Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
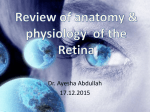
Heavy Metal Concentrations in Human Eyes JAY C. ERIE, MD, JOHN A. BUTZ, BA, JONATHAN A. GOOD, BS, ELIZABETH A. ERIE, BA, MARY F. BURRITT PHD, AND J. DOUGLAS CAMERON, MD ● PURPOSE: To measure the concentration of toxic heavy metals in the fluids and tissues of human eyes. ● DESIGN: Laboratory investigation. ● METHODS: Thirty autopsy eyes of 16 subjects were dissected to obtain the aqueous, vitreous, lens, ciliary body, retina, and retinal pigment epithelium/choroid. Concentrations of lead, cadmium, mercury, and thallium in ocular tissues, ocular fluids, and blood were determined using an inductively coupled plasma-mass spectrometer and expressed as ng/g. Heavy metal concentrations in ocular tissues were compared using a paired t test. ● RESULTS: Lead and cadmium were found in all of the pigmented ocular tissues studied, concentrating to the greatest extent in the retinal pigment epithelium/choroid (mean, 432 ⴞ 485 ng/g and 2,358 ⴞ 1,522 ng/g). Cadmium was found in the retina in all eyes (mean, 1,072 ⴞ 489 ng/g) whereas lead was found in the retina in 9 (30%) of 30 eyes (mean, 53 ⴞ 54 ng/g). Trace concentrations of lead and cadmium were detected in the vitreous (mean, 0.5 ⴞ 1.0 ng/dl and 19 ⴞ 29 ng/dl), lens (mean, 13 ⴞ 18 ng/g and 20 ⴞ 18 ng/g), and blood (mean, 0.5 ⴞ 1.2 g/dl and 3.1 ⴞ 4.1 g/l) but were not detected in the aqueous. Mercury and thallium were not detected in any ocular tissues or fluids or in the blood. ● CONCLUSIONS: Lead and cadmium accumulate in human ocular tissues, particularly in the retinal pigment epithelium and choroid. The potential ocular toxicity of these heavy metals and their possible role in eye disease requires further study. (Am J Ophthalmol 2005;139: 888 – 893. © 2005 by Elsevier Inc. All rights reserved.) H METHODS UMAN CELLS EMPLOY METALS, SUCH AS COPPER, zinc, and iron, to control significant metabolic and signaling functions making them essential for life. Other metals can be potentially toxic such as the heavy metals: lead, cadmium, mercury, and thallium. Lead, Accepted for publication Dec 3, 2004. From the Department of Ophthalmology (J.C.E., J.D.C., E.A.E.) and Metals Laboratory (J.A.B., J.A.G, M.F.B) Mayo Clinic and Mayo Clinic College of Medicine, Rochester, Minnesota. Supported by Research to Prevent Blindness, New York, New York and the Mayo Foundation, Rochester, Minnesota. Inquiries to Jay C. Erie, MD, Mayo College of Medicine, 200 1st Street SW, Rochester, MN 55905; fax: 507-284-4612; e-mail: [email protected] 888 in particular, is a neurotoxin that has been linked to visual deterioration,1 central and peripheral nervous system disorders,2 renal dysfunction,3 and hypertensive cardiovascular disease.4 Cadmium toxicity has been associated with renal disease, hypertension, and an increased prevalence of cardiovascular disease.5 Heavy metals are ubiquitous pollutants that have permanently contaminated air, water, and soil. The toxic effect of heavy metals usually involves an interaction between the heavy metal ion and the specific target protein, resulting in a change in protein structure and function.6 Cells involved in the transport of trace metals are particularly susceptible to toxicity. The retinal pigment epithelium is a metal-chelating tissue that is capable of binding essential and toxic heavy metals because of the high affinity of metals to melanin in retinal pigment epithelium melanosomes.7,8 Recently, Eichenbaum and Zheng9 showed that the retina and choroid can accumulate the heavy metal, lead. Blood and urine samples reflect the amount of metals circulating at the time of sampling and do not