Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Saturated fat and cardiovascular disease wikipedia , lookup
Electrocardiography wikipedia , lookup
Cardiovascular disease wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Heart failure wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Coronary artery disease wikipedia , lookup
Cardiac surgery wikipedia , lookup
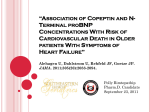
Clinical Chemistry 56:11 1718–1724 (2010) Proteomics and Protein Markers Prognostic Assessment of Elderly Patients with Symptoms of Heart Failure by Combining High-Sensitivity Troponin T and N-Terminal Pro–B-Type Natriuretic Peptide Measurements Urban Alehagen,1* Ulf Dahlström,1 Jens F. Rehfeld,2 and Jens P. Goetze2 BACKGROUND: N-terminal pro–B-type natriuretic peptide (NT-proBNP) is a useful biomarker in heart failure assessment, whereas measurement of cardiac troponin is central in the diagnosis of patients with acute coronary syndromes. This report examined the prognostic use of combining high-sensitivity cardiac troponin T (hs-cTnT) and NT-proBNP measurements in elderly patients presenting to a primary care center with symptoms associated with heart failure. METHODS: A total of 470 elderly patients (age range 65– 86 years) presenting with symptoms of heart failure were recruited from primary healthcare. In addition to clinical examination and echocardiography, hs-cTnT and NT-proBNP plasma concentrations were measured. All patients were followed for 10 years, and cardiovascular mortality was registered. RESULTS: By use of the hs-cTnT assay, 80.4% of the population had plasma concentrations above the lower detection limit of the assay. Of those displaying a plasma concentration of hs-cTnT ⬎99th percentile of a healthy population, 43% also had an NT-proBNP concentration in the fourth quartile (⬎507 ng/L). In the multivariate analysis, we observed a 2.5-fold increased risk for cardiovascular mortality in individuals with a plasma NT-proBNP concentration ⬎507 ng/L (P ⬍ 0.0001). Conversely, patients with hs-cTnT ⬎99th percentile displayed an approximately 2-fold increased risk for cardiovascular mortality (P ⫽ 0.0002). Combining the 2 biomarkers, NT-proBNP concentrations ⬎507 ng/L with hs-cTnT ⬎99th percentile increased the risk 3-fold, even after adjustment for clinical variables such as age, sex, impaired estimated glomerular filtration rate, and anemia (P ⬍ 0.0001). 1 Department of Medical and Health Sciences, Linkoping University, Linkoping, Sweden; 2 Department of Clinical Biochemistry, Rigshospitalet, University of Copenhagen, Copenhagen, Denmark. * Address correspondence to this author at: Department of Cardiology, Heart Center, University of Linköping, SE-581 85 Linköping, Sweden. Fax ⫹46-13222324; e-mail [email protected]. 1718 CONCLUSIONS: hs-cTnT and NT-proBNP measurements combined provide better prognostic information than using either biomarker separately in elderly patients with symptoms associated with heart failure. © 2010 American Association for Clinical Chemistry The pathophysiological concept of heart failure has changed dramatically during the last decade with increased understanding of a multiorgan neurohormonal response (1, 2 ) as well as activation of immunological (3, 4 ) and inflammatory systems (5–7 ). As a consequence, new biomarkers for diagnosis and prognosis in heart failure have emerged (8 –10 ). The use of biomarkers extends from diagnostic assessment to identification of patients at high risk for hospitalization or cardiovascular mortality. B-type natriuretic peptide (BNP)3 and the N-terminal fragment of the biosynthetic precursor (N-terminal pro–B-type natriuretic peptide [NT-proBNP]) have been intensively examined as heart failure biomarkers (11 ). The relation between increased plasma concentrations of cardiac troponin T (cTnT) or cTnI and acute coronary syndrome is firmly established (12, 13 ). Interestingly, cardiac troponin concentrations near the 99th percentile of a healthy population have recently been suggested to be associated with risk for cardiovascular complications and death (14, 15 ). Thus, small increases in plasma cardiac troponin concentrations below those usually observed in myocardial