Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
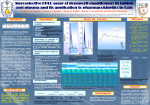
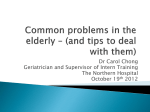
Syncope secondary to second-degree atrioventricular block with donepezil use Aneley Hundae, MD, Aasim Afzal, MD, Manish D. Assar, MD, and Jeffrey M. Schussler, MD Donepezil, an acetylcholinesterase inhibitor, is approved for the treatment of mild to moderate dementia secondary to Alzheimer’s disease. Although most prescribers are aware of the common gastrointestinal side effects of donepezil, cardiovascular side effects are rarely observed. Cardiovascular side effects of donepezil have almost always been observed in patients with a history of conduction defects or sick sinus syndrome. We report a case of a woman with early onset Alzheimer’s disease and no history of cardiac disease who developed second-degree heart block after a few weeks of therapy with donepezil. Withdrawal of donepezil led to resolution of the atrioventricular block. D onepezil, along with galantamine and rivastigmine, has been commonly prescribed for treatment of Alzheimer’s disease. Although cardiovascular adverse events have been reported, they are rarely experienced. This case highlights atrioventricular block as a potential adverse effect of donepezil. CASE PRESENTATION A 50-year-old woman who had developed early onset Alzheimer’s dementia at the age of 45 was brought to the hospital after she experienced a witnessed syncopal event. According to her husband, she lost consciousness for about a minute with no signs of seizure activity. Her husband reported that she had been “slow” for a few days. She was not on any prescription medication other than donepezil, which was started a few days prior to presentation. Her family indicated that she had been taking donepezil regularly and did not take more than the prescribed dosage. The family history was significant for Alzheimer’s disease. On physical exam, there were signs of advanced dementia. Thyroid function, syphilis serology, and vitamin B12 were normal or negative. The electrocardiogram (ECG) obtained by paramedics showed second-degree atrioventricular block (AVB) (Figure 1) with a heart rate of 30 beats per minute. No previous ECG was available for comparison. An echocardiogram showed a normal left ventricular ejection fraction and no structural abnormalities. The patient was admitted to the hospital and donepezil was stopped. Her heart rate gradually rose, and no new syncopal events occurred. A later ECG showed sinus rhythm, with only a first-degree AVB (Figure 2). The patient remained asymptomProc (Bayl Univ Med Cent) 2014;27(4):325–326 atic during the rest of her hospital stay and was subsequently discharged. At 1-month follow-up, her ECG showed no AVB. DISCUSSION Cholinesterase inhibitors are a class of drugs that include donepezil, rivastigmine, and galantamine. They inhibit acetylcholinesterase enzyme in the central nervous system and increase acetylcholine, which is deficient in Alzheimer’s disease (1). Donepezil is highly selective for the central nervous system and is widely used in Alzheimer’s disease. Common side effects include nausea, diarrhea, malaise, and dizziness. In theory, the cholinergic effect of donepezil can cause sinus bradycardia and AVB. Donepezil, being a cholinesterase inhibitor, leads to increased levels of acetylcholine, which stimulates glycinergic and GABAergic inhibitory receptors by vagal neurotransmission, which in turn act to slow the heart rate (2). Theoretically, donepezil and other acetylcholinesterase inhibitors can aggravate preexisting nodal disease and lead to AVB (2). Heart rhythm disturbances, however, are rare (3). In a study of 1762 patients with Alzheimer’s disease on donepezil, Dunn et al reported nausea, diarrhea, malaise, dizziness, and insomnia as common side effects, with no reported cardiac rhythm disturbances (4). Bordier et al reviewed 16 patients with Alzheimer’s disease who presented with syncope. AVB was present in 2 of the 16 cases (5). Suleyman et al (3) reported complete AVB and ventricular arrhythmia associated with donepezil use. Rowland et al have suggested guidelines for managing cardiovascular risks prior to and during treatment with acetylcholinesterase inhibitors. A heart rate check is recommended at baseline, and if the rate is <50 beats per minute, the cause of bradycardia needs to be investigated before starting the medication. Monthly follow-up is recommended after drug initiation or dosage change, and 6-month follow-up is recommended during the drug maintenance phase (2). From the Department of Internal Medicine (Hundae), Division of Cardiology (Afzal, Schussler), Baylor University Medical Center at Dallas; and the Department of Internal Medicine, Texas A&M College of Medicine (Schussler). Corresponding author: Jeffrey M. Schussler, MD, Division of Cardiology, Department of Internal Medicine, 621 N. Hall Street, Suite 400, Dallas, TX 75226 (e-mail: [email protected]). 325 Figure 1. Electrocardiogram at the time of syncope showing second-degree atrioventricular block. Figure 2. Electrocardiogram before discharge; second-degree atrioventricular block had changed to first-degree atrioventricular block. 1. 2. 3. 326 Ellis JM. Cholinesterase inhibitors in the treatment of dementia. J Am Osteopath Assoc 2005;105(3):145–158. Rowland JP, Rigby J, Harper AC, Rowland R. Cardiovascular monitoring with acetylcholinesterase inhibitors: a clinical protocol. Advances Psych Treatment 2007;13:178–184. Suleyman T, Tevfik P, Abdulkadir G, Ozlem S. Complete atrioventricular block and ventricular tachyarrhythmia associated with donepezil. Emerg Med J 2006;23(8):641–642. 4. 5. Dunn NR, Pearce GL, Shakir SA. Adverse effects associated with the use of donepezil in general practice in England. J Psychopharmacol 2000;14(4):406–408. Bordier P, Lanusse S, Garrigue S, Reynard C, Robert F, Gencel L, Lafitte A. Causes of syncope in patients with Alzheimer’s disease treated with donepezil. Drugs Aging 2005;22(8):687–694. Baylor University Medical Center Proceedings Volume 27, Number 4