Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
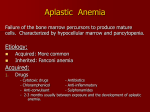
CPC Jaji Bettadpur MD MED-PEDS Jan 14th 2005 CASE Chief Complaint: Generalised fatigue and weakness. HPI: Pt is a 68 year old white male 1-2 month h/o worsening fatigue. Mild shortness of breath . No fevers ,chills,nausea or vomting. No cough or sick contacts No chest pain/palpitations/orthopnea Mild dyspnea on exertion. CASE No weight loss or changes in appetite, Occasional constipation. No hematochezia, melena, dysuria or hematuria. Denies rashes notes several small bruises on his legs. PMH : HTN – diagnosed in 1972 Atrial fibrillation- diagnosed in July 2004 Osteoarthritis GERD Hyperlipidemia BPH CASE MEDICATIONS Aspirin 325 mg qd Lisinopril 40 mg qd Meclizine 25 mg tid prn Terazosin 5 mg qhs Amiodarone 200 mg qd Hydralazine 25 mg tid Simvastatin 20 mg qhs CASE Social History : Tobacco –quit in 1972 after 45 pack/year history Alcohol –quit in 1972.Drank socially Drugs-denies Retired veteran and airport maintenance supervisor CASE Family History: Aunt with DM No Family history of CAD or Cancers. CASE Physical Exam: Vitals : T-97.5, P-74 BP 118.74,R 20 General; Alert,oriented in NAD HEENT-PERRL,EOMI ,mucous membranes moist, pale conjunctiva,Oropharynx-normal ,no thyromegaly,No JVD, no LAD,no carotid bruits. CASE Continued… CVS-RRR with soft systolic murmur 2/6 at apex LUNGS-CTA –Bilaterally. No wheezing or rhonchi. ABDOMEN-soft,NT,ND ,normal BS,no splenomegaly, no masses. EXTREMITIES -mild1+edema,good peripheral pulses,multiple small petechiae on legs. LABS Na- 138 K 3.2 Chloride -104 Bicarb 26 BUN 20 Creatinine 1.8 Glucose 88 Calcium-8.7 Magnesium 2.2 LABS TSH 10.57 FT4 0.9 Normal(0.4 - 5.7) Iron studies : Fe 43 TIBC 307 CBC 03/04 WBC- 7.0 08/04 WBC 5.1 10/04 WBC 3.7 Hgb 16.6 Hgb 12.9 Platelets 180 Platelets 153 Hgb 9.3 MCV 94 Retic 0.5% Platelets 86 Signs and Symptoms Pertinent Positives: Pale conjunctiva Worsening fatigue Mild Shortness of breath Constipation soft systolic murmur petechiae on legs. history of Atrial fibrillation Signs and Symptoms Pertinent Negatives: No weight loss No change in appetite No fevers or chills No cough No hematuria No adventitious sounds on lung examination No thyromegaly No splenomegaly Problem list Pancytopenia Low Reticulocyte count Atrial Fibrillation on Amiodarone Hypothyroidism Bone Marrow Failure The study of bone marrow failure is traditionally dated to 1888. Paul Ehrlich described a patient who died after an explosive short illness. In 1904 Vaquez and Aubertin presented a case report and first named the disease. BONE MARROW Failure Cabot stressed the marrow’s distinctive pathology and emphasized the need for it’s examination. Tissues from patients were only examined during autopsy in the earlier cases of AA. In practice Pancytopenia was often equated with aplastic anemia. The etymologic root of the term aplastique! Aplastic Anemia Severe AA Moderate AA At least 2 of the following: ANC <0.5x109/L Platelet count <20 x 109/L Anemia with corrected Retic count <1% Those with Pancytopenia who do not fulfill the criteria of severe disease. AND One of the following: Bone marrow cellularity <25% Bone Marrow cellularity <50% with fewer than Pancytopenia With Hypocellular Bone marrow: Acquired Aplastic Anemia Inherited Aplastic anemia Some Myelodysplasia syndromes. Acute Leukemia Some Lymphomas of the Bone Marrow Acquired Aplastic Anemia Irradiation Drugs Viruses EBvirus (infectious Mononucleosis) ,Hepatitis, Parvovirus, HIV. Immune diseases Idiopathic aplastic anemia With Hypocellular Bone marrow: Acquired Aplastic Anemia Inherited Aplastic anemia Some Myelodysplasia syndromes. Acute