represent the cumulative degree of exposure. Tissue biopsies for elemental analysis can aid in identifying the accumulation of metals from chronic exposure.10,11 At present, data on heavy metal concentrations and distribution in human eyes are limited.7,9 The purpose of our study was to measure the concentrations and establish a reference range of toxic heavy metals (lead, cadmium, mercury, and thallium) in the fluids and tissues of eyes. © 2005 BY ● SAMPLE COLLECTION: Eye tissue and blood were collected at the time of autopsy according to a protocol reviewed and approved by the Mayo Foundation Institutional Review Board. This study was a laboratory investigation. Thirty eyes from 16 subjects (10 men, 6 women) aged 62 to 94 years (mean, 78 ⫾ 9 years) were prospectively analyzed. In two randomly selected subjects, one eye was dissected and sent for metal analysis and the fellow eye was dissected and sent for histologic examination. All subjects were Caucasian. Based on autopsy findings, eye dissection findings, and review of medical history, subjects were excluded if they had previous ocular trauma, intraoc- ELSEVIER INC. ALL RIGHTS RESERVED. 0002-9394/05/$30.00 doi:10.1016/j.ajo.2004.12.007 TABLE 1. Eye Concentrations of Lead and Cadmium Lead Dry Weight (ng/g) Aqueous Vitreous Lens Ciliary body RPE/Choroid Retina Cadmium Wet Weight (ng/g or ng/dL)* Dry Weight (ng/g) Wet Weight (ng/g or ng/dL)* Mean ⫾ SD Range Mean ⫾ SD Range Mean ⫾ SD Range Mean ⫾ SD Range 13 ⫾ 18 321 ⫾ 127 432 ⫾ 485 53 ⫾ 54 0–97 127–464 29–2,165 0–172 0 0.5 ⫾ 1.0 4⫾4 73 ⫾ 70 82 ⫾ 109 5⫾7 0 0.0–3.5 0–13 27–175 6–378 0–27 20 ⫾ 18 1,012 ⫾ 1,464 2,358 ⫾ 1,522 1,072 ⫾ 489 0–50 220–3,495 407–4,846 130–1,624 0 21 ⫾ 34 5⫾5 109 ⫾ 70 298 ⫾ 165 82 ⫾ 60 0 0–123 0–16 53–201 74–731 5–212 * ⫽ Units for aqueous and vitreous are expressed as ng/dL wet weight only. Units for lens, ciliary body, RPE/choroid, and retina are expressed as ng/g for dry and wet weight; n ⫽ 16 (30 eyes) for vitreous, RPE/choroid, and retina; n ⫽ 8 (9 eyes) for ciliary body and lens; n ⫽ 5 (5 eyes) for aqueous. ular tumor, glaucoma, diabetes mellitus, exudative macular degeneration, corneas suitable for corneal transplantation, or any systemic disease or occupation likely to cause aberration in metal content. Eyes with macular drusen were included. All samples were collected, refrigerated, and processed within 11 hours after death (5.9 ⫾ 3.6 hours). Aqueous aspirates were obtained through a clear cornea stab incision with a 30-gauge needle on a tuberculin syringe. The anterior segment was dissected from the posterior segment using a scissors and a fine-toothed forceps. The crystalline lens, if present, and the ciliary body were detached and removed separately. In some cases, the anterior segment was used for glaucoma research and the aqueous, lens, and ciliary body were not available. Vitreous aspirates from all specimens were collected with an 18-gauge needle in an “open-sky” fashion. The retina and choroid complex were isolated and removed separately using a fine-toothed forceps and scissors. The entire dissection procedure was completed within 15 minutes. All samples were placed in separate labeled, acid-washed, metal-free plastic containers (Sarstedt Inc., Newton, North Carolina, USA) for transport to the metals laboratory. Blood was obtained from the femoral vein directly into a metal-free EDTA tube. The cause of death of the subjects were as follows: six acute myocardial/cardiac arrest, three acute respiratory distress, two pancreatic cancer, one trauma, one lymphoma, one leukemia, one pneumonia, one perforated bowel. Occupations included: five housewives, four farmers, two office workers, two teachers, one