Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Idiopathic intracranial hypertension wikipedia , lookup
Fundus photography wikipedia , lookup
Mitochondrial optic neuropathies wikipedia , lookup
Visual impairment due to intracranial pressure wikipedia , lookup
Photoreceptor cell wikipedia , lookup
Optical coherence tomography wikipedia , lookup
Diabetic retinopathy wikipedia , lookup
Macular degeneration wikipedia , lookup
Retinal waves wikipedia , lookup
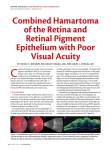
SHORT COMMUNICATION ARCH SOC ESP OFTALMOL 2008; 83: 193-196 COMBINED HAMARTOMA OF THE RETINA AND RETINAL PIGMENT EPITHELIUM DIAGNOSED BY RETINAL ANGIOGRAPHY AND OPTICAL COHERENCE TOMOGRAPHY HAMARTOMA COMBINADO DE RETINA Y EPITELIO PIGMENTARIO RETINIANO. DIAGNÓSTICO MEDIANTE TOMOGRAFÍA DE COHERENCIA ÓPTICA Y ANGIOFLUORESCEINGRAFÍA PÉREZ-ÁLVAREZ MJ1, ALEJANDRE-ALBA N1, GARCÍA-SÁNCHEZ J2 ABSTRACT RESUMEN Clinical case: This report is based on the case of a 35-year-old woman who developed a combined hamartoma of the retina and retinal pigment epithelium in her right eye. The diagnosis was determined based on the fundus examination: hyperplasia of the retinal pigment epithelium cells, tortuosity of the vessels and epiretinal membrane. Discussion: Optical coherence tomography and retinal angiography are important to rule out malignant melanoma of the choroid and retinoblastoma. Regular follow-up is essential because reduction in visual acuity can be related to an epiretinal membrane, neovascular membrane or vitreous hemorrhage (Arch Soc Esp Oftalmol 2008; 83: 193-196). Caso clínico: Se presenta el caso de una paciente de 35 años, que desarrolló un hamartoma combinado de retina y epitelio pigmentado retiniano. El diagnóstico se determinó en base a los característicos hallazgos funduscópicos: hiperplasia del epitelio pigmentado retiniano, tortuosidad vascular y membrana epirretiniana. Discusión: La tomografía de coherencia óptica y la angiofluoresceingrafía permiten descartar melanoma coroideo o retinoblastoma. Es importante realizar un seguimiento periódico por la posibilidad de afectación visual por membrana neovascular coroidea, membrana epirretiniana o hemorragia vítrea. Key words: Hamartoma of the retina and retinal pigment epithelium, Optical coherence tomography. Palabras clave: Hamartoma combinado de retina y epitelio pigmentado retiniano, tomografía de coherencia óptica. Received: Sept. 15, 2006. Accepted: Feb. 18, 2008. San Carlos Clinical Hospital. Complutense University of Madrid. Madrid. Spain. 1 Graduate in Medicine. 2 Ph.D. in Medicine. Correspondence: María Jesús Pérez Álvarez Paseo de los Pontones, 5, 4.º Dcha. 28005 Madrid España E-mail: [email protected] PÉREZ-ÁLVAREZ MJ, et al. INTRODUCTION Combined Hamartomas of Retina and Retinal Pigment Epithelium (CHRRPE) are rare benign tumors characterized by the proliferation of retinal pigment epithelium (RPE) and glyal tissue, generating a large papillary and retinal distortion. A single unilateral over-elevated hyper-pigmented lesion is observed, accompanied by vascular tortuosity and epiretinal membrane (ERM). CASE REPORT This short communication presents the case of a 35 year-old woman who visited the practice due to miodesopsiae in the right eye (RE). The exploration evidenced a corrected visual acuity (VA) in both eyes of 1. No iridian nodules were observed in the anterior biomicroscopy. The tonometry gave normal results, while the funduscopy showed for the right eye a nasal, elevated and hyper pigmented peripapillary lesion, with telangectasic tortuous vessels and ERM, as well as peripapillary chorioretinal atrophy below the lesion (fig. 1). The periphery exhibited an area of vitreous traction, possibly the cause of the symptoms, which was photocoagulated with argon laser. The left eye produced normal results (fig. 2). The angiofluoresceingraph (AFG) showed a fluorescence interruption in early times and telangiectasic vessels with loss of contrast and slight tincture of the lesion in late times. No choroidal or retinal neovascularization signs were observed (fig. 3). The ocular echography did not reveal significant elevation of the lesion or signs suggesting choroidal melanoma. The Optical Coherence Tomography (OCT) showed a hyper-reflecting retinal elevation with underlying hypo-reflecting shadow and important distortion of the retinal architecture within the limits of the lesion, with clear ERM (figs. 4 and 5). The Humphrey 24-2 computerized perimetry showed that the lesion generated an absolute scotoma. With a suspected Combined Hamartoma of retina and retinal pigment epithelium (CHRRPE), the Fig. 1: RE funduscopy showing the characteristic elevated pigmented lesion with telangiectasic vessels. Fig. 3: Late times showing loss from telangiectasic dilatations and slight tincture of the lesion. 