infarction may indicate “low-grade” myocardial damage due to nonischemic mechanisms (16 –18 ). Because the sensitivity of the cardiac troponin assays has improved greatly, it is possible to test whether such small increases in plasma concentrations can provide prognostic information also in heart failure (19 ). From the Received December 13, 2009; accepted August 20, 2010. Previously published online at DOI: 10.1373/clinchem.2009.141341 3 Nonstandard abbreviations: BNP, B-type natriuretic peptide; NT-proBNP, N-terminal pro–B-type natriuretic peptide; cTnT, cardiac troponin T; hs-cTnT, high-sensitivity cTnT; EF, ejection fraction; AUC, area under the curve. hs-cTnT and NT-proBNP in Heart Failure American Acute Decompensated Heart Failure National Registry (ADHERE), it was reported that patients with acute heart failure and increased cTnT or cTnI plasma concentrations displayed a 2.5-fold increased risk of death (20 ). However, this report was based on troponin measurement using contemporary, but not high-sensitivity, assays. It has been suggested that using 2 biomarkers together in cardiovascular diagnosis and prognosis may provide better risk information than using only 1 marker. For instance, this approach has been reported in patients with stable coronary artery disease (15 ). The aim of the present study was to evaluate if combined measurement of NT-proBNP and high-sensitivity cardiac troponin T (hs-cTnT) provides useful prognostic information in an elderly population with symptoms associated with heart failure in primary healthcare. Materials and Methods PATIENT POPULATION We evaluated elderly patients with symptoms associated with heart failure seen in the primary healthcare setting. The design of the study has already been published (21 ). In brief, all patients (n ⫽ 470) were between 65 and 87 years of age. All patients contacted the primary health center because of symptoms (tiredness, dyspnea, peripheral edema, or multiple symptoms). A cardiologist visited the health center and reviewed all records of patients with the above-listed symptoms. The cardiologist met with the patients, performed a clinical examination, and established a new patient record. Patients in whom heart failure could not be excluded were invited to participate in the study. All patients included in the study were enrolled in 1996. A new record was created and a clinical examination was carried out for each patient. We evaluated the New York Heart Association (NYHA) functional class, performed Doppler echocardiography, and took blood samples. No patients were lost during follow-up, and all patient deaths were recorded. The regional ethical review board in Linköping approved the study protocol. DEFINITIONS Cardiovascular mortality was defined as death caused by heart failure, and/or fatal arrhythmia, sudden death, ischemic heart disease, or cerebrovascular disease. Diabetes mellitus was defined as having a fasting blood glucose ⬎7.0 mmol/L or already undergoing treatment for diabetes (diet, oral therapy, or insulin). Hypertension was defined as a resting blood pressure ⬎140/90 mmHg, as measured in the right arm or having a prior diagnosis of hypertension. Ischemic heart disease was defined as a history of angina pectoris and/or treatment for ischemic symptoms or on the basis of verified pre- vious myocardial infarction. Dyspnea was defined from the patient history, whereas presence of peripheral edema was defined from patient history and/or clinical examination. ECHOCARDIOGRAPHY Doppler echocardiographic examinations (Acuson XP-128c) were performed with the patient in the supine left position. Values for left ventricular systolic function (22 ), expressed as ejection fraction (EF), were categorized into 4 classes with interclass limits of 30%, 40%, and 50% (23, 24 ). Normal systolic function was defined as EF ⱖ50%. Severely impaired systolic function was defined as EF ⬍30%. BLOOD SAMPLES The blood samples were obtained while the patients were at rest in a supine position. All blood samples were collected in plastic vials containing EDTA (ethylenediamine tetracetic acid). The samples were then placed on ice before chilled centrifugation at 3000g and frozen