Leukemia Some Lymphomas of the Bone Marrow APLASTIC ANEMIA Pancytopenia WITH CELLULAR BONE MARROW: Primary Bone marrow disorders: * Myelodysplasia syndromes * Paroxysmal Nocturnal hemoglobinuria * Myelofibrosis with myeloid metaplasia * Some aleukemic leukemias * Myelopthisis * Bone marrow lymphoma * Hairy cell leukemia PANCYTOPENIA SECONDARY TO SYSTEMIC DISEASES: 1. SLE 2. Sjogren’s syndrome 3. Hypersplenism 4. VitaminB12, folate deficiency 5. Overwhelming infection 6. Alcohol 7. Brucellosis 8. Ehrlichiosis 9. Sarcoidosis 10. Tuberculosis and atypical mycobacteria PANCYTOPENIA 1. 2. 3. 4. 5. HYPOCELLULAR BONE MARROW with or without CYTOPENIA: Q fever Legionnaires’ disease Mycobacteria Anorexia nervosa Hypothyroidisim Narrowed Differential Myelodysplastic syndrome Acute Leukemia Acquired Aplastic Anemia : Drugs causing Pancytopenia Idiopathic AA Hypothyroidism HYPOTHYROIDISM High TSH Low FT4 Symptoms of Fatigue Constipation Pallor Usually normocytic anemia. Hypothyroid A case of a 68 year old woman who presented with myxedema coma and was found to be anemic. Further investigations showed a pancytopenia and a hypoplastic anemia confirmed by bone marrow. Following treatment she became euthyroid and was found to have resolution of her pancytopenia and bone marrow returned to normal.(Song SH et al 1998) DIFFERENTIAL Hypothyroidism Myelodysplastic syndrome Acute Leukemia Acquired Aplastic Anemia : Drugs causing Pancytopenia Idiopathic AA Myelodysplastic syndromes Cytopenia with a cellular Bone marrow Morphologic abnormalities in 2 or more cell lines. Usually idiopathic May be seen after chemotherapy Ineffective hematopoeisis Myelodysplastic syndrome May evolve into AML Frequent abnormalities involving long arm of chromosome 5 Deletions of chromosome 5 and 7 MYELODYSPASIA and the % which convert to Acute Leukemia RA with ring sideroblasts Rare Refractory anemia 5- 15 % Refractory anemia with 25- 40% excessive blasts Refractory anemia with 70-90% excessive blasts in transformation (RAEB-T) CMML 25-40% RAEB RAEB. Note agranular myelocytes and agranular poorly segmented neutrophil, and abnormal basophil with dense nuclear chromatin (arrowed). RARS RARS. Left-shifted megaloblastoid erythropoiesis. A cluster of proerythroblast cells Contain curdled chromatin. Result of ineffective erythropoiesis Findings Age over 60 Asymptomatic with abnormal blood count Fatigue Infections or bleeding Course indolent May have splenomegaly Laboratory findings Anemia MCV normal or increased Reticulocyte count usually reduced Neutropenia common Neutrophils exhibit Pelger Huet cells Myeloid series may be left shifted. Small number of blasts or promyelocytes may be seen. Platelets normal or reduced. Pelger Huet cells Bone Marrow Hypercellular / Hypocellular Erythroid hyperplasia is common Signs of abnormal erythropoiesis include megaloblastic features,nuclear budding or multinucleated erythroid precursors. BONE MARROW Prussian blue stain may show ring sideroblasts. Characteristic abnormality is the presence of dwarf megakaryocytes with a unilobed nucleus. TREATMENT Patients supported with transfusions. GCSF or GMCSF. Erythropoietin subcutaneously weekly Azacitidine improves both symptoms and blood counts and prolongs time to conversion to acute leukemia. Revimid (CC-5013) may hold promise in patients with low risk myelodysplasia. Prognosis It is ultimately a fatal disease. Risk of transformation to AML depends on the percentage of blasts in the bone marrow. PROGNOSIS Those with excessive blasts or CMML have short survival usually less than 2 years and have a higher risk of developing AML Findings with full deletions is associated