attorney, one construction worker, and one telephone operator. ● FRESH TISSUE PREPARATION AND DIGESTION: Each tissue was placed into a preweighed Teflon digestion tube. The sample was weighed to determine a wet weight (grams) and then dried at 95 C overnight. The sample was then reweighed the next day to determine the dry weight (grams). Concentrated trace metals grade nitric acid (0.5 ml) was VOL. 139, NO. 5 added to the digest tube. The tube was placed in a Teflon heating mantel, and the sample was digested at 95 C for approximately 1 hour until all tissue material has been dissolved. 3.5 milliliters of reagent grade water was added to each tube. This digest mixture was then thoroughly vortexed. Two deviations from this procedure were considered acceptable: (1) aqueous, vitreous, and blood were processed strictly on a wet weight basis, and (2) the amount of acid and water used for the digestion was sometimes adjusted for extremely small weights or incomplete digestions. ● MASS SPECTROMETRY ANALYSIS: All four elements (lead, cadmium, mercury, and thallium) were analyzed simultaneously on a PE/SCIEX Elan 6100 inductively coupled plasma-mass spectrometer (Perkin Elmer Life & Analytical Sciences, Shelton, Connecticut, USA). Aqueous acidic calibrating standards were diluted with an aqueous acidic diluent (2% hydrochloric acid, 2.5% tertiary butanol, and 1 g/l gold) containing three internal standards (bismuth, gallium, and rhodium). Blanks, quality control specimens, and digested samples were also diluted in an identical manner. All samples were vortexed and aspirated into a pneumatic nebulizer. The resulting aerosol was directed to the hot plasma discharge by a flow of argon. Instrumentation response was defined by the linear relationship of analyte concentration vs ion counts (analyte ion count/internal standard ion count). Analyte concentrations were derived by reading the ion count ratio for each mass of interest. The concentration of the digest was used to calculate the concentration of metal in the tissue as a dry and wet weight and expressed as ng/g. Subsequent analysis and discussion is based on tissue concentrations as a dry weight, as this avoids potential errors attributable to tissue hydration and allows for future comparisons with formalin-fixed (that is, partially dehydrated) concentrations.10 ● TISSUE ANALYSIS AND ASSAY TECHNIQUE: The assay used to quantitate metal concentrations in the tissue digests is routinely employed to perform the same analysis HEAVY METAL CONCENTRATIONS IN HUMAN EYES 889 TABLE 2. Cadmium and Lead Concentrations (mean ⫾ SD, g/g) in Smokers vs Non-smokers Cadmium RPE/Choroid Retina Lead Smoker* Non-smoker† P‡ Smoker* Non-smoker† P‡ 4,029 ⫾ 1,819 1,498 ⫾ 528 1,652 ⫾ 845 932 ⫾ 423 .004 .002 367 ⫾ 210 39 ⫾ 39 286 ⫾ 196 49 ⫾ 63 .56 .62 *n ⫽ 5 subjects (9 eyes). † n ⫽ 10 subjects (19 eyes); the smoking status of 1 subject (two eyes) was unknown, and these eyes were excluded from analysis. ‡ 2-sample t-test. above the normal adult range (⬍5 g/l); 2 of the 3 subjects were smokers. No subjects had detectable blood levels of mercury and thallium. Table 1 shows the concentrations and reference ranges for lead and cadmium in the fluids and tissues of fresh autopsy human eyes. No mercury or thallium was detected in any of the ocular tissues or fluids. Cadmium and lead were found in all of the pigmented ocular tissues (e.g., retinal pigment epithelium/choroid, ciliary body) studied but concentrated to the greatest extent in the retinal pigment epithelium/choroid (mean, 2,389 ⫾ 1592 ng/g and 439 ⫾ 507 ng/g, dry weight; n ⫽ 16). Retinal pigment epithelium/choroid cadmium concentrations were fivefold greater than