding Author: Dr. Irshad A Subhan, Associate Consultant, King Abdulla Medical City, Mecca, Kingdom of Saudi Arabia. Phone: +91-966543027674. E-mail: [email protected] IJSS Case Reports & Reviews | March 2016 | Vol 2 | Issue 10 1 Bamahfouz, et al.: Ocular Surface Neoplasia Management and Outcome have been described in the literature in an a empt to reduce the recurrence rate. The efficacy of these various adjunctive therapies is still debated.14 Surgical excision involving a wide area and adjuvant chemotherapy may be curative in some cases. However importantly, high degree of clinical suspicion leading early diagnosis followed by effective treatment will minimize the mortality and morbidity related to the disease.7 CASE REPORT A 68-year-old male patient presented to the outpatient clinic, at the King Abdullah Medical City in January 2014 with the chief complaint of reduced vision in his right eye, and gradually increasing mass in the left eye. His general physical examination was normal. A complete ophthalmic examination bilaterally revealed visual acuity without correction of hand motion in the right eye and 20/40 in the left eye. Intraocular pressures of 14 and 16 mm of Hg in the right eye and left eye, respectively. Both pupils were round and equally reacting to light and accommodation. Ocular movements were normal. Slit lamp examination showed mature cataract in the right eye and early cataract in the left eye. There was 3 mm × 4 mm mass minimally elevated conjunctival lesion in the left eye nasally, with regular margins and fixed base on the cornea (Figure 1a and 1b). Clinically, the case was diagnosed as OSSN. Fundus examination was normal. There was no regional lymphadenopathy. The patient was subjected for surgical intervention. Total excision of the conjunctival mass with a free margin of 2 mm followed by double freeze-thaw cryo-application. Amniotic membrane transplant was carried out as shown in the pictures (Figure 1c). Histopathological examination revealed moderately differentiated squamous cell carcinoma with a background of severe squamous dysplasia and carcinoma in situ (Figure 2a-c) with invasive features involving superior and temporal margins. Postoperatively, he was treated with topical MMC 0.02% eye drops 4 times/ day for 14 days for two cycles with refresh tears eye drops 4 times/day for two weeks between the cycles along with topical steroids and antibiotics. The patient was followed up every 2 months at the beginning then examined at 6 months intervals. 1-year follow-up showed no recurrence or complications from treatment. DISCUSSION The bulbar conjunctiva and limbal area are the most frequent sites of conjunctival tumors. Therefore, early diagnosis and excision were performed. Truly cancerous lesions are absent. Hence, it is emphasized to perform early excision of any enlarging limbal lesion in preventing malignant transformation. Africa has the highest incidence of OSSN in the world, where males and females are equally affected.15 Our case highlights the importance of considering CSCC in refractory cases of conjunctival inflammation with limbal and corneal epithelial involvement. OSSN regarded as uncommon disease with a propensity to affect men in their sixth decade. Histologically, the disease characterized by changes in basal, supra-basal, superficial, and full thickness epithelium. Characteristic cellular changes are increased hyperchromatism, pleomorphism, and loss of polarity, which when severe, involves with tumor cells breaching the basement membrane and also invading into the matrix of the stroma.16 The risk of squamous cell carcinoma of conjunctiva/dysplasia seemed to be higher in the presence of multiple than single infections. In the equatorial Africans, the conjunctiva is the site that is not protected from ultraviolet light by heavy pigmentation.17 Although complete excision with cryotherapy gives good results with localized lesions, other newer modalities such as immunotherapy hold