Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
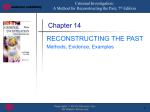
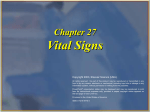
Describe the priorities of the renal nursing assessment. Identify ways in which alterations of hemoglobin and hematocrit levels can signal fluid volume deficit or excess. Explain the reason elevations of blood urea nitrogen and creatinine signal renal dysfunction. Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-1 Kidney Anatomy Both kidneys are enclosed in a renal capsule Renal cortex is the outer layer of the capsule & contains blood-filtering mechanism Renal medulla is the inner region, