Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
History of invasive and interventional cardiology wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Myocardial infarction wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Coronary artery disease wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
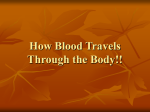
J Appl Physiol 106: 1338–1346, 2009. First published January 29, 2009; doi:10.1152/japplphysiol.90592.2008. Right coronary artery becomes stiffer with increase in elastin and collagen in right ventricular hypertrophy Marisa Garcia2 and Ghassan S. Kassab1 1 Department of Biomedical Engineering, Surgery, Cellular and Integrative Physiology, Indiana University Purdue University, Indianapolis, Indiana; and 2Department of Biomedical Engineering, University of California, Irvine, California Submitted 29 September 2008; accepted in final form 26 January 2009 stress; strain; wall shear stress; constitutive equation BLOOD VESSELS ARE subjected to the mechanical loading of blood pressure and blood flow throughout the cardiac cycle. The vessels undergo structural and mechanical adaptations in response to changes in the local hemodynamic conditions. For example, changes in blood flow cause changes in fluid wall shear stress (WSS; the tractive frictional force exerted by flowing blood on the inner layer of the vessel wall) by eliciting a wide range of biochemical and physiological responses in experimental (46) and clinical studies (16, 22). Studies have demonstrated that a sudden increase in blood flow initiates an enlargement of the arterial lumen that progresses for months as the WSS tends to a homeostatic or normal level (23, 25). A gradual increase in blood flow has been reported by several groups to result in outward hypertrophic remodeling of resistance (4, 41, 44, 45, 47) and conductive arteries (25, 36, 39). The flow-induced remodeling may be an attempt to maintain mechanical homeostasis (24, 25). When blood flow is elevated in a vessel, the endothelium responds to restore WSS toward Address for reprint requests and other correspondence: G. S. Kassab, Dept. of Biomedical Engineering, SL-174, Indiana Univ. Purdue Univ. Indianapolis, 723 West Michigan St., Indianapolis, IN 46202 (e-mail: [email protected]). 1338 homeostatic levels by changing vascular tone, increasing the lumen diameter (44), and potentially altering the function and mechanical properties of the vessel wall. A detailed analysis of these adaptations is necessary to understand vascular function and dysfunction, including atherogenesis (36, 37). The increase in stiffness of arteries represents an early risk factor for cardiovascular diseases (1, 19). Specifically, increased stiffness is associated with aging (14), atherosclerosis (6), and heart failure (27). It is also associated with various risk factors including hypertension (7), diabetes (42), hyperlipidemia (33), and smoking (43). Furthermore, arterial stiffness has also been shown to be an independent risk factor for cardiovascular events such as primary coronary events (3). Therefore, the assessment of coronary mechanical properties is important in understanding the processes of coronary artery disease. Recently, our group (37) characterized the mechanical properties of normal coronary blood vessels in the range of physiological loading. We used a method of analysis to compute the biaxial (circumferential and axial) incremental elastic moduli under in vivo (homeostatic) conditions to characterize the stiffness of the vessel wall (37). Briefly, the method utilizes a well-accepted approach to nonlinear elasticity that uses a linearized incremental formulation. It was demonstrated that the normal incremental moduli under homeostatic conditions are layer (intima-media and adventitia) and direction (circumferential and axial) dependent. The objective of the present study was to quantitatively describe the remodeling of the right coronary artery (RCA) in response to flow-overload during right ventricular hypertrophy (RVH) in response to pulmonary artery banding. Our hypothesis is that the remodeled proximal RCA has increased homeostatic moduli in association with increases in elastin and collagen in the vessel wall. Accordingly, we determined the incremental elastic moduli in the circumferential, axial, and cross directions in the physiological range and the corresponding changes in elastin and collagen of the vessel wall using multiphoton microscopy (MPM) for the control and remodeled vessels in RVH. It was found that the moduli are significantly increased in all directions in line with an increase in elastin and collagen of media but more prominently of the adventitia. The physiological and pathophysiological implications of the increased stiffness in RCA are highlighted. METHODS Animal preparation. Ten male Yorkshire farm pigs were used in this study (5 RVH and 5 control). RVH was induced through acute The costs of publication of this article were defrayed in part by the payment of page charges. The article must therefore be hereby marked “advertisement” in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 8750-7587/09 $8.00 Copyright © 2009 the American Physiological Society http://www. jap.org Downloaded from http://jap.physiology.org/ by 10.220.33.4 on May 7, 2017 Garcia M, Kassab GS. Right coronary artery becomes stiffer with increase in elastin and collagen in right ventricular hypertrophy. J Appl Physiol 106: 1338 –1346, 2009. First published January 29, 2009; doi:10.1152/japplphysiol.90592.2008.—Changes in blood flow influence the structure, function, mechanical properties, and remodeling of arteries. The objective of the present study was to investigate the role of increased blood flow on the biaxial incremental elastic moduli of the porcine right coronary artery (RCA) and to determine the microstructural basis for the changes in moduli. We hypothesized that an increase in RCA flow will lead to increased stiffness in conjunction with remodeling of elastin and collagen in the vessel wall. The control and experimental groups consisted of five RCA vessels each. The RCA of the experimental group was exposed to 4 wk of flow-overload in right ventricular hypertrophy induced by pulmonary artery banding. Stress-strain relationships were determined and the incremental elastic moduli were derived in the circumferential, axial, and cross directions. The results show a significant increase in the elastic moduli in the circumferential (262.7 ⫾ 15.7 vs. 120.2 ⫾ 12.4 kPa; P ⬍ 0.001), axial (177.8 ⫾ 25.5 vs. 100.3 ⫾ 