194 Fig. 2: LE funduscopy without alterations. ARCH SOC ESP OFTALMOL 2008; 83: 193-196 Retina and retinal pigment epithelium combined hamartoma Fig. 4 y 5: Optical Coherence Tomography showing the distortion of the retinal architecture, elevating hyper-reflecting lesion with pre-retinal membrane. patient was referred to internal medicine to discard associated diseases and a cranial and orbitary Nuclear Magnetic Resonance (NMR) was performed. The systemic studies produced normal results. After 6 months of evolution, the lesion remains stable without VA reduction or emergence of metamorphopsiae or other complications. DISCUSSION A hamartoma is a benign proliferation of cells which, in normal conditions, are in the same location, therefore the CHRRPE exhibits a malformation of the RPE, the neurosensory retina, vascularization and adjacent vitreous, in variable degrees. 93% of cases exhibit vascular tortuosity, 87% hyper-pigmentation, 80% elevated lesion, and 78% ERM. Usually these are single and unilateral lesions located close to the optic nerve (76%), in the macula (17%) or peripheral (7%) (1,2). 10% of cases constitute a casual finding, with the most frequent symptoms being the painless loss of VA (60%), while other expressions include strabismus (18%), miodesopsia (5%), leucochoria and pain (5%). The direct involvement of the fovea, the papillomacular line or the optic nerve are the most frequent causes of VA reduction, although it can also be caused by the traction caused by the ERM, and intra- or sub-retinal exudation from the vascular components of the lesion (2). In the majority of cases, the disease progression is stationary (2). However, on some occasions there may be late vision loss due to vitreous hemorrhage (VH), choroidal neovascular membrane (CNVM), chronic macular edema, progressive retinoschisis, macular hole, retina detachment (RD) and retinal neovascularization (1). The lesion will grow only exceptionally. As mentioned above, the diagnostic is based on funduscopy and confirmed with OCT and AFG (2,3). OCT is highly characteristic, with considerable distortion of all the structures, ERM and vitreoretinal traction. This test could be a tool for determining the usefulness of vitrectomy pars plana (VPP) with peeling of ERM in some cases (4). Echography is not always precise because the lesions are not very elevated and do not exhibit a typical ultrasound pattern. The differential diagnostic must be made with choroidal tumors and retinoblastoma (2,3), and the above mentioned tests are useful for this purpose. The majority of cases do not exhibit systemic expressions. The literature reports cases with type 1 and 2 neurofibromatosis, although this association is not yet clearly established. It can also be associated to facial hemangioma, pigment incontinence and tuberous sclerosis. Therefore, neuroimaging tests are not recommended (1). Most cases do not require treatment. Occlusion is recommended in children to prevent amblyopia. The indications for VPP are not yet fully established with regard to the peeling of ERM. The cases described in the literature exhibit different visual results. This controversy is due to the fact that, at the histological level, the lesion is intra-retinal and therefore improvements are evidenced only by the cases exhibiting clear vitreous traction (4). VPP would be indicated as treatment for the complications (VH, RD) with variable results for different authors (1.5). Some describe good visual results after submacular surgery as treatment for CNVM because these are located above the RPE (Gass type 2) (5). ARCH SOC ESP OFTALMOL 2008; 83: 193-196 195 PÉREZ-ÁLVAREZ MJ, et al. It can be concluded that, even though CHRRPE are benign tumors, an adequate differential diagnostic must be made by means of AFG and OCT, in addition to a regular follow-up due to the risk of losing VA on account of the associated complications such as ERM, CNVM, VH and RD. REFERENCES 1. Helbig H, Niederberger H. Presumed combined hamartoma of the retina and retinal pigment epithelium with preretinal neovascularization. Am J Ophthalmol 2003; 136: 1157-1159. 196 2. Hamdi R, De Korvin H, Speeg-Schatz C, Szwarcberg J. Combined hamartoma of the retina and retinal pigment epithelium. Four case studies. J Fr Ophtalmol 2006; 29: e6. 3. Shields CL, Materin MA, Shields JA. Review of optical coherence tomography for intraocular tumors. Curr Opin Ophthalmol 2005; 16: 41-54. 4. Stallman JB. Visual improvement after pars plana vitrectomy and membrane peeling for vitreoretinal traction associated with combined hamartoma of the retina and retinal pigment epithelium. Retina 2002; 22: 101-104. 5. Inoue M, Noda K, Ishida S, Yamaguchi T, Nagai N, Shinoda K, et al. Successful treatment of subfoveal choroidal neovascularization associated with combined hamartoma of the retina and retinal pigment epithelium. Am J Ophthalmol 2004; 138: 155-156. ARCH SOC ESP OFTALMOL 2008; 83: 193-196