a promise in large unresectable and recurrent lesions.9 As of now, the best available options remain early detection and effective treatment. However, non-invasive diagnostic methods are still not available, and there is no evidence to guide treatment.15 Herein, we stress the need for early diagnosis and management of lesions. Routine histopathological diagnosis a a b c Figure 1: (a) Slit lamp photograph under diffuse illumination of left eye show sessile, vascular conjunctival epithelial tumor cover temporal side of limbus of the left eye. (b) A close-up view of the overhanging conjunctivo-corneal mass with large intrinsic and feeder vessels. (c) Post-operative excision of the conjunctival mass was done with free margin of 2 mm and amniotic membrane transplant covering the conjunctival defect after excision biopsy 2 b c Figure 2: (a) Hematoxylin and Eosin stain. The histopathologic appearance of the tumor showed infiltrating moderately differentiated squamous cell carcinoma. The infiltrating nests and cords were extending from the basement line into the underlying connective tissue with lymphocytic infiltrate within the connective tissue. (b) Background of squamous dysplasia and carcinoma in situ are seen with the replacement of conjunctival epithelium by dysplastic squamous cells, thickening, and keratinization of superficial cells. (c) The infiltrating moderately differentiated squamous cell carcinoma with higher magnification IJSS Case Reports & Reviews | March 2016 | Vol 2 | Issue 10 Bamahfouz, et al.: Ocular Surface Neoplasia Management and Outcome of orbital and adnexal tumors uncovered some rare tumors and varied histological types. This improves the management of these patients. CSCC, an invasive form of OSSN that responds well and without any recurrence on a year follow-up with combined treatment of surgical excision, cryotherapy, and topical chemotherapy-like MMC.18 Surgery, chemotherapy, and immunotherapy are other treatment modalities which in combination show good results in aggressive, recurrent, and large tumors.9 Surgery often resulted in a low recurrence rate during the follow-up period with fewer complications.17 For Ca in situ simple surgical excision associated with cryotherapy was quiet effective. 2. 3. 4. 5. 6. Various treatments have been described with good results, with the use of MMC and topical cyclosporin to prevent recurrences.19 MMC allows treatment of the entire ocular surface, including the conjunctival fornices, and may reach and destroy subclinical disease and prevent new tumors arising elsewhere on the ocular surface.14 Often, delay in presentation and previous unsuccessful surgery leads to invasion of the orbit and loss of the eye.7 Primary and residual in situ disease can be treated with topical chemotherapy.20 7. MMC treatment following surgical excision reduces the recurrence rate and should be considered as the adjuvant therapy in the treatment of primary and localized recurrent disease.21,22 MMC can be used as only therapy in more diffuse disease, often requiring a close follow-up because of the significant risk of recurrent disease or persistent. Clinically, whether the tumor is benign or malignant is of critical importance. Histopathology is the gold standard in the diagnoses of various grades and types of CSCC and gives a fair understanding of disease prognosis. 11. CONCLUSION 15. CSCC, an invasive form of OSSN responded well and without any recurrence on a year follow-up with combined treatment of surgical excision, cryotherapy, and topical chemotherapy-like MMC. We recommend the use of such a combined approach in the management of such cases. ACKNOWLEDGMENTS We are grateful to Dr. Tahira Hamid, Associate Consultant Pathologist from the Department of Pathology of King Abdullah Medical City. REFERENCES 1. Chauhan S, Sen S, Sharma A, Tandon R, Kashyap S, Pushker N, et al. American joint commi ee on cancer staging and clinicopathological IJSS Case Reports & Reviews | March 2016 | Vol 2 | Issue 10 8. 