11.9 kPa; P ⫽ 0.025), and cross directions (104.8 ⫾ 8.2 vs. 68.2 ⫾ 8.6 kPa; P ⫽ 0.016) of the experimental RCA compared with controls. Multiphoton microscopy was used to assess the changes in elastin and collagen content in the media and adventitia of the vessel wall. We found a significant increase in elastin and collagen area fraction particularly in the adventitial layer. These data suggest stiffening of the vessel wall as a result of increased elastin and more predominantly collagen. STIFFER RCA IN FLOW-OVERLOAD J Appl Physiol • VOL from 0 to 125 mmHg at every stretch ratio. The Biopac system was used for continuous data acquisition. The vessels were preconditioned to stretch and pressure several (⬃5–7) times to ensure repeatable loading and unloading responses for both groups identically. After preconditioning, the forces generated and deformations were continuously acquired during loading. The total experimental duration was ⬍4 h. Morphometric measurements. After being tested, the coronary segment was removed from the luers and two rings, sufficiently distant (1–2 mm) from the ligated ends, were cut (one from each end) for the morphometric measurements of no-load and zero-stress states. Both rings were allowed to stabilize for 1–2 h in saline solution at room temperature (22°C). The rings were photographed in the no-load state before a cut was made radially at the anterior position allowing each sector to approach the zero-stress state. The rings opened into a sector and gradually approached a constant opening angle defined as the angle subtended by two radii connecting the midpoint of the inner wall to the ends of the open segment. The cross section of each sector was photographed 1 h after the radial cut. Using a morphometric analysis system (Sigma Scan Pro.5.0), the inner and outer circumferences and area of the rings in the no-load state were determined. The circumference of the border between the medial and adventitial layers was determined for each no-load and zero-stress state ring. The morphological measurements of inner and outer circumferences and opening angle in the zero-stress state were also acquired. Microscopic visualization of the vessel. The arterial wall contains collagen and elastin fibers and smooth muscle cells as the primary load-bearing components. MPM was used to visualize the microstructural components of excised porcine blood vessels through twophoton excited fluorescence (TPEF) and second-harmonic generation (SHG) microscopy. The current protocol for the visualization of elastin and collagen, exclusively, in porcine coronary arteries has been validated by Zoumi et al. (49) and is briefly described here. A 1- to 1.5-mm-long ring was obtained from the remaining, untested RCA and, in the zero-stress state, fixed in 10% formalin. An upright microscope was utilized making it necessary to use a special thinglass-bottom chamber in which a hole was drilled in the center of a culture dish and coverslipped to create a short well. The well was surrounded by a thin ring of grease and the specimen was placed inside with a small amount of saline (0.9%) solution at room temperature (22°C). A coverslip was placed on the grease and gently pressed down until just touching the segment. The dish was overturned and mounted on the upright microscope stage. A Zeiss LSM 510 Meta confocal/MPM system equipped with a tunable Titanium-Sapphire laser was used to scan the vessel thickness of arterial specimens. The samples were imaged with a 40⫻ corr, C-Apochromat, numerical aperture 1.2, water immersion microscope objective. Two-dimensional (x-y plane) images (512 ⫻ 512 pixels) were acquired from various depths (z) into the vessel wall at a rate of 9 frames/s (pixel dwell time of 1.6 s/pixel). Resolution was ⬃0.45 m and 0.5 m in the x-y and z image planes, respectively. MPM images were obtained using a 385– 425 emission filter for SHG and a 480 –520 band-pass infrared (IR) emission filter for TPEF. Each acquired image was typically integrated over a few seconds. The scan time for an entire vessel wall was ⬍1 h. Histology. Tissues were fixed (10% formalin) for at least 48 h before processing. Five rings from each group, control and experimental, were rinsed with a buffer solution, dehydrated, and embedded in paraffin. The 5-m-thick sections were mounted on glass slides and stained with Verhoeff’s Elastic stain. The nuclei counts were performed in the media using the ImageJ software. Statistical analysis. Student’s t-test was used to detect differences between control and experimental vessels. A P ⬍ 0.05 is indicative of a significant difference between the population means. Values are expressed as means ⫾ SE. 106 • APRIL 2009 • www.jap.org Downloaded from http://jap.physiology.org/ by 10.220.33.4 on May 7, 2017 pulmonary artery banding similar to Kassab et al. (26). All experiments were performed in accordance with national and local ethical guidelines, including the Institute of Laboratory Animal Research (ILAR) Guide, Public Health Service policy, Animal Welfare Act, and institutional policies regarding the use of animals in research and an approved Indiana University Purdue University IACUC protocol. Ketamine hydrochloride (20 mg/kg im) and atropine (0.05 mg/kg im) were used to preanesthetize the animals. Endotracheal intubation was performed and surgical anesthesia was mechanically maintained, via a face mask, through the inhalation of isofluorane (0.5–2%) and oxygen. An incision was made on the neck to chronically implant 7Fr sheaths in the left carotid artery, for arterial pressure measurement, and in the right external jugular vein, for drug administration. Lidocaine (80 mg iv) was administered as a bolus before cardiac instrumentation. A left lateral fourth-intercostal-space thoracotomy was performed using sterile techniques. A small segment of the proximal RCA was dissected free of surrounding tissue and a flow probe (Transonic) was placed around it to measure coronary flow. A glycerin-filled occluder was placed around the pulmonary artery and the associated tubing was exteriorized for inflation of the occluder after recovery. The thoracotomy was closed, and the animal was allowed to recover for 1 wk. After 1 wk of recovery, the animal was preanesthetized and surgical anesthesia was maintained, as described above, while a fluid-filled silastic pressure-monitoring catheter was inserted through the jugular sheath and advanced into the right atrium and right ventricle. The degree of banding of the pulmonary artery (PA) was gauged from the systolic RV pressure. The