with a poor prognosis. DIFFERENTIAL Myelodysplastic syndromes Acute Leukemia Acquired Aplastic Anemia : Drugs causing Pancytopenia Idiopathic AA ACUTE LEUKEMIA Malignancy of the hematopoietic progenitor cell. Most cases arise with no clear cause. The malignant cells proliferate in an uncontrolled fashion and replace normal bone marrow. The cases which arise after toxin or chemotherapy exposure often develop from a myelodysplastic prodrome and are associated with abnormalities in chromosome 5 and 7. ACUTE LEUKEMIA Short duration of symptoms. Fever, fatigue and bleeding. Cytopenia or pancytopenia. Bone marrow may have more than 20% blasts. AML is an adult disease with a median age of presentation of 60 years and an increasing incidence with advanced age. AML ACUTE LEUKEMIA SYMPTOMS and SIGNS: Fever Dyspnea Gingival bleeding or epistaxis Neutropenia Tiredness. ACUTE LEUKEMIA On examination patients are pale with petechiae and may not have signs of infection. Gum hypertrophy,stomatitis and bone or joint pain may be present. Splenomegaly and lymphadenopathy may be present in AML but less remarkable than in ALL FAB This classification lists M0 –M7 In M3 patients Organomegaly is uncommon. High frequency of DIC is seen. In M4 Leukocyte count is markedly elevated. Organomegaly and lymphadenopathy are common. Leukemic skin and Gum deposits noted FAB classification M5 is associated with a relatively high incidence of organomegaly, lymphadenopathy and leukemic skin and gum deposits. M6 –many cases evolve from MDS or present as a secondary leukemia. M7 associated with Down’s syndrome WHO This classification incorporates cytogenetic and molecular findings in addition to morphologic ,cytochemical and immunophenotype features. Major change is, the reduction of the number of blasts required for the diagnosis of AML from 30-20% DIAGNOSIS Peripheral blood smear shows circulating blasts. Auer rods are seen in leukemic blasts. If blasts sparse then Definitive diagnosis by BM biopsy. Infiltration of bone marrow with leukemic blasts is seen. ACUTE LEUKEMIA Blast forms must be identified as myeloid and not lymphoid lineage. It should be classified as the appropriate variant according to the FAB and WHO classifications. TREATMENT Induction therapy aims to reduce the total body leukemic cell population . Hence the goal of remission induction therapy is to restore normal bone marrow function. Postinduction or remission consolidation therapy requires one or more courses of chemotherapy or BM transplantation. TREATMENT Cytogenetic testing is recommended prior to starting therapy in every newly diagnosed patient The most common remission Induction therapy employs cytarabine and daunorubicin. TREATMENT Depending on age and patient selection, 60-80% attain complete remission with this regimen. The same chemotherapy regimen used for remission induction can be repeated for one or more cycles as consolidation treatment. AML Auer rods DIFFERENTIAL Myelodysplastic syndromes Acute Leukemia Acquired Aplastic Anemia : -Drugs causing Pancytopenia -Idiopathic AA DRUGS 1. 2. 3. 4. 5. 6. Innumerable drugs Drugs taken by patient Amiodarone Lisinopril Hydralazine Aspirin Meclizine Simvastatin DRUGS Medical drug use is frequently associated with Aplastic anemia. At the end of the 19th century Chemicals like Benzene were linked to marrow function. This concept was further supported by the association with amidopyrine and later with Chloramphenicol in the 1960s Classification 1. 2. 3. 4. 