9. 10. 12. 13. 14. 16. 17. 18. 19. 20. 21. high-risk predictors of ocular surface squamous neoplasia: A study from a tertiary eye center in India. Arch Pathol Lab Med 2014;138:1488-94. Tiong T, Borooah S, Msosa J, Dean W, Smith C, Kambewa E, et al. Clinicopathological review of ocular surface squamous neoplasia in Malawi. Br J Ophthalmol 2013;97:961-4. Elshazly LH. A clinicopathologic study of excised conjunctival lesions. Middle East Afr J Ophthalmol 2011;18:48-54. Gichuhi S, Sagoo MS, Weiss HA, Burton MJ. Epidemiology of ocular surface squamous neoplasia in Africa. Trop Med Int Health 2013;18:1424-43. Rishi P, Shields CL, Eagle RC. Conjunctival intraepithelial neoplasia with corneal furrow degeneration. Indian J Ophthalmol 2014;62:809-11. Ackuaku-Dogbe E. Histopathological features of tumours of the orbit and Adnexia seen in Korle-Bu teaching Hospital Ghana. West Afr J Med 2012;31:58-62. Johnson TE, Tabbara KF, Weatherhead RG, Kersten RC, Rice C, Nasr AM. Secondary squamous cell carcinoma of the orbit. Arch Ophthalmol 1997;115:75-8. Gökmen Soysal H, Ardiç F. Malignant conjunctival tumors invading the orbit. Ophthalmologica 2008;222:338-43. Emmanuel B, Ruder E, Lin SW, Abnet C, Hollenbeck A, Mbulaiteye S. Incidence of squamous-cell carcinoma of the conjunctiva and other eye cancers in the NIH-AARP diet and health study. Ecancermedicalscience 2012;6:254. Mittal R, Rath S, Vemuganti GK. Ocular surface squamous neoplasia - Review of etio-pathogenesis and an update on clinico-pathological diagnosis. Saudi J Ophthalmol 2013;27:177-86. McKelvie PA, Daniell M, McNab A, Loughnan M, Santamaria JD. Squamous cell carcinoma of the conjunctiva: A series of 26 cases. Br J Ophthalmol 2002;86:168-73. Moshirfar M, Khalifa YM, Kuo A, Davis D, Mamalis N. Ocular surface squamous neoplasia masquerading as superior limbic keratoconjunctivitis. Middle East Afr J Ophthalmol 2011;18:74-6. Nagaiah G, Stotler C, Orem J, Mwanda WO, Remick SC. Ocular surface squamous neoplasia in patients with HIV infection in sub-Saharan Africa. Curr Opin Oncol 2010;22:437-42. Nagata M, Nakamura T, Sotozono C, Inatomi T, Yokoi N, Kinoshita S. LRIG1 as a potential novel marker for neoplastic transformation in ocular surface squamous neoplasia. PLoS One 2014;9:e93164. Chen C, Louis D, Dodd T, Muecke J. Mitomycin C as an adjunct in the treatment of localised ocular surface squamous neoplasia. Br J Ophthalmol 2004;88:17-8. Di Girolamo N. Association of human papilloma virus with pterygia and ocular-surface squamous neoplasia. Eye (Lond) 2012;26:202-11. Wa d d e l l K M , D o w n i n g R G , L u c a s S B , N e w t o n R . Corneo-conjunctival carcinoma in Uganda. Eye (Lond) 2006;20:893-9. Nigwekar S, Gupta A, Bhosale M, Haldipurkar T, Baviskar B, Misra S. Combined treatment modality for invasive ocular surface squamous neoplasia in an HIV positive patient: A case report. Int J Stud Res 2012;2:25-7. Crim N, Forniés-Paz ME, Monti R, Espósito E, Maccio JP, Urrets-Zavalía JA. In situ carcinoma of the conjunctiva: Surgical excision associated with cryotherapy. Clin Ophthalmol 2013;7:1889-93. Yin VT, Merri HA, Sniegowski M, Esmaeli B. Eyelid and ocular surface carcinoma: Diagnosis and management. Clin Dermatol 2015;33:159-69. Gupta A, Muecke J. Treatment of ocular surface squamous 3 Bamahfouz, et al.: Ocular Surface Neoplasia Management and Outcome neoplasia with Mitomycin C. Br J Ophthalmol 2010;94:555-8. 22. Prabhasawat P, Tarinvorakup P, Tesavibul N, Uiprasertkul M, Kosrirukvongs P, Booranapong W, et al. Topical 0.002% mitomycin C for the treatment of conjunctival-corneal intraepithelial neoplasia and squamous cell carcinoma. Cornea 2005;24:443-8. 4 How to cite this article: Bamahfouz AY, El-Moneim HM, Bachal MA, Bahubaishi KM. Management and Treatment of Ocular Surface Neoplasia. IJSS Case Reports & Reviews. 2016;2(10):1-4. Source of Support: Nil, Conflict of Interest: None declared. IJSS Case Reports & Reviews | March 2016 | Vol 2 | Issue 10