occluder was slowly filled with glycerin which stenosed the PA until the RV systolic pressure was raised by 9.3–10.7 kPa (70 – 80 mmHg). The occluder was then fixed to maintain this degree of stenosis over a 4-wk period, during which time the RV pressure was hypertensive, the cardiac muscle hypertrophied, and the RCA flow increased. After the 4-wk banding period, the animal was again preanesthetized and surgical anesthesia was administered as described above. A midline sternotomy was performed and a bolus of normal saline with 200 U/kg of heparin was injected through the carotid artery catheter. A set of angiograms was obtained for a separate study. The pigs were then euthanized by an injection of pentobarbital sodium (300 mg/kg) through the jugular vein. After harvest, the heart was placed in an ice-cold saline bath. The degree of RVH was assessed by measuring right-to-left ventricle weight ratio (8). In situ preparation of coronary vessel. About 3.2 cm of proximal RCA length was dissected free of fat and connective tissue under a dissection microscope ⬃1–2 cm from its emergence at aortic ostia and every branch was ligated to eliminate leakage from the blood vessel. The vessel was marked in situ and the axial retraction upon excision was documented to compute the axial stretch ratio (ratio of in situ-to-unloaded length). By tying silk sutures (3-0) around the insertion sites, a luer was secured in place on either end of the vessel. Ultrasonic crystals (Sonometrics) were sutured (10-0) diametrically at the midpoint of the vessel segment. The changes in diameter were continuously recorded with the crystals during mechanical testing. Experimental measurement. The protocol for biaxial (inflation and axial extension) testing of coronary arteries was recently described by our group (37, 38). Here, we modified the set-up by the addition of ultrasound crystals. Briefly, the arterial specimen with attached crystals was horizontally mounted on a TRIAX machine where the vessel was kept in a saline bath during testing. The test set-up included a pressure transducer and a manually driven linear stage where the axial force was recorded by a load cell. The pressure transducer was calibrated against a hydrostatic mercury column at pressures of 0 and 100 mmHg. The load cell was calibrated with a series of weights, and a linear relationship was confirmed. During testing, the axial stretch ratio (z; defined as the change in axial length between loaded and no-load state) was varied over a small range (1.3–1.5) relative to the in vivo loading. A pressure regulator was utilized to vary the pressure 1339 1340 STIFFER RCA IN FLOW-OVERLOAD RESULTS Fig. 1. Representative example of outer diameter measurements with ultrasonic crystals during a pressure ramp in control and flow-overload right coronary artery (RCA). puted according to Eqs. 1b and 4, respectively (APPENDIX). The circumferential and axial stresses and strains in conjunction with Eqs. 5 and 6 (APPENDIX) yield the values of the incremental moduli. The data on the circumferential, axial, and cross incremental moduli for the control and experimental RCA are summarized in Fig. 3. The results show a significant increase in the moduli of elasticity in the circumferential (P ⬍ 0.001), axial (P ⫽ 0.025), and cross (P ⫽ 0.016) directions of the experimental vessels compared with the control group. Figure 4 compares the mean circumferential Cauchy stress and Green strain for both groups at physiologic loading (pressure of 100 mmHg and stretch ratio of z ⫽ 1.4). The Cauchy stress is seen to be significantly elevated in the experimental group (P ⫽ 0.032) while the Green strain remains unchanged (P ⫽ 0.949). This finding reflects the restoration of circumferential strain at elevated stress. MPM was used to study the remodeling of the threedimensional structure of elastin and collagen of intact, unstained tissue. The specimen generated TPEF signals from elastin and SHG signals exclusively from collagen for the excitation wavelength used (800 nm) (49). Figure 5 illustrates two-dimensional (230 ⫻ 230 m) representative visualizations of coronary arterial walls at 40⫻ magnification. The images Table 1. Characteristics of RVH model n Body wt, kg Heart wt, g RV/(LV⫹S) RV pressure, mmHg Systemic BP, mmHg RCA flow rate, ml/min RCA diameter, mm WSS, dyn/cm2 WT, mm WTA, mm WTI-M, mm z Control RVH 5 43.4⫾5.0 220⫾22.0 0.31⫾0.01 31.2⫾0.88 64⫾6 39.9⫾4.03 3.61⫾0.17 10.7⫾0.55 0.48⫾0.043 0.20⫾0.017 0.28⫾0.025 1.40⫾0.00 5 43.7⫾1.90 252⫾24.7 0.73⫾0.093* 80.9⫾11.8* 68⫾8 81.3⫾13.1* 4.16⫾0.16* 12.5⫾1.84 0.46⫾0.028 0.20⫾0.012 0.26⫾0.015 1.43⫾0.01* Values are means ⫾ SE; n ⫽ no. of pigs. RVH, right ventricular hypertrophy; RV, right ventricle; LV, left ventricle; S, septum; BP, blood pressure; WSS, wall shear stress; WT, vessel wall thickness for right coronary artery, RCA; WTA, adventitial layer thickness; WTI-M, intimal-medial layer thickness; z, axial stretch ratio. *Statistically significant difference between the 2 groups (P ⬍ 0.05). J Appl Physiol • VOL Fig. 2. Representative example of a comparison of the incremental stressstrain relationships of a control and flow-overload RCA. Pressure was varied in the 80- to 120-mmHg range and axial stretch ratio (z) was varied from 1.3 to 1.5. 106 • APRIL 2009 • www.jap.org Downloaded from http://jap.physiology.org/ by 10.220.33.4 on May 7, 2017 Pressure-overload in the right ventricle was induced by stenosis of the PA for 4 wk which led to hypertrophy of the right ventricle and hence an increase in RCA flow. Table 1 summarizes the characteristics of the experimental group relative to controls. The systolic RV pressure increased significantly after banding (159% of control value after 4 wk). The increase in RV mass was also significant as reflected by the 138% increase in RV/(left ventricle ⫹ septum) ratio compared with control hearts. The mean arterial blood pressure was not significantly different in the two groups (64 ⫾ 6 vs. 68 ⫾ 8 mmHg for control and experimental groups, respectively). The flow rate in the RCA increased by ⬃104% from a mean control value of 39.9 ml/min. The inner diameter of the RCA increased approximately by 15% which nearly normalized the WSS to the control value of ⬃10 dyn/cm2. The pressure-outer diameter relationship for the experimental and control animal is shown in Fig. 1. It is clear that the remodeled vessel has a larger outer diameter at any given pressure. This also reflects the changes in the inner diameter since the vessel wall thickness (including intima-medial and adventitial layer) is not