at ⫺70 °C, the temperature at which all samples were kept until final analysis. The samples were only thawed once (1997) before analyses of hs-cTnT (2009); in total, there were 2 freeze-thaw cycles for the samples used in this study. NT-proBNP AND hs-cTnT ANALYSES ProBNP 1–76 (NT-proBNP) was measured on the Elecsys 2010 (Roche Diagnostics). This assay uses 2 polyclonal antibodies directed against amino acid sequences 1–21 and 39 –50, respectively. Total assay CV was 4.8% at 220 ng/L and 2.1% at 4254 ng/L (n ⫽ 70). hs-cTnT was also measured on the Elecsys 2010 platform using a new assay from Roche. This assay measures human troponin by using monoclonal antibodies against amino acids 125–131 and 136 –147, respectively. The assay working range is reported as 3–10 000 ng/L, with an interassay CV according to the manufacturer of 3.1% at 24 ng/L and 1.3% at 300 ng/L. The lower limit of quantification is 13 ng/L, the lowest limit of detection is ⬍5 ng/L, and the limit of the blank is ⬍3 ng/L, as listed by the manufacturer. The 99th percentile concentration limits as established in a healthy population were used for assay interpretation, and we adopted the sex-specific 99th percentile limits reported by Mingels et al. (males ⬎18 ng/L; females ⬎8 ng/L) in our analyses (25 ). STATISTICAL ANALYSES Descriptive data are presented as percentages or mean and SD. In the case of continuous variables, comparative analyses were performed by using the Student unpaired 2-sided t-test, whereas the 2 test was used for discrete variables. Correlation was evaluated by using Clinical Chemistry 56:11 (2010) 1719 the Pearson product–moment correlation coefficient. Cox proportional hazard regression analyses as well as a Kaplan–Meier analysis were used to analyze the risk of mortality during the follow-up period. Censored patients were patients who were still alive at the end of the study period or who had died of causes other than cardiovascular disease. Completed patients comprised those who had died from cardiovascular disease. A P value ⬍0.05 was considered statistically significant. To evaluate the possible additive prognostic effects of biomarkers in multivariate analysis, weighted variables, obtained by summing each variable value in the multivariate setting multiplied by the  coefficients of the multivariate Cox proportional hazard regression function determined for each variable set, were analyzed by ROC analysis using the method of DeLong et al. (26 ). All data were analyzed by using standard software packages (Statistica v. 9.1, Statsoft; Analyse-it v.2.21, Analyse-it Software). Table 1. Baseline characteristics of the study population.a n 1720 Clinical Chemistry 56:11 (2010) 73 (5.6) M/F 242/228 Body mass index, mean (SD) 27 (4.3) History Smokers 151 (32) Diabetes 100 (21) Hypertension 412 (88) NYHA class I 213 (45) NYHA class II 204 (43) NYHA class III 53 (11) Medication Results In the study population, there was an approximately equal distribution of sexes (245 men vs 225 women): 20% of study participants had diabetes and almost 90% had been diagnosed with hypertension according to present guidelines (Table 1). The total study population was followed for 10 years (mean 3199 days, SD 1094). The cause of death was determined by autopsy in 10 patients; information given in the death certificates issued by the physician(s) in charge of the patient was used to establish cause of death for all other cases. Patients who survived during the follow-up period were observed during a mean observation period of 3465 days (SD 796), and those who did not survive the full 10 years were observed during a mean follow-up period of 2027 days (SD 1080). During the 10-year follow-up, 177 patients suffered all-cause mortality (37%) and 119 patients suffered a cardiovascular death (25%). There was a significant but poor correlation between hs-cTnT and NT-proBNP concentrations (r ⫽ 0.22, P ⬍ 0.0001). When examining only patients with left ventricular dysfunction (e.g., EF ⬍40%), a higher correlation (r ⫽ 0.42, P ⬎ 0.0001) was seen. In the total cohort, 378 patients (80.4%) had a plasma hs-cTnT concentration above the lower detection limit (5 ng/L). A difference between male and