retinal pigment epithelium/choroid lead concentrations (P ⬍ .0001). Cadmium was found in the retina of all 30 eyes (mean, 1,113 ⫾ 486 ng/g, dry weight, n ⫽ 16), whereas lead was found in the retina in 9 (30%) of 30 eyes (mean, 59 ⫾ 75 ng/g, dry weight, n ⫽ 16) at a concentration 18-fold less than cadmium (P ⬍ .0001). Retinal pigment epithelium/choroid cadmium concentrations were twofold greater than retina cadmium concentrations (P ⫽ .0002), whereas retinal pigment epithelium/ choroid lead concentrations were sevenfold greater than retina lead concentrations (P ⬍ .0001). Five subjects were smokers, 10 were nonsmokers, and 1 was unknown. Cadmium concentrations in the retinal pigment epithelium/choroid and retina were greater in smokers than in nonsmokers (P ⫽ .004, P ⫽ .002, respectively; Table 2). Blood cadmium concentrations were not significantly different in smokers (3.7 ⫾ 6.1 g/l, n ⫽ 5) when compared with nonsmokers (2.4 ⫾ 3.1 g/l, n ⫽ 10, P ⫽ .38). There was no difference in lead concentrations in the retinal pigment epithelium/choroid and retina in smokers when compared with nonsmokers (P ⫽ .56, P ⫽ .62, respectively; Table 2). Retina and retinal pigment epithelium/choroid cadmium concentrations in the right eye correlated with concentrations in the left eye (P ⬍ .001). Similarly, retinal pigment epithelium/choroid lead concentrations in the right eye correlated with concentrations in the left eye (P ⬍ .001). Retina lead concentrations did not correlate between eyes (P ⫽ .92; Figure 1). The two eyes randomly selected for histologic examination (hematoxylin-eosin and periodic acid/Schiff) showed on blood, urine, and digests of hair and nails. As such, it is validated to perform with less than a 20% coefficient of variation on both an intra- and inter-assay basis at the lowest level of each calibration curve. These values in g/l are 10, 5, 0.2, and 1 for thallium, lead, cadmium, and mercury, respectively. Additionally, for the purposes of this study, the precision for lead was examined at a significantly lower level because of the concentration of lead in the tissue digests. A lead calibration curve ranging from 0.01 to 0.50 g/dl was prepared with each analytical run and demonstrated an r2 of 0.999 or better. To demonstrate analytical precision for lead, 17 tissue digests were analyzed 6 times over the course of 5 separate analytical runs. The CV of these analyses ranged from a low of 1.6% on a sample with a concentration of 0.219 ng/dl to a high of 35.9% on a sample with a concentration of 0.037 ng/dl. Seventy-three percent of samples with a lead concentration ⬎0.219 ng/dl had a CV ⬍15%. In the typical sample with a CV above 10%, the results increased with each measurement. This suggests that the variation in the results is primarily attributable to contamination and highlights the significant challenge of sample handling in trace metals analysis. ● DATA ANALYSIS: Heavy metal concentrations from two eyes of the same subject were averaged and treated as one observation (total number of observations equals 16). Tissue heavy metal concentrations, as a dry weight, were compared using a paired t test when data were distributed normally or Wilcoxon rank-sum tests if they were not. Lead and cadmium concentrations in smokers and nonsmokers were compared using a 2-sample t test. Correlations between right and left eyes were examined by using Pearson Product Moment analysis. The level of significance was P ⬍ .05. RESULTS MEAN BLOOD LEAD AND CADMIUM LEVELS AT THE TIME OF death were 0.5 ⫾ 1.2 g/dl (range, 0 – 4 g/dl) and 3.1 ⫾ 4.1 g/l (range, 0.2–14.6 g/l). All 16 subjects had blood lead levels within the normal adult range (⬍20 g/dl). Three (19%) of 16 subjects had blood cadmium levels 890 AMERICAN JOURNAL OF OPHTHALMOLOGY MAY 2005 FIGURE 1. Correlations of heavy metal concentrations (ng/g, dry weight) between left and right eyes for retina cadmium (Top left), retina lead (Bottom left), retinal pigment epithelium/choroid cadmium (Top right), and retinal pigment epithelium/choroid lead (Bottom right). that the dissected retina contained only neural retina and the dissected uvea contained both retinal pigment epithelium and choroid. DISCUSSION THIS INVESTIGATION DEMONSTRATES THAT THE HEAVY metals, lead and cadmium, accumulate in the tissues of adult human eyes, concentrating to the greatest extent in the retinal pigment epithelium and choroid. The pigmented tissues of the eye, such as the retinal pigment epithelium, choroid, iris, and ciliary body, have a high affinity for metal ions.8 Melanin within the pigment granules binds metal ions.11 Metal ions are bound by melanosomes according to atomic weight and volume (e.g., the percentage binding of calcium 30%, zinc 37%, lead 62%, iron 65%, and mercury 72%).8 Metals such as zinc, copper, calcium, manganese, molybdenum, and iron are found in ocular melanosomes, particularly within the retinal pigment epithelium.8,12–14 Heavy metals can effectively compete for the same binding sites as other metal ions15 and have the capacity to replace previously bound metals and alter ocular metal concentrations.16,17 Once bound, heavy metals are not VOL. 139, NO. 5 easily amenable to displacement.18 Ulschafer and coworkers,7 using metal x-ray spectra, showed that aluminum, mercury, and selenium were sometimes present in retinal pigment epithelium melanosomes; energy spectra for lead and cadmium were not presented. Eichenbaum and Zheng9 found measurable concentrations of lead in the choroid and retina; cadmium was not analyzed. Does the accumulation of lead and cadmium in ocular tissues provoke toxic injury? Neither lead or cadmium has any demonstrated beneficial effect, and both metals generally disrupt cellular biochemistry.6 Neurotoxicity from lead19 and cadmium20 exposure is of concern, especially because lead at even very low concentrations can have profoundly detrimental neurologic effects21 Low-level lead exposure produces scotopic vision deterioration and rod and bipolar apoptotic cell death.1,22,23 In rabbits, lead poisoning causes swelling of the retinal pigment epithelium,24 which leads to degeneration of the photoreceptors.25 Visual loss in humans after systemic lead poisoning is usually related to encephalopathy and optic neuropathy, because of the toxic effect of lead on the brain and optic nerve. Recent evidence, however, indicates that lead and cadmium can exert oxidative stress by producing reactive oxygen species that result in lipid peroxidation, DNA damage, and HEAVY METAL CONCENTRATIONS IN HUMAN EYES 891 depletion of cell antioxidant defense systems.19,26 Oxidative stress and free radical damage is thought to play a significant role in age-related macular degeneration.27 The metal ion, iron, has recently been implicated in retinal degeneration through iron-mediated oxidative damage.28 Whether the accumulation of lead and cadmium in the retinal pigment epithelium/choroid or retina could reach a concentration necessary to cause retinal pigment epithelium and photoreceptor damage requires additional study. Lead and cadmium were found in all of the pigmented ocular tissues (e.g., retinal pigment epithelium/choroid, ciliary body) that we studied. The importance of melanin binding of heavy metals in pigmented ocular tissues is unclear. Melanin may confer tissue protection by acting as a filter or detoxicant for heavy metals from the