significantly different in the two groups as shown in Table 1. The inner diameter was calculated, using the incompressibility assumption, from the outer diameter, the axial stretch ratio, and the no-load area as per Eq. 2 in the APPENDIX. Figure 1 also demonstrates a greater rate of change in diameter at lower pressures for the control compared with the experimental vessel which indicates loss of compliance in the experimental vessel. The circumferential strain and stress were computed according to Eqs. 1a and 3, respectively (APPENDIX), in reference to the zero-stress state. The zero-stress state can be characterized by the opening angle which was found to decrease from 156 ⫾ 17.8 degrees in the control to 131 ⫾ 10.5 degrees in the experimental group. The incremental circumferential stressstrain data are shown in Fig. 2 for various z of a control and experimental animal. The leftward shift and increase in slope suggest stiffening of the vessels in the experimental group. The axial strain and second Piola-Kirchhoff stress were also com- STIFFER RCA IN FLOW-OVERLOAD Fig. 3. Data (in kPa) of circumferential (Y11), axial (Y22), and cross (Y12 ⫽ Y21) incremental elastic moduli for control (mean stress of 32–53 kPa) and experimental (mean stress of 42– 63 kPa) RCA. *Statistically significant difference between the 2 groups (P ⬍ 0.05). J Appl Physiol • VOL and elastin (79%) for the wall. In the wall, collagen increased significantly from an average value of 11.6 ⫾ 0.40 to 37.7 ⫾ 2.8% (P ⬍ 0.001). Elastin also increased significantly in the wall from 6.6 ⫾ 0.87 to 11.8 ⫾ 1.2% (P ⫽ 0.007) for the control and experimental stacks, respectively. Figure 6 summarizes the collagen-to-elastin (C/E) ratios of the wall and individual layers (media and adventitia) of the control and remodeled vessels. From Fig. 6, the C/E ratio for the media increased significantly from a value of 4.0 ⫾ 0.53 to 6.6 ⫾ 0.38 (P ⫽ 0.005). In the adventitia, there was no significant change in the C/E ratio in the experimental group (1.1 ⫾ 0.10 vs. 1.3 ⫾ 0.12; P ⫽ 0.392). The C/E ratio of the wall increased significantly from 1.8 ⫾ 0.23 to 3.3 ⫾ 0.33 (P ⫽ 0.008). To further examine the changes in the arterial wall, and to evaluate smooth muscle hyperplasia, histological sections were prepared. Figure 7 demonstrates the arterial wall from a control (Fig. 7A) to a remodeled (Fig. 7B) vessel. Elastic fibers are visualized in blue-black to black, collagen is pink to red, nuclei are blue to black, and other tissue elements are yellow to brown. The number of nuclei per millimeter squared section area did not change significantly from 616.7 ⫾ 56.5 to 569.9 ⫾ 53.7 (P ⫽ 0.285) for the control and experimental segments, respectively. The small and insignificant difference (8%) in nuclei per area confirmed the absence of hyperplasia in this study. The images in Fig. 7 represent between 15 to 20% of the vessel ring circumference. DISCUSSION Previous studies established that the mechanical properties of vessels are essentially determined by the matrix components of the wall (49). Thus, changes in composition and structure of the wall will result in altered vessel wall mechanics. Here, we show that flow-overload induces an increase in the elastic moduli in the axial and circumferential directions (increase in stiffness). In the present model, the microstructural basis for the increase in stiffness correlates with an increase in elastin and collagen in the media and particularly in the adventitia layer. This underscores, in the RCA, the importance of the adventitia during expansive remodeling. Flow-overload model. Our current model of RVH has the effect of flow increase in the RCA (Table 1) with no change in pressure (40). In this model, the banding or “obstruction” of the Fig. 4. Means ⫾ SE of Cauchy stress (kPa) and Green strain at physiological loading (pressure of 100 mmHg and axial stretch ratio of 1.4) for control and experimental RCA groups. *Statistically significant difference between the 2 groups (P ⬍ 0.05). 106 • APRIL 2009 • www.jap.org Downloaded from http://jap.physiology.org/ by 10.220.33.4 on May 7, 2017 demonstrate raw data of an overlay (top left) of SHG/TPEF along with individual signals (top middle: SHG; top right: TPEF) obtained from the porcine RCA wall for a control (Fig. 5A) and remodeled (Fig. 5B) specimen. Through overlapping of both SHG and TPEF, a high-contrast image that shows structural details of the adventitia and media is attained. The bottom rows of Fig. 5, A and B, illustrate black and white representations of the top row (collagen and elastin) with the brightness and contrast adjusted for optimum visualization. These images correspond to ⬃8.3 to 12% of the wall circumference. For a semiquantitative analysis, the imaged slices of the entire wall thickness of coronary specimens were processed with the ImageJ software available from the National Institutes of Health. The elastin and collagen contents were analyzed for their relative area fractions, calculated with respect to the total area in the region of interest. Table 2 summarizes the average area measurements (per two-dimensional image) of elastin and collagen in the wall and individual layers (media and adventitia) of the control and experimental groups. Table 2 also includes the percent change in elastin and collagen content in the wall and individual layers (media and adventitia) for complete stacks from control and experimental groups. Values for the wall correspond to a region of 230 ⫻ 230 m and values for the individual layers (media and adventitia) correspond to localized 50 ⫻ 50-m regions of interest within the wall. The values were normalized for stack size which ranged between 42 and 115 images (21–57.5 m). Table 2 shows that collagen increased significantly in the media and adventitia by ⬃91 and 112%, respectively. In the media, the average percent content of collagen increased significantly from 19.8 ⫾ 0.86 to 37.9 ⫾ 3.0% (P ⬍ 0.001) for the control and experimental stacks, respectively. In the adventitia, collagen increased significantly from an average percent content value of 28.5 ⫾ 1.01 to 60.5 ⫾ 2.04% (P ⬍ 0.001). Elastin, however, had no significant change in the media (9% of control value) but increased significantly in the adventitia by ⬃80% (Table 2). In the media, the elastin did not change significantly from an average percent content value of 5.3 ⫾ 0.74 to 5.8 ⫾ 0.36% (P ⫽ 0.578) for the control and experimental stacks, respectively. In the adventitia, elastin increased significantly from 25.7 ⫾ 2.4 to 46.4 ⫾ 3.0% (P ⬍ 0.001). Table 2 also shows a significant increase in collagen (226%) 1341 1342 STIFFER RCA IN FLOW-OVERLOAD Downloaded from http://jap.physiology.org/ by 10.220.33.4 on May 7, 2017 Fig. 5. Two-dimensional visualization [2-photon excited fluorescence (TPEF)/second-harmonic generation (SHG)] of coronary arterial walls (cross sections containing adventitial, medial, and intimal layers of RCA). The images are 230 ⫻ 230 m. The excitation wavelength is z ⫽ 800 nm. A: control segment. B: experimental segment. Top, middle: collagen (from SHG). Top, right: elastin (from TPEF). Left: overlap of the signals. Bottom: illustrates black and white representations of the collagen and elastin in the top. Magnification 40⫻. J Appl Physiol • VOL 106 • APRIL 2009 • www.jap.org STIFFER RCA IN FLOW-OVERLOAD 1343 Table 2. Average area measurements (per 2D image) of elastin and collagen in RCA Wall Elastin Collagen Media Elastin Collagen Adventitia Elastin Collagen Control RVH %Change in Content 3,517⫾459 6,132⫾211 6,278⫾618* 19,994⫾1,485* 79%* 226%* 132⫾19 494⫾21 144⫾9 946⫾75* 9% 91%* 642⫾60 710⫾25 1,157⫾75* 1,508⫾51* 80%* 112%* Values are means ⫾ SE (m2). Values for the wall correspond to a region of interest of 230 ⫻ 230 m and values for the individual layers (media and adventitia) correspond to localized 50 ⫻ 50-m regions of interest. *Statistically significant difference between the 2 groups (P ⬍ 0.05). 2D, 2-dimensional. Fig. 6. Summary of collagen-to-elastin (C/E) ratios of the RCA wall and individual layers (media and adventitia) for control and remodeled (flowoverload) groups. *Statistically significant difference between the 2 groups (P ⬍ 0.05). J Appl Physiol • VOL Fig. 7. Representative histological sections of RCA cross-sections. A: control segment. B: experimental segment. Remodeling of adventitia and microstructure. The use of MPM for the visualization of elastin and collagen in the remodeled wall is novel to this study. Previous studies employed tissue processing techniques to quantify only the content of collagen and elastin but not the arrangement of structure (49). MPM allows for the visualization and quantification of collagen and elastin (Fig. 5) without the need for staining, processing, or digestion techniques. This new approach allows for visualization of the three-dimensional structure which is fundamental for future microstructural modeling. Although previous studies utilized MPM to detect microscopic anatomical changes in vessels (49), this study is the first to utilize the three-dimensional rendering capabilities to measure changes in content (Table 2). The individual wall components (mainly collagen and elastin fibers) are loaded sequentially which is the cause of the nonlinear response in the stress-strain relationship (49). Elastin (with a low elastic modulus) is preferentially the initial loadbearer, while collagen (with a high elastic modulus) is recruited as the load causes a high stretch. The variation of the incremental elastic moduli, therefore, is said to be an indicator 106 • APRIL 2009 • www.jap.org Downloaded from http://jap.physiology.org/ by 10.220.33.4 on May 7, 2017 PA causes a pressure increase in the right ventricle which leads to concentric hypertrophy, an adaptation of the ventricle to reduce myocardial wall stress (18). Consequently, an increase in RV mass develops which increases the blood supply demand and therefore necessitates a gradual increase in flow in the RCA as reported previously using microsphere blood flow measurements (48). Remodeling of RCA stiffness in RVH. Although the increase in stiffness is a well-known phenomenon in the hypertensive vessels (3, 7, 21), vascular enlargement in flow-overload has previously been considered a physiological response to restore the WSS. This is the first study to demonstrate increased stiffness of a blood vessel in chronic flow-overload (Figs. 2 and 3). Here, we quantitatively characterized the change in mechanical properties (Fig. 3) for the intact artery ex vivo. The literature on the mechanical properties of isolated remodeled vessels is very limited (28). Those that do provide mechanical data focus only on distension with no regard to the axial stretch (28). Our study shows that differences in axial strain between normal and remodeled vessels are significant (Figs. 3 and 4). Other studies focused primarily on residual strain measurements of opening angles (10, 20). Although this is important, it does not provide a thorough understanding of the mechanics of the vessel wall. Our study is the first to quantify the three incremental elastic moduli of a remodeled vessel in reference to the zero-stress state (Fig. 3). 1344 STIFFER RCA IN FLOW-OVERLOAD J Appl Physiol • VOL implies that the vascular system closely regulates the degree of deformation. The regulation of strain was clearly observed in the animal model after 4 wk of flow-overload (Fig. 4). Remodeling of the zero-stress state. Fung (9) previously proposed that the remodeling of the zero-stress state is an index of the nonuniformity of growth and remodeling. Fung and Liu (10, 12, 35) showed that hypertension induces growth of intima that exceeds that of the adventitia. Consequently, the vessel sector (in the zero-stress state) shows an outward bend and hence an increase in the opening angle. Conversely, Lu et al. (39) showed that flow-overload induces growth of adventitia that exceeds that of intima which is consistent with our current findings in the flow-overload model of RCA (Table 2). Hence, the vessel sector bends inward and decreases the opening angle as reported in this study. In summary, hypertension and flowoverload have opposing effects on the opening angle. In models of simultaneous hypertension and flow-overload, the effects of opening angle were found to be conciliatory (25). Comparison with other studies. Our group recently determined the values of the elastic moduli of a normal intact RCA and its layers (intima-media and adventitia) in normal pigs (37). Although the results are generally similar for a control vessel, a methodological difference should be noted. A major difference between our previous and present measurements is the implementation of ultrasonic crystals for the measurement of dimensions during loading (see Fig. 1). This allows for continuous data acquisition during testing of a vessel and hence reveals primarily the elastic response. This differed from previous studies where a camera was used to take snapshots to record dimensions at discrete points in which relaxation of stress as well as creep may have