females patients was observed for hs-cTnT concentrations (males: mean 16 ng/L, females: mean 11 ng/L; t ⫽ 2.59, P ⫽ 0.03). In patients with a plasma hs-cTnT concentration above the 99th percentile of a healthy population, 43% (74/172) also displayed a plasma NTproBNP concentration in the fourth quartile. The different quartiles of hs-cTnT and NT-proBNP are 470 Age, mean (SD) Angiotensin-converting enzyme inhibitors 156 (33)  receptor blocker 189 (40) Digitalis 47 (10) Diuretics 207 (44) Examinations Increased cardio-thoracic ratio EF ⬍40% a b 207 (44) 55 (12) eGFRb ⬍60, mL 200 (42) NT-proBNP, ng/L 220 (0–18 707) hs-cTnT, ng/L 9.33 (3.0–220.3) Data are n (%) or median (range) unless otherwise indicated. eGFR, estimated glomerular filtration rate [Modification of Diet in Renal Disease (MDRD) formula]. shown in Table 2. Of those in the first quartile of hscTnT, 10% had died of CV mortality and 11% in the corresponding group of NT-proBNP. In the fourth quartiles, the corresponding figures were 45% and 53% for hs-cTnT and NT-proBNP, respectively. Among patients presenting with symptoms of heart failure and left ventricular dysfunction (EF ⬍40%), 61.8% (34/55) had a plasma hs-cTnT concentration above the 99th Table 2. The different quartiles of hs-cTnT and NT-proBNP. Hs-cTnT cutoff value, ng/L NT-proBNP cutoff value, ng/L Quartile 1 ⬍5.69 ⬍110 Quartile 2 5.69–9.33 110–220 Quartile 3 9.33–15.3 220–507 Quartile 4 ⬎15.3 ⬎507 hs-cTnT and NT-proBNP in Heart Failure percentile, and 67.3% (37/55) displayed a plasma NTproBNP concentration in the fourth quartile. Cardiovascular mortality was evaluated in the entire study population; the results are presented in Kaplan–Meier analyses in Fig. 1. Of patients who died from cardiovascular disease during the follow-up period, 60.5% had plasma hs-cTnT concentrations ⬎99th percentile. Regarding the NT-proBNP concentrations, 52.5% of patients with plasma NT-proBNP concentrations in the fourth quartile suffered a cardiovascular death compared with 10.9% among patients with a plasma concentration in the first quartile. When combining the 2 biomarkers in patients with a plasma hs-cTnT concentration ⬎99th percentile and a plasma NT-proBNP concentration in the fourth quartile, 62.2% had died a cardiovascular death during the follow-up period. The results of cardiovascular mortality based on quartiles of the biomarkers are presented in Tables 2 and 3. In the univariate Cox proportional hazard regression comparing concentrations above and below the cutoff, a 3.5- to 4.5-fold increased risk was indicated by either of the biomarkers. When comparing patients in whom both biomarkers were above the threshold with patients in whom both biomarkers were below the threshold, a 5-fold increase in the risk of cardiovascular mortality was seen (Table 3). In the multivariate Cox regression, both hs-cTnT and NTproBNP concentrations above the cutoff indicate more than 2 times the increased risk of cardiovascular mortality. However, combining the 2 biomarkers and analyzing those patients in whom both biomarkers were above the cutoff values increased the risk by a factor 3 (Table 4). A ROC analysis was also performed by using a 3-step model; step 1 consisted of clinical variables only (symptoms: tiredness, dyspnea, previous or present ischemic heart disease, diabetes, NYHA functional class III, male sex, age 70 –75 or ⬎75 years; signs: rales, jugular distension, peripheral edema). Step 2 consisted of clinical variables plus NT-proBNP concentrations, and step 3 included clinical variables plus NT-proBNP ⫹ hs-cTnT measurement. A difference in area under the curve (AUC) values between model step 1 (AUC 0.78) and step 3 (AUC 0.84) (95% CI 0.01– 0.10, P ⫽ 0.009) could be shown. Discussion There is now solid evidence that measurement of cardiac-derived natriuretic peptides and their biosynthetic precursors are useful in the evaluation of patients with heart failure. By comparison, cardiac troponins have a central role in diagnosing patients with acute coronary syndromes. Recent data suggest that troponin measurement may have prognostic value, even in heart failure patients who otherwise do not display Fig. 1. A Kaplan–Meier analysis illustrating