adjacent neural retina and photoreceptor cells.7,9 Similar to the retinal pigment epithelium, the choroid plexus of the brain sequesters lead, acting as a defensive barrier to prevent entry of toxic elements into the brain.29 Conversely, melanin binding of heavy metals throughout the life of an individual produces a local reservoir of potentially toxic elements that ultimately could reach a concentration that is destructive to the retinal pigment epithelium and adjacent retina. For example, chronic exposure to chloroquine and phenothiazine derivatives, which have an affinity for melanin, can result in degeneration of pigment cells or adjacent photoreceptors.30,31 In our study, lead and cadmium concentrations in the retinal pigment epithelium/choroid were significantly higher than concentrations in the retina. Because heavy metals have a high affinity for sulfhydryl groups in melanin, one would expect higher heavy metal concentrations in the pigmented retinal pigment epithelium and choroid than in the neural retina. In contrast, Eichenbaum and Zheng,9 reported higher lead concentrations in the retina than in the choroid. These authors, however, did not screen for blood lead levels, so it is not known if their subjects had systemic lead intoxication. Additionally, they used older atomic absorption spectrophotometry that is approximately 50-fold less sensitive to lead detection than the mass spectrometer used in our study. Finally, they mistakenly attributed retina lead levels to the accumulation of lead ions in retinal pigment epithelium melanosomes. Many studies,24,32 as well as our histologic examination, show that the neural retina separates from the retinal pigment epithelium at death and that retinal pigment epithelium cells are included with the choroid not the neural retina. How lead and cadmium avoid the blood-retinal barrier and gain entry to the neural retina is not entirely clear. Investigators have shown that lead and cadmium can enter various cells through calcium channels33 or avoid the blood-brain barrier by retrograde axonal transport.34 Additionally, potential defects or gaps in the blood-retinal barrier could represent sites for metal ion transport or 892 AMERICAN JOURNAL leakage into the retina. For comparison, retina cadmium levels in our study (1,072 ⫾ 489 ng/g) are 20-fold higher than published normal brain cadmium levels (38 to 57 ng/g).10 Retina lead levels (53 ⫾ 54 ng/g), by contrast, are similar to published normal brain lead levels (0 –100 ng/g).10,35 Lead and cadmium are industrial pollutants that cause permanent contamination of air, dust, and soil. These heavy metals are released into the environment from fossil fuel power plants, mining and smelting of metal ores, trash incineration, and combustion of leaded gasoline. Human exposure to these metals is inevitable. Lead and cadmium enter the blood from either the lung or intestine and clear the blood rapidly in approximately 30 days.36 By contrast, lead and cadmium reside in target organs with very long half-lives, accumulate in the body over time, and increase in concentration with age.5,19,21 Therefore, tissue metal concentrations reflect cumulative exposure, whereas blood concentrations reflect recent exposure.10,37 In our study, blood lead and cadmium concentrations in all subjects were well below alert levels, indicating no recent elevated exposure. Lead and cadmium concentrations in the ocular fluids (e.g., vitreous and aqueous) were similarly very low or not detectable. Tissue concentrations of lead and cadmium were considerably higher, suggesting that the ocular tissue heavy metal concentrations in these subjects reflect accumulation from chronic exposure rather than recently elevated doses. No previous studies have examined cadmium concentrations in the choroid and retina of human eyes. We found cadmium in the retinal pigment epithelium/choroid and retina of all the subjects studied. Similarly, cadmium primarily accumulates in the uvea of rabbit eyes.38 In our study, retinal pigment epithelium/choroid and retina cadmium concentrations were significantly greater in smokers than in nonsmokers. Others have shown that smokers have higher cadmium body burdens than nonsmokers of similar ages.39 Tobacco plants are a bioaccumulator of cadmium, and cigarette smoke is a significant source of cadmium,40 with 50% of inhaled cadmium absorbed into systemic circulation.39 Blood cadmium can then reach the uvea and be deposited in the choroid and adjacent retinal pigment epithelium. In summary, lead and cadmium are toxic heavy metals that accumulate in the retinal pigment epithelium and choroid, ciliary body, and the retina of humans at concentrations greater than found in the blood or in the fluids of the eye. The potential ocular toxicity of these heavy metals and their possible role in diseases of the retina and choroid requires further study. REFERENCES 1. Fox DA, Campbell ML, Blocker YS. Functional alterations and apoptotic cell death in the retina following developmenOF OPHTHALMOLOGY MAY 2005 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. tal or adult lead exposure. Neurotoxicology 1997;18: 645– 664. Bressler J, Kim KA, Chakraborti C, Goldstein G. Mechanism of lead neurotoxicity. Neurochem Res 1999;24:595– 600. Humphreys DJ. Effects of exposure to excessive quantities of lead on animals. Br Vet J 1991;147:18 –30. Khalil-Manesh F, Gonik HC, Weiler EJ, et al. Lead-induced hypertension: possible role of endothelial factors. Am J Hypertens 1993;6:723–729. Satarug S, Baker JR, Urbenjapol S, et al. A global perspective on cadmium pollution and toxicity in non-occupationally exposed population. Toxicology Letters 2003;137:65– 83. Stillman MJ, Presta A. Characterizing metal ion interactions with biological molecules—the spectroscopy of metallothionein. In: Zalups RZ, Koropatnick J, editors. Molecular biology and toxicology of metals. New York: Taylor & Francis 2000:276 –299. Ulshafer RJ, Allen CB, Rubin ML. Distributions of elements in the human retinal pigment epithelium. Arch Ophthalmol 1990;108:113–117. Potts AM, Au PC. The affinity of melanin for inorganic ions. Exp Eye Res 1976;22:487– 491. Eichenbaum JW, Zheng W. Distribution of lead and transthyretin in human eyes. Clin Toxicol 2000;38:377–381. Bush VJ, Moyer TP, Batts KP, Parisi JE. Essential and toxic element concentrations in fresh and formalin-fixed human autopsy tissues. Clin Chem 1995;41:284 –294. Larrson BS. Interaction between chemicals and melanin. Pigment Cell Research. 1993;6:127–133. Panessa BJ, Zadunaisky JA. Pigment granules: a calcium reservoir in the vertebrate eye. Exp Eye Res 1981;32:593– 604. Bowness JM, Morton RA, Shakir MH, Stubbs L. Distribution of copper and zinc in mammalian eyes: occurrence of metals in melanin fractions from eye tissues. Biochem J 1952;51: 521–530. Samuelson DA, Smith P Ulshafer FJ, et al. X-ray microanalysis of ocular melanin in pigs maintained in normal and low zinc diets. Exp Eye Res 1993;56:63–70. Drager UC, Balkema GW. Does melanin do more than protect from light? Neurosci Res Suppl 1987;6:575–586. Sarna T, Hyde JS, Swartz HM. Ion exchange in melanin, an electron spin resonance study with lanthanide probes. Science 1976;192:1132–1134. Jamall IS, Roque H. Cadmium-induced alterations of ocular trace elements. Influence of dietary selenium and copper. Biol Trace Elem Res 1989 –1990;23:55– 63. Sarna