occurred. To our knowledge, there are no equivalent data on the coronary arteries in flowoverload. Critique of methods. The extent of manipulation of the RCA for placement of a flow transducer warrants a comment. The site of placement of the transducer was proximal to the vessel emergence from the aorta and the site of testing of measurement was 3–3.5 cm away. Hence, the vessel of interest was sufficiently far away from area of injury. We compared vessels in models with and without the placement of a flow transducer and found no significant differences. Histological examination verified the lack of injury in the vessel wall (Fig. 7). Stress-strain behavior and the incremental elastic moduli were implemented to quantitatively describe the stiffness of the isolated RCA. A limitation here is that we focused on a relatively small pressure range (80 –120 mmHg) to linearize the stress-strain curves. Although this is sufficient to determine the in vivo properties, a full range of deformation analysis would allow a more thorough understanding of the biomechanical behavior of these vessels. Finally, we considered the vessel wall as a homogenous structure. Given that the incremental moduli are layer (intima-media and adventitia) dependent, the methods employed in this study should be applied to the individual layers to investigate their role and contribution to the remodeling of the coronary artery. Significance of study. Stress and strain are intimately related to tissue function, growth, and remodeling. Hence, a thorough understanding of the stress and strain state in normal and diseased vessel wall can be used to predict vascular dysfunction. Here, we observed changes in vascular stiffness that 106 • APRIL 2009 • www.jap.org Downloaded from http://jap.physiology.org/ by 10.220.33.4 on May 7, 2017 of vessel structural composition, and is observed to change significantly with vascular remodeling. In this study, the collagen content increased significantly both in the media and adventitia (Table 2). Elastin, on the other hand, had almost no change in the media, although there was a significant increase in the adventitia. The increase in microstructural content did not significantly affect the vessel wall thickness (Table 1), suggesting a nonuniform growth. A prevailing growth in the adventitial layer concurrently with an unchanging wall thickness is consistent with previous flow-overload studies (39). From Fig. 6, the results show an increase in the C/E ratios of ⬃77.5% overall (wall), 63% in the media, but only 12% in the adventitia from control to experimental vessels. These data suggest that RVH stress stimulates the induction of collagen more rapidly than elastin in the media but at a similar rate in the adventitia. The significant increase in collagen and elastin, particularly in the adventitial layer, may explain the increase in stiffness in our model. This shift in microstructural composition may adversely affect or limit the vessel’s functional abilities. Thus, the previously thought physiological compensatory enlargement in flow-overload (Fig. 1) may lead to vascular dysfunction. Uniform shear hypothesis. The remodeling of blood vessels in response to flow-overload obeys the constant WSS hypothesis (23, 39). This principle implies that the volumetric flow rate is proportional to the cube of the vessel radius assuming a laminar, incompressible, Newtonian flow through a rigid cylindrical vessel (24). Hence, to maintain a constant WSS, the cube of the radius must increase in proportion to the increase in blood flow. Blood vessels accommodate such a change in vessel radius acutely through vasoactive regulation, and chronically by remodeling vascular caliber, and thus maintaining homeostasis (25). The RCA was found to undergo enlargement of the caliber (Fig. 1) to restore the WSS (Table 1) which is consistent with previous studies in other vessels (2, 25, 30, 32). Uniform circumferential stress and strain hypothesis. An increase in mean circumferential wall stress (Fig. 4) was expected, according to APPENDIX Eq. 3a, because the vessel dilates (increases in radius) in flow-overload with no significant change in wall thickness (see Table 1). This is consistent with Girerd et al. (15) who reported a 51% increase in circumferential stress despite normalization of WSS in an arterialvenous (a-v) fistula of patients with end-stage renal disease (ESRD). The strain, on the other hand, normalizes to the control values fully after 4 wk (Fig. 4). These findings are in agreement with our previous longitudinal hypertension and flow-overload studies (5, 39). In both models, strain reached its peak sooner and normalized faster than mean wall stress. Hence, we concluded that the vessel appears more “sensitive” to changes in strain which implies the enforcement of a homeostatic state of strain. In support of the notion of strain homeostasis in the vascular system, Guo and Kassab (17) recently determined the distribution of circumferential stress and strain along the porcine aorta and throughout the coronary arterial tree. They showed that the circumferential stretch ratio and average wall stress varied from 1.2 to 1.6 and 10 to 150 kPa, respectively, along the aorta and the entire left anterior descending coronary arterial tree (more than 3 orders of magnitude difference in vessel diameters). The relative uniformity of circumferential stretch ratio from the proximal aorta to a 10-m arteriole 1345 STIFFER RCA IN FLOW-OVERLOAD APPENDIX Theoretical Formulation The circumferential deformation of an artery may be described by the midwall circumferential Lagrangian-Green strain, which is defined as follows 1 E ⫽ 共 2 ⫺ 1兲 2 (1a) where is the midwall stretch ratio ( ⫽ c/C, where c refers to the midwall circumference of the vessel in the loaded state and C refers to the corresponding midwall circumference in the zero-stress state). Similarly, the axial Green strain is given by 1 E z ⫽ 共2z ⫺ 1兲 2 (1b) where z is the axial stretch ratio (defined as the change in axial length between loaded and no-load state). The midwall circumference in the loaded state was computed from the average of inner and outer diameter. The inner diameter (Di) of the vessel can be computed from the incompressibility condition for a cylindrical vessel as 冑 D i ⫽ Do2 ⫺ 4Ao z (2) where Do and A0 are outer diameter at the loaded state and wall area in the no-load state, respectively. Because all the quantities on the right-hand side of Eq. 2 are measured, the loaded Di can be computed. The total wall thickness (h) was computed as h ⫽ (Do ⫺ Di)/2. The mean Cauchy stress in the circumferential () is given by Laplace’s equation as ⫽ PD i 2h (3a) where P is the luminal pressure. The second Piola-Kirchhoff circumferential stress (S) is related to the Cauchy stress by S ⫽ 2 o Similarly, the axial second Piola-Kirchhoff stress (Sz) is given by Sz ⫽ 冋 册 4F 1 PD2i 2 2 2 ⫹ z 共Do ⫺ Di 兲 2h共Do ⫹ Di兲 (4) where F is the axial force imposed on the vessel. Incremental Moduli If we assume the material of the blood vessel wall is homogeneous, incompressible, orthotopic, and linearly elastic, the classical theory of thin-walled elastic shells can be used to compute the linearized stress-strain relationships and hence the elastic moduli. If a small perturbation of stress and strain from a homeostatic in vivo state is considered, a linear incremental stress-strain relationship can be expressed as follows ␦S 11 ⫽ Y 11 ␦E 11 ⫹ Y 12 ␦E 22 , ␦S 22 ⫽ Y 21 ␦E 11 ⫹ Y 22 ␦E 22 (5) where Sij and Eij are components of second Piola-Kirchhoff stress and Lagrange-Green strain, respectively. The indexes 1 and 2 denote circumferential and axial directions, respectively. Y11 and Y22 are the classic incremental Young’s moduli in the circumferential and axial directions, respectively; Y12 ⫽ Y21 are denoted as cross-modulus, although they have no equivalents in classic mechanics but are necessary terms for the strain energy function (11). Although these equations are Hookean, they are not isotropic. Least-Squares Method for Determination of Elastic Moduli Three elastic moduli (i.e., Y11, Y12, and Y22) must be determined as given by Eq. 5. The method of derivation of elastic moduli is clearly outlined by Huang et al. (20). Briefly, a least-squares method is used to minimize the error between the theoretical stresses given by Eq. 5 and the experimental measurements. The result is a 3 ⫻ 3 matrix whose solution is the 3 ⫻ 1 matrix of elastic moduli 冋 A 11 0 A 12 0 A 22 A 21 A 12 A 21 A 11 ⫹ A 22 册冋 册 冋 册 Y 11 B 11 Y 22 ⫽ B 22 Y 12 B 12 (6) where n n A 11 ⫽ ⌺ n ⌬E 11 ⌬E 11 n n A 12 ⫽ A 21 ⫽ ⌺ n ⌬E 11 ⌬E 22 n n A 22 ⫽ ⌺ n ⌬E 11 ⌬E 22 n n B 11 ⫽ ⌺ n ⌬S 11 ⌬E 11 n n n n B 12 ⫽ ⌺ n ⌬S 22 ⌬E 11 ⫹ ⌺ n ⌬S 11 ⌬E 22 n n B 22 ⫽ ⌺ n ⌬S 22 ⌬S 22 and n n 0 ⌬S 11 ⫽ S 11 ⫺ S 11 , n n 0 ⌬S 22 ⫽ S 22 ⫺ S 22 , n n 0 ⌬E 11 ⫽ E 11 ⫺ E 11 , n n 0 ⌬E 22 ⫽ E 22 ⫺ E 22 , n ⫽ 0,1,2 . . . The in vivo state is denoted by n ⫽ 0 and consequently 0 0 0 0 ⫽ ⌬S 22 ⫽ ⌬E 11 ⫽ ⌬E 22 ⫽0 ⌬S 11 The symbol ␦ is dropped for convenience, but it should be recalled that the quantities of stress and strain are all defined in the incremental sense according to Eq. 5. The constants A and B are determined from the n experiments, and the matrix is solved for the three elastic moduli. ACKNOWLEDGMENTS We thank Dr. Q. Dang for excellent technical expertise. GRANTS (3b) J Appl Physiol • VOL This research was supported in part by National Heart, Lung, and Blood Institute Grants HL-087235 and HL-084529. 106 • APRIL 2009 • www.jap.org Downloaded from http://jap.physiology.org/ by 10.220.33.4 on May 7, 2017 accompanies the expansive remodeling of coronary arteries in flow-overload. Given that increased stiffness is an important risk factor for vascular dysfunction, flow-overload in RVH may predispose the RCA to endothelial dysfunction and vascular disease. In addition to cardiac hypertrophy, there are many possible clinical conditions in which the findings of this study may have an impact. Other models of flow-overload include chronic obstructive pulmonary diseases, Bernheim’s Syndrome, mitral valve stenosis, and a-v fistula used in dialysis for ESRD patients. These conditions may involve other factors which contribute to their pathology in addition to flow-overload. For instance, in patients with ESRD, the role of uremiaspecific factors (mainly calcification) may significantly affect the observed arterial stiffness (29). The influences of calcification, enzymes, cytokines, and other proteins have yet to be completely understood in these conditions. In our study, the model allowed for the determination of the effect of pure flow-overload on the RCA. The synergistic interplay of flowoverload with biochemical factors in other disease states remains to be investigated in future studies. 1346 STIFFER RCA IN FLOW-OVERLOAD REFERENCES J Appl Physiol • VOL 106 • APRIL 2009 • www.jap.org Downloaded from http://jap.physiology.org/ by 10.220.33.4 on May 7, 2017 1. Arnett DK, Evans GW, Riley WA. Artery stiffness: a new cardiovascular risk factor? Am J Epidemiol 140: 669 – 682, 1991. 2. Blacher J, Pannier B, Guerin A, Marchais SJ, Safar ME, London GM. Carotid arterial stiffness as a predictor of cardiovascular and all-cause mortality in end-stage renal disease. Hypertension 32: 570 –574, 1998. 3. Boutouyrie P, Tropeano AI, Asmar R, Gautier I, Benetos A, Lacolley P, Laurent S. Aortic stiffness is an independent predictor of primary coronary events in hypertensive patients: a longitudinal study. Hypertension 39: 10 –15, 2002. 4. Buus CL, Pourageaud F, Fazzi GE, Janssen G, Mulvany MJ, De Mey JG. Smooth muscle cell changes during flow-related remodeling of rat mesenteric resistance arteries. Circ Res 89: 180 –186, 2001. 5. Dang Q, Duch B, Gregersen H, Kassab GS. Indicial response of growth and remodeling of common bile duct post obstruction. Am J Physiol Gastrointest Liver Physiol 286: G420 –G427, 2004. 6. Dart AM, Lacombe F, Yeoh JK, Cameron JD, Jenning GL, Laufer E, Esmore DS. Aortic distensibility in patients with isolated hypercholesterolaemia, coronary artery disease, or cardiac transplant. Lancet 338: 270–277, 1991. 7. Dzau VJ, Safar ME. Large conduit arteries in hypertension: role of the vascular renin-angiotensin system. Circulation 77: 947–954, 1988. 8. Fulton RM, Hutchinson EC, Jones AM. Ventricular weight in cardiac hypertrophy. Br Heart J 14: 413– 420, 1952. 9. Fung YC. Biomechanics: Motion, Flow, Stress and Growth. New York: Springer-Verlag, 1990. 10. Fung YC, Liu SQ. Change of residual strains in arteries due to hypertrophy caused by aortic constriction. Circ Res 65: 1340 –1349, 1989. 11. Fung YC, Liu SQ. Determination of the mechanical properties of the different layers of blood vessels in vivo. Proc Natl Acad Sci USA 92: 2169 –2173, 1995. 12. Fung YC, Liu SQ. Strain distribution in small blood vessels with zero-stress state taken into consideration. Am J Physiol Heart Circ Physiol 262: H544 –H552, 1992. 13. Gibbons GH, Dzau VJ. The emerging concept of vascular remodeling. N Engl J Med 330: 1431–1438, 1994. 