the survival from cardiovascular mortality in the study population during 10 years of follow-up. The population was subdivided as follows: (A) NT-proBNP quartiles (quartile 3 vs quartile 4: P ⬍ 0.0001); (B) 99th percentile of hs-cTnT (hs-cTnT ⬍99% vs hs-cTnT ⬎99%: P ⬍ 0.0001); and (C) NT-proBNP quartiles and 99th percentile of hs-cTnT. Group 1: NT-proBNP ⬍ quartile 4, hs-cTnT ⬍99th percentile; group 2: NT-proBNP in quartile 4, hs-cTnT ⬍99th percentile; group 3: NT-proBNP ⬍ quartile 4, hs-cTnT ⬎99th percentile; group 4: NT-proBNP in quartile 4, hs-cTnT ⬎99th percentile. Clinical Chemistry 56:11 (2010) 1721 Table 3. Cardiovascular mortality in different patient groups depending on concentration of NT-proBNP or hs-cTnT. a Univariate Cox proportional hazard regression analysis, hazard ratio (95% CI) P Cardiovascular mortality, % NT-proBNP in quartile 4 (⬎507 ng/L) vs NT-proBNP ⱕ507 ng/L 4.31 (3.00–6.18) ⬍0.0001; 2: 61.8 52.5 vs 16.2 hs-cTnT ⬎99% gender specific vs hs-cTnT ⬍99% gender specifica 3.15 (2.18–4.55) ⬍0.0001; 2: 39.3 41.9 vs 15.8 Both NT-proBNP in quartile 4 (⬎507 ng/L) ⫹ hs-cTnT ⬎99% gender specific vs NT-proBNP ⱕ507 ng/L ⫹ hs-cTnT ⬍99% gender specifica 4.70 (3.25–6.81) ⬍0.0001; 2: 63.1 62.2 vs 18.4 hs-cTnT 99% gender specific: male patients: 18 ng/L, female patients 8 ng/L. symptoms of ischemic heart disease (27 ). With the introduction of high-sensitivity assays, this perspective can now be tested. We therefore evaluated the use of NT-proBNP and hs-cTnT measurement and the possible benefit of using additive prognostic information concerning cardiovascular mortality in a primary healthcare population. In the study population, a substantial fraction displayed plasma hs-cTnT concentrations above the lowest level of detection, even in the absence of ischemic heart disease symptoms. This finding resembles earlier results (28, 29 ). By using the less-sensitive assays in the earlier studies, however, only a small part of the heart failure population displayed plasma cTnT concentrations above the lower limit of detection. By using new assays with increased sensitivity, the cardiac troponin concentrations can now be determined at concentrations that may reflect discrete/early myocardial damage (30 ). Whether presence of the cardiac troponins in plasma is due to cardiomyocyte apoptosis or is a consequence of other pathophysiological processes still remains to be determined (14 ). Sex-specific cutoff values have also been reported, where male patients have higher concentrations values compared with female patients (25, 30 ). The precise sex differences still need to be examined in reference individuals Table 4. Cox proportional regression hazard analyses including clinical variables influencing cardiovascular mortality in an elderly population followed for 10 years. Hazard ratio Model I, 95% CI P Hazard ratio Age ⬎75 years 1.69 1.14–2.52 0.009 1.84 1.24–2.73 0.002 1.69 1.13–2.54 0.01 Male sex 1.52 1.02–2.26 0.04 1.72 1.14–2.58 0.01 1.60 1.08–2.39 0.02 NYHA III 1.96 1.22–3.15 0.005 2.42 1.52–3.86 0.0002 2.33 1.45–3.75 0.0005 EF ⬍40% 1.55 0.96–2.50 0.07 2.04 1.29–3.22 0.002 1.63 1.01–2.64 0.05 Ischemic heart disease 0.82 0.55–1.20 0.31 0.91 0.62–1.33 0.62 0.83 0.56–1.22 0.34 Body mass index ⬎27 kg/m 2 Model II, 95% CI P Hazard Model III, ratio 95% CI P 1.12 0.76–1.67 0.56 1.10 0.74–1.63 0.63 1.17 0.79–1.74 0.43 eGFRa ⬍60 mL 1.38 0.92–2.08 0.12 1.22 0.80–1.84 0.36 1.29 0.85–1.95 0.24 Diabetes 2.15 1.43–3.24 0.0002 1.71 1.13–2.58 0.01 2.02 1.35–3.03 0.0007 Hemoglobin ⬍120 g/L 1.80 0.97–3.35 0.06 1.52 0.81–2.83 0.19 1.54 0.83–2.86 0.18 NT-proBNP in quartile 4 (⬎507 ng/L) 2.56 1.95–4.49 ⬍0.0001 — — — — — — hs-cTnT ⬎99% — — — 2.24 NT-proBNP in quartile 4 ⫹ hs-cTnT ⬎99% — — — — a — — 1.46–3.43 0.0002 — — 3.09 2.00–4.79 ⬍0.0001 eGFR, estimated glomerular filtration rate [Modification of Diet in Renal Disease (MDRD) formula]. hs-cTnT ⬎99%: sex-specific 99th percentile cutoffs in a healthy population (males: 18 ng/L; females: 8 ng/L) were used in our study. NT-proBNP quartile 4: We used a lower-boundary concentration for the fourth quartile of the plasma concentration of NT-proBNP (507 ng/L) as a cutoff in the study population. Model I: Clinical variables analyzed together with the fourth quartile of NT-proBNP. Model II: Various clinical variables analyzed together with the 99th sex-specific hs-cTnT percentile. Model III: Various clinical variables analyzed together with the fourth quartile of NT-proBNP ⫹ 99th sex-specific hs-cTnT percentile at the same time. 1722 Clinical Chemistry 56:11 (2010) hs-cTnT and NT-proBNP in Heart Failure (i.e., not patients), but the difference was nevertheless noted also in this study. Whether minor myocardial damage takes place in heart failure patients has recently been discussed by Latini and Masson (9 ). The Kaplan–Meier analysis of the proportion of cardiovascular mortality of the 2 biomarkers supports this (Fig. 1). However, the underlying pathophysiology of low plasma troponin T concentrations during heart failure still deserves to be explored further. Notably, the heart failure syndrome constitutes more than reduced ejection fraction of the left ventricle, including changes in renal function and other organs. Both the univariate and multivariate Cox regression show that the prognostic information concerning risk of cardiovascular death by use of hs-cTnT is as reliable as NT-proBNP (Tables 3 and 4). Combining the 2 biomarkers may further improve the identification of patients with increased myocardial wall tension and minor myocardial damage, even in the absence of ischemic symptoms. In both the univariate and multivariate evaluations, the increased risk was detected even with the long observation time. Notably, a long follow-up period often results in reduced importance of cardiovascular events, since other conditions gain a greater influence on total mortality (Table 4). In the ROC analysis, the additive information from using both biomarkers was significant and suggests a combined use of 2 biomarkers in clinical practice. The Cox proportional hazard regression analysis also showed additive information by using both markers (hazard ratio increased from 2- to 3-fold). The Val-Heft study reported similar results in terms of additive prognostic information by using hscTnT measurement and a natriuretic peptide (14 ). However, there are several important differences between that study and ours. First, the mean age of the study population was ⬎10 years older than the population in the Val-Heft study. Second, there were unequal proportions of men and women in the Val-Heft study that were not present in our study. Third, the mean EF in the Val-Heft study was 27%, whereas the majority of individuals in our population did not display impaired cardiac function according to Doppler echocardiography. Fourth, in the Val-Heft study, the natriuretic peptide assay used was BNP by a manual indirect method (Shionogi, Shionoria assay), whereas we used NT-proBNP. Fifth, the Val-Heft study used the median as a cutoff, whereas we used the presently recommended cutoff for diagnosing myocardial damage (i.e., the 99th percentile) (31 ). Consequently, our cohort conforms better with the everyday clinical population. Finally, the patients identified by use of the combined biomarker approach represent a high-risk population (Fig. 1C). These patients should therefore be handled as such, which suggests the use of a heart failure outpatient clinic with a more aggressive treatment regimen (32 ). The choice of cutoff values of NTproBNP is based on the plasma concentration in the study population. However, the fourth quartile of NTproBNP (⬎507 ng/L) is not far from the guidelines on how to diagnose heart failure given by the European Society of Cardiology, where a plasma concentration ⬎400 ng/L could be regarded as “uncertain diagnosis,” and a concentration ⬎2000 ng/L gives the diagnosis “chronic heart failure likely” if there are signs and symptoms of heart failure (33 ). This could indicate that the evaluated study population is representative of the patients with signs/symptoms found in the community. Our study presents data that are based on community-living elderly patients, i.e., the group seen most frequently by clinicians in daily practice. In the literature, the vast majority of studies report on a different age-group than the one that is most usually encountered in patients