T, Froncisz W, Hyde JC. Cu 2⫹ probe of metal-ion binding sites in melanin using electron paramagnetic resonance spectroscopy. II. Natural melanin. Arch Biochem Biophys 1980;202:304 –313. Hsu P-C, Guo YL. Antioxidant nutrients and lead toxicity. Toxicology 2002;180:33– 44. Arvidson B. Cadmium toxicity and neural damage. In: Dreosti IE, Smith RM, editors. Neurobiology of the trace elements. Humana Press, Clifton, New Jersey, 1983:51–78. Goyer RA. Lead toxicity: current concerns. Environ Health Perspect 1993;100:177–187. VOL. 139, NO. 5 22. Fox DA, Sillman AJ. Heavy metals affect rods, but not cone photoreceptors. Science 1979;206:78 – 80. 23. Bushnell PJ, Bowman RE. Scotopic vision deficits in young monkeys exposed to lead. Science 1977;196:333–335. 24. Brown DVL. Reactions of the rabbit retinal pigment epithelium to systemic lead poisoning. Trans Am Ophthamol Soc 1974;72:404 – 447. 25. Hughes WF, Coogan P. Pathology of the retinal pigment epithelium and retina in rabbits poisoned with lead. Am J Pathol 1974;77:237–254. 26. Bhattacharyya MH, Wilson AK, Ragan SS, Jonch M. Biochemical Pathways in Cadmium toxicity. In: Zalups RZ, Koropatnick J, editors. Molecular biology and toxicology of metals. New York, New York: Taylor & Francis 2000:276 – 299. 27. Beatty S, Koh H, Phil M, et al. The role of oxidative stress in the pathogenesis of age-related macular degeneration. Surv Ophthalmol 2000;45:115–134. 28. Hahn P, Milam AH, Dunaief JL. Maculas affected by age-related macular degeneration contain increased chelatable iron in the retinal pigment epithelium and Bruch’s membrane. Arch Ophthalmol 2003;121:1099 –1105. 29. Cavallaro T, Martone RL, Dwork AJ, et al. The retinal pigment epithelium is the unique site of transthyretin synthesis in the rat eye. Invest Ophthal Vis Sci 1990;31:497– 501. 30. Ing RM. The melanin binding of drugs and its implications. Drug Metabol Rev 1984;15:1183–1212. 31. Koneru PB, Lien EJ, Koda RT. Review: oculotoxicities of systemically administered drugs. J Ocular Pharmacol 1986;2: 385– 404. 32. Fisher SK, Anderson DH. Cellular response of the retinal pigment epithelium to retinal detachment and reattachment. In: Marmor MF, Wolfensberger TJ, editors. The retinal pigment epithelium. Oxford University Press. New York, New York 1998:492–507. 33. Simons TJB. Lead-calcium interactions in cellular lead toxicity. Neurotoxicology 1993;14:77– 86. 34. Arvidson B. Retrograde axonal transport of cadmium in the rat hypoglossal nerve. Neuroscience Letters 1985;62:45– 49. 35. Barry PSI. A comparison of concentrations of lead in human tissues. Br J Ind Med 1975;32:119 –139. 36. Rabinowitz MB. Toxicokinetics of bone lead. Environ Health Perspect 1990;91:33–37. 37. Hu H, Rabinowitz M, Smith D. Bone lead as a biological marker in epidemiologic studies of chronic toxicity: conceptual paradigms. Environmental Health Perspectives 1998; 106:1– 8. 38. Grubb BR, DuVal GE, Morris JS, Bentley PJ. Accumulation of cadmium by the eye with special reference to the lens. Toxicol Applied Pharm 1985;77:444 – 450. 39. Elinder CG, Kjellstrom T, Lind B, et al. Cadmium exposure from smoking cigarettes: variations with time and country where purchased. Environ Res 1983;33:220 –227. 40. Chaney JA, Ryan JA, Li YM, Brown SL. Soil cadmium as a threat to human health. In: McLaughlin, MJ Singh, editors. BR Developments in plant and soil sciences. Dordrecht, Kluver Academic Publishers. 1999:219 –256. HEAVY METAL CONCENTRATIONS IN HUMAN EYES 893 Biosketch Jay C. Erie, MD is a comprehensive ophthalmologist and an assistant professor of Ophthalmology at Mayo Clinic and Mayo College of Medicine, Rochester, Minnesota, USA. 893.e1 AMERICAN JOURNAL OF OPHTHALMOLOGY MAY 2005