5. Agents that regularly produce marrow depression Cytotoxic drugs used in cancer chemotherapy: Alkylating agents Antimetabolites Antimitotics Some antibiotics Benzene and less often benzene containing chemicals. CLASSIFICATION 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. Agents probably associated with aplastic anemia but with a relatively low probability relative to their use: Chloramphenicol Insecticides Antiprotozoals NSAIDS Anticonvulsants Gold and Arsenic Sulfonamides as a class. Antithyroid medications Antidiabetes drugs Carbonic anhydrase D-Pencillamine 2 Chlordeoxyadenosine CLASSIFICATION 1. 2. 3. Agents more rarely associated with Aplastic Anemia: Antibiotics Antihistamines. Sedatives and Tranqulizers 4. Antiarrhythmics 5. 6. 7. 8. Lithium Thiocyanate Carbimazole Amphetamines 9. Lisinopril Drugs LISINOPRIL Hematological effects: * Rare causes of Bone marrow depression has been reported including anemia,neutropenia and thrombocytopenia * One case of Pancytopenia has been reported in a 79 year old woman after 12 months of Lisinopril therapy 5mg/day (Schratzlseer et al 1994) * Small reduction in hemoglobin has been seen frequently in some patients. Lisinopril A single case of Hemolytic anemia has been reported which resolved after stopping the drug and treating with a tapering steroid therapy No cases of Thyroid abnormalities reported. HYDRALAZINE Pancytopenia has been reported in a 63 year old male who was treated with 25 mg qid for 10 days. He was also noted to have obstructive jaundice. The patient recovered within 2 weeks of withdrawal from Hydralazine. Constipation seen No thyroid abnormalities noted. ASPIRIN Anemia, thrombocytopenia seen. No thyroid abnormalities. AMIODARONE Antiarrhythmic agent Class 111 Has innumerable side effects reported. Causes Pulmonary toxicity Thyroid problems:Hypothyroidism (1% to 22%) Hyperthyroidism (<3%), Gastrointestinal: Nausea, vomiting, anorexia and constipation (10% to 33%), Rare cases of Pancytopenia AMIODARONE Iodinated benzofuran derivative. Contains 2 iodine atoms It’s metabolisim in the liver releases approximately 3 mg of inorganic iodine per 100 mg of Amiodarone into the systemic circulation. A typical American diet has an average iodine intake of 0.3 mg/day. Therefore 6 mg of iodine associated with a 200mg dose significantly increases the daily load. AMIODARONE Elimination from the body occurs with a half-life of about 100 days. Hence toxicity can occur well after withdrawal. Effects of Amiodarone on Thyroid function are divided into 2 categories: 1. Intrinsic effects on Thyroid 2. Effects due to Amiodarone’s iodine content. INTRINSIC EFFECTS on THYROID It inhibits the outer ring of T4 hence decreases production of T3 reverses T3 accumulation since it is not converted to T2. Blocks T3 receptor binding to nuclear receptors and decreases expression of some thyroid hormone related genes. Direct effect on thyroid follicular cellsdestructive Thyroiditis Effects due to Iodine content Normal autoregulation of Iodine prevents normal individuals from becoming hyperthyroid after exposure to an iodine load(radiocontrast) When a critical high is reached in intrathyroidal concentrations the Wolff-Chaikoff effect takes place. AMIODARONE With underlying disease there are defects in Iodine autoregulation. People with autoimmune thyroid disease fail to escape from the WC effect. Patients with autonomous function in a nodular goitre do not autoregulate iodine. Hence the effects of Iodine in Amiodarone is dependent on the underlying status of the patient. AMIODARONE HYPOTHYROIDISM TSH elevation may be transient during the first few months of therapy. Small increases in TSH (10-20) and low normal serum T4 concentrations occur in about 20% of patients Hypothyroidism can occur as soon as 2 weeks and as late as 39 months