with heart failure in the community. Our study conforms better in this regard. We have shown that hs-cTnT is a powerful prognostic indicator for CV mortality among individuals with symptoms associated with heart failure, even without overt ischemic symptoms. When the 2 biomarkers hs-cTnT and NT-proBNP are combined, more information becomes available from this patient group, who often has many comorbidities. Author Contributions: All authors confirmed they have contributed to the intellectual content of this paper and have met the following 3 requirements: (a) significant contributions to the conception and design, acquisition of data, or analysis and interpretation of data; (b) drafting or revising the article for intellectual content; and (c) final approval of the published article. Authors’ Disclosures of Potential Conflicts of Interest: Upon manuscript submission, all authors completed the Disclosures of Potential Conflict of Interest form. Potential conflicts of interest: Employment or Leadership: None declared. Consultant or Advisory Role: None declared. Stock Ownership: None declared. Honoraria: None declared. Research Funding: Grants from the County Council of Östergötland, The Swedish Heart and Lung Foundation, and the strategic research area “Inflammation, atherosclerosis and ischemic heart disease—new strategies for prevention, diagnosis and treatment,” which is sponsored by the County Council of Östergötland and the University of Linköping. Expert Testimony: None declared. Role of Sponsor: The funding organizations played no role in the design of study, choice of enrolled patients, review and interpretation of data, or preparation or approval of manuscript. Acknowledgments: We thank laboratory technicians Lone Olsen and Jan Kirkeby Simonsen for laboratory assistance with the highsensitivity troponin T measurements. Clinical Chemistry 56:11 (2010) 1723 References 1. van Veldhuisen DJ, Boomsma F, de Kam PJ, Man in’t Veld AJ, Crijns HJ, Hampton JR, Lie KI. Influence of age on neurohormonal activation and prognosis in patients with chronic heart failure. Eur Heart J 1998;19:753– 60. 2. Johnson W, Omland T, Hall C, Lucas C, Myking OL, Collins C, et al. Neurohormonal activation rapidly decreases after intravenous therapy with diuretics and vasodilators for class IV heart failure. J Am Coll Cardiol 2002;39:1623–9. 3. Davis CJ, Gurbel PA, Gattis WA, Fuzaylov SY, Nair GV, O’Connor CM, Serebruany VL. Hemostatic abnormalities in patients with congestive heart failure: diagnostic significance and clinical challenge. Int J Cardiol 2000;75:15–21. 4. Strassburg S, Anker SD. Metabolic and immunologic derangements in cardiac cachexia: where to from here? Heart Fail Rev 2006;11:57– 64. 5. Sharma R, Coats AJ, Anker SD. The role of inflammatory mediators in chronic heart failure: cytokines, nitric oxide, and endothelin-1. Int J Cardiol 2000;72:175– 86. 6. Vasan RS, Sullivan LM, Roubenoff R, Dinarello CA, Harris T, Benjamin EJ, et al. Inflammatory markers and risk of heart failure in elderly subjects without prior myocardial infarction: the Framingham Heart Study. Circulation 2003;107: 1486 –91. 7. Vila V, Martinez-Sales V, Almenar L, Lazaro IS, Villa P, Reganon E. Inflammation, endothelial dysfunction and angiogenesis markers in chronic heart failure patients. Int J Cardiol 2008;130: 276 –7. 8. von Haehling S, Schefold JC, Lainscak M, Doehner W, Anker SD. Inflammatory biomarkers in heart failure revisited: much more than innocent bystanders. Heart Fail Clin 2009;5:549 – 60. 9. Latini R, Masson S. Biomarkers of myocyte injury in heart failure. Heart Fail Clin 2009;5:529 –36. 10. Gupta S, Drazner MH, de Lemos JA. Newer biomarkers in heart failure. Heart Fail Clin 2009;5: 579 – 88. 11. Sudoh T, Kangawa K, Minamino N, Matsuo H. A new natriuretic peptide in porcine brain. Nature 1988;332:78 – 81. 12. Heeschen C, Goldmann BU, Terres W, Hamm CW. Cardiovascular risk and therapeutic benefit of coronary interventions for patients with unstable angina according to the troponin T status. Eur Heart J 2000;21:1159 – 66. 