14. Gillensen T, Gillensen F, Sieberth H, Hanrath P, Heintz B. Age-related changes in the elastic properties of the aortic tree in normotensive patients: investigation by intravascular ultrasound. Eur J Med Res 1: 144–148, 1995. 15. Girerd X, London G, Boutouyrie P, Mourad JJ, Safar M, Laurent S. Remodeling of the radial artery in response to a chronic increase in shear stress. Hypertension 27: 799 – 803, 1996. 16. Green DJ, Maiorana A, O’Driscoll G, Taylor R. Effect of exercise training on endothelium-derived nitric oxide function in humans. J Physiol 561: 1–25, 2004. 17. Guo X, Kassab GS. Distribution of stress and strain along the porcine aorta and coronary arterial tree. Am J Physiol Heart Circ Physiol 286: H2361–H2368, 2004. 18. Gupta S, Das B, Sen S. Cardiac hypertrophy: mechanisms and therapeutic opportunities. Antioxid Redox Signal 9: 623– 652, 2007. 19. Hodes RJ, Lakatta EG, McNeil CT. Another modifiable risk factor for cardiovascular disease? Some evidence points to arterial stiffness. J Am Geriatr Soc 43: 581–582, 1995. 20. Huang W, Delgado-West D, Wu JT, Fung YC. Tissue remodeling of rat pulmonary artery in hypoxic breathing. II. Course of change of mechanical properties. Ann Biomed Eng 29: 552–562, 2001. 21. Izzo JL. Arterial stiffness and the systolic hypertension syndrome. Curr Opin Cardiol 19: 341–352, 2004. 22. Joannides R, Haefeli WE, Linder L, Richard V, Bakkali EH, Thuillez C, Lüscher TF. Nitric oxide is responsible for flow-dependent dilatation of human peripheral conduit arteries in vivo. Circulation 91: 1314–1319, 1995. 23. Kamiya A, Togawa T. Adaptive regulation of wall shear stress to flow change in the canine carotid artery. Am J Physiol Heart Circ Physiol 239: H14 –H21, 1980. 24. Kassab GS, Fung YC. The pattern of coronary arteriolar bifurcations and the uniform shear hypothesis. Ann Biomed Eng 23: 13–20, 1995. 25. Kassab GS, Gregersen H, Nielsen SL, Liu X, Tanko L, Falk E. Remodeling of the coronary arteries in supravalvular aortic stenosis. J Hypertens 20: 2429 –2437, 2002. 26. Kassab GS, Imoto K, White FC, Rider CA, Fung YC, Bloor CM. Coronary arterial tree remodeling in right ventricular hypertrophy. Am J Physiol Heart Circ Physiol 265: H366 –H375, 1993. 27. Khan Z, Millard RW, Gabel M, Walsh RA, Hoit BD. Effect of congestive heart failure on in vivo canine aortic elastic properties. J Am Coll Cardiol 33: 267–272, 1999. 28. Kobs R, Muvarak N, Eickhoff J, Chesler N. Linked mechanical and biological aspects of remodeling in mouse pulmonary arteries with hypoxia-induced hypertension. Am J Physiol Heart Circ Physiol 288: H1209 – H1217, 2005. 29. Kraœniak A, Drozdz M, Pasowicz M, Chmiel G, Michalek M, Szumilak D, Podolec P, Klimeczek P, Konieczyñska M, Wicher-Muniak E, Tracz W, Khoa TN, Souberbielle JC, Drueke TB, Sulowicz W. Factors involved in vascular calcification and atherosclerosis in maintenance haemodialysis patients. Nephrol Dial Transplant 22: 515–521, 2007. 30. Langille BL. Arterial remodeling: relation to hemodynamics. Can J Physiol Pharmacol 74: 834 – 841, 1996. 31. Langille BL, Dajnowiec D. Cross-linking vasomotor tone and vascular remodeling: a novel function for tissue transglutaminase? Circ Res 96: 9–11, 2005. 32. Laurent S, Boutouyrie P, Asmar R, Gautier I, Laloux B, Guize L, Ducimetiere P, Benetos A. Aortic stiffness is an independent predictor of all-cause and cardiovascular mortality in hypertensive patients. Hypertension 37: 1236 –1241, 2001. 33. Lehmann ED, Watts GF, Gosling RG. Aortic distensibility and hypercholesterolaemia. Lancet 340: 1171–1172, 1992. 34. Liu J, Sukhova G, Sun J, Xu W, Libby P, Shi G. Lysosomal cysteine proteases in atherosclerosis. Arterioscler Thromb Vasc Biol 24: 1359 – 1366, 2004. 35. Liu SQ, Fung YC. Relationship between hypertension, hypertrophy, and opening angle of zero-stress state of arteries following aortic constriction. J Biomech Eng 111: 325–335, 1989. 36. London GM, Safar ME. Arterial wall remodeling and stiffness in hypertension: heterogeneous aspects. Clin Exp Pharmacol Physiol 23, Suppl 1: S1–S5, 1996. 37. Lu X, Pandit A, Kassab GS. Biaxial incremental homeostatic elastic moduli of coronary artery: two-layer model. Am J Physiol Heart Circ Physiol 287: H1663–H1669, 2004. 38. Lu X, Yang J, Zhao JB, Gregersen H, Kassab GS. Shear modulus of coronary arteries: contribution of media and adventitia. Am J Physiol Heart Circ Physiol 285: H1966 –H1975, 2003. 39. Lu X, Zhao JB, Wang GR, Gregersen H, Kassab GS. Remodeling of the zero-stress state of femoral arteries in response to flow overload. Am J Physiol Heart Circ Physiol 280: H1547–H1559, 2001. 40. Murray PA, Baig H, Fishbein MC, Vatner SF. Effects of experimental right ventricular hypertrophy on myocardial blood flow in conscious dogs. J Clin Invest 64: 421– 427, 1979. 41. Pourageaud F, De Mey JG. Structural properties of rat mesenteric small arteries after 4-wk exposure to elevated or reduced blood flow. Am J Physiol Heart Circ Physiol 273: H1699 –H1706, 1997. 42. Salomma V, Riley W, Kark JD, Nardo C, Folsom AR. Noninsulindependent diabetes mellitus and fasting glucose and insulin concentrations are associated with arterial stiffness indexes. The ARIC Study Atherosclerosis Risk in Communites Study. Circulation 91: 1432–1443, 1995. 43. Stefanadis C, Tsiamis E, Vlachopoulos C, Stratos C, Toutouzas K, Pitsavos C, Marakas S, Boudoulas H, Toutouzas P. Unfavorable effect of smoking on the elastic properties of the human aorta. Circulation 95: 31–38, 1997. 44. Tulis DA, Unthank JL, Prewitt RL. Flow-induced arterial remodeling in rat mesenteric vasculature. Am J Physiol Heart Circ Physiol 274: H874 – H882, 1998. 45. Tuttle JL, Nachreiner RD, Bhuller AS, Condict KW, Conners BA, Herring BP, Dalsing MC, Unthank JL. Shear level influences resistance artery remodeling: wall dimensions, cell density and eNOS expression. Am J Physiol Heart Circ Physiol 281: H1380 –H1389, 2001. 46. Wang DH, Prewitt RL. Microvascular development during normal growth and reduced blood flow: introduction of a new model. Am J Physiol Heart Circ Physiol 260: H1966 –H1972, 1991. 47. Wesselman JP, Kuijs R, Hermans JJ, Janssen GM, Fazzi GE, van Essen H, Evelo CT, Struijker-Boudier HA, De Mey JG. Role of the RhoA/Rho kinase system in flow-related remodeling of rat mesenteric small arteries in vivo. J Vasc Res 41: 277–290, 2004. 48. Wyse RK, Jones M, Welham KC, de Leval MR. Cardiac performance and myocardial blood flow in pigs with compensated right ventricular hypertrophy. Cardiovasc Res 18: 733–745, 1984. 49. Zoumi A, Lu X, Kassab GS, Tromberg BJ. Imaging coronary artery microstructure using second-harmonic and two-photon fluorescence microscopy. Biophys J 87: 2778 –2786, 2004.