after initiating therapy. AMIODARONE Treatment of Hypothroidism: It resolves on discontinuation of therapy in patients with no underlying disease. Amiodarone is usually not discontinued Thyroid function can be normalised with T4 therapy. AMIODARONE Pancytopenia is seen in <1 % of cases. Other hematologic adverse effects have been reported in the literature in about 1-3% such as coagulation abnormalities. Precise mechanism of these toxic reactions are not known In Feb of 2004 ,2 cases in which each of the 2 patients who were on Amiodarone were noted to have developed pancytopenia. Further investigations led to granulomas in their bone marrow. AMIODARONE In June of 2000 a case was reported where Patient was noted to have thrombocytopenia. She had been receiving Amiodarone for 8 months prior to this. Her bone marrow biopsy showed multiple noncaseating epitheloid granulomas. These on repeat BM biopsy were fewer on cessation of the drug. It was concluded that a Bone marrow biopsy is required in any blood dyscrasia associated with amiodarone. AMIODARONE Rosenbaum et al in 1998 presented 2 case reports. In the first case the patient had a diagnosis of myeloproliferative disorder for about 10 years and had been on aspirin for several years. She was started on Amiodarone and a follow up Bone marrow biopsy showed granulomas. All tests including fungal TB were negative. It was concluded that Amiodarone was directly responsible for these granulomas. AMIODARONE In the second case a 78 year old with atrial fibrillation was started on Amiodarone and 18 months later a bone marrow biopsy was done to investigate polyclonal gammopathy. Granulomas were noted in the bone marrow Amiodarone was discontinued. However in both cases amiodarone could not conclusively be implicated as no follow up bone marrow was done. Epitheloid Granuloma Granuloma AMIODARONE In 2001 another case described a patient with indolent myeloma on therapy with Amiodarone who was noted to have bone marrow granulomas which resolved on cessation of therapy. He was noted to have anemia and no clinical or laboratory evidence for mycobacteria ,fungal or sarcoidosis. Following cessation of the Amiodarone the bone marrow granulomas dissappeared . The anemia resolved. AMIODARONE In Feb of 2004, 2 cases of Amiodarone induced Bone Marrow granulomas were reported in patients being investigated for pancytopenia and refractory anemia respectively. The patient had been on Amiodarone for 2 years 200 mg/day. By exclusion it was attributed to the drug Amiodarone. DIAGNOSIS Myelodysplastic syndrome AML Acquired Aplastic Anemia: Amiodarone induced Pancytopenia and hypothyroidism CONCLUSION Stop Amiodarone . TESTS REQUIRED 1)Peripheral Blood smear. 2)Bone marrow biopsy. REFERENCES Practical diagnosis of Hematology 3rd ed Carl Kjeldsberg MD CRC desk reference for Hematology N.K. Shenton Hoffman : Hematology: Basic principles and Practice 3rd ed. Micromedex Healthcare series Uptodate Hypoplastic anemia complicating myxoedema coma Song SH,McCallum CJ,Campbell IW Amiodarone induced bone marrow granulomas steven k. Moran and Arumugan Manoharan. Amiodarone induced bone granulomas N.Y.Z. Boutros,S.Dilly Unexplained Bone Marrow granulomas: Is Amiodarone the culprit? A report of 2 cases Amiodarone –associated granuloma in bone marrow. The End To receive credit for having studied the CPC, please send Dr. Oliver (TAMU 407i) a list of the differential diagnoses for this patient.



























































































![Aplastic Anemia [PPT]](http://s1.studyres.com/store/data/000248384_1-5c39883593ffaaa864ec61d1eb51b312-150x150.png)