13. Quenot JP, Le Teuff G, Quantin C, Doise JM, Abrahamowicz M, Masson D, Blettery B. Myocar- 1724 Clinical Chemistry 56:11 (2010) 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. dial injury in critically ill patients: relation to increased cardiac troponin I and hospital mortality. Chest 2005;128:2758 – 64. Latini R, Masson S, Anand IS, Missov E, Carlson M, Vago T, et al. Prognostic value of very low plasma concentrations of troponin T in patients with stable chronic heart failure. Circulation 2007;116:1242–9. Omland T, de Lemos JA, Sabatine MS, Christophi CA, Rice MM, Jablonski KA, et al. A sensitive cardiac troponin T assay in stable coronary artery disease. N Engl J Med 2009;361:2538 – 47. Fernandes CJ Jr, Akamine N, Knobel E. Myocardial depression in sepsis. Shock 2008;30(Suppl 1):14 –7. Aujesky D, Hughes R, Jimenez D. Short-term prognosis of pulmonary embolism. J Thromb Haemost 2009;7(Suppl 1):318 –21. Lega JC, Lacasse Y, Lakhal L, Provencher S. Natriuretic peptides and troponins in pulmonary embolism: a meta-analysis. Thorax 2009;64:869 – 75. Zairis MN, Tsiaousis GZ, Georgilas AT, Makrygiannis SS, Adamopoulou EN, Handanis SM, et al. Multimarker strategy for the prediction of 31 days cardiac death in patients with acutely decompensated chronic heart failure. Int J Cardiol 2010; 141:284 –90. Peacock WF, De Marco T, Fonarow GC, Diercks D, Wynne J, Apple FS, Wu AH. Cardiac troponin and outcome in acute heart failure. N Engl J Med 2008;358:2117–26. Alehagen U, Eriksson H, Nylander E, Dahlström U. Heart failure in the elderly: characteristics of a Swedish primary health care population. Heart Drug 2002;2:211–20. Choy AM, Darbar D, Lang CC, Pringle TH, McNeill GP, Kennedy NS, Struthers AD. Detection of left ventricular dysfunction after acute myocardial infarction: comparison of clinical, echocardiographic, and neurohormonal methods. Br Heart J 1994;72:16 –22. Jensen-Urstad K, Bouvier F, Hojer J, Ruiz H, Hulting J, Samad B, et al. Comparison of different echocardiographic methods with radionuclide imaging for measuring left ventricular ejection fraction during acute myocardial infarction treated by thrombolytic therapy. Am J Cardiol 1998;81: 538 – 44. van Royen N, Jaffe CC, Krumholz HM, Johnson KM, Lynch PJ, Natale D, et al. Comparison and reproducibility of visual echocardiographic and 25. 26. 27. 28. 29. 30. 31. 32. 33. quantitative radionuclide left ventricular ejection fractions. Am J Cardiol 1996;77:843–50. Mingels A, Jacobs L, Michielsen E, Swaanenburg J, Wodzig W, van Dieijen-Visser M. Reference population and marathon runner sera assessed by highly sensitive cardiac troponin T and commercial cardiac troponin T and I assays. Clin Chem 2009;55:101– 8. DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics 1988;44: 837– 45. Ilva T, Lassus J, Siirila-Waris K, Melin J, Peuhkurinen K, Pulkki K, et al. Clinical significance of cardiac troponins I and T in acute heart failure. Eur J Heart Fail 2008;10:772–9. Daniels LB, Laughlin GA, Clopton P, Maisel AS, Barrett-Connor E. Minimally elevated cardiac troponin T and elevated N-terminal pro-B-type natriuretic peptide predict mortality in older adults: results from the Rancho Bernardo Study. J Am Coll Cardiol 2008;52:450 –9. Sundstrom J, Ingelsson E, Berglund L, Zethelius B, Lind L, Venge P, Arnlov J. Cardiac troponin-I and risk of heart failure: a community-based cohort study. Eur Heart J 2009;30:773– 81. Giannitsis E, Kurz K, Hallermayer K, Jarausch J, Jaffe AS, Katus HA. Analytical validation of a high-sensitivity cardiac troponin T assay. Clin Chem 2010;56:254 – 61. Dickstein K. ELITE II and Val-HeFT are different trials: together what do they tell us? Curr Control Trials Cardiovasc Med 2001;2:240 –3. Lainscak M, Cleland JG, Lenzen MJ, Follath F, Komajda M, Swedberg K. International variations in the treatment and co-morbidity of left ventricular systolic dysfunction: data from the EuroHeart Failure Survey. Eur J Heart Fail 2007;9:292–9. Dickstein K, Cohen-Solal A, Filippatos G, McMurray JJ, Ponikowski P, Poole-Wilson PA, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2008: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2008 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association of the ESC (HFA) and endorsed by the European Society of Intensive Care Medicine (ESICM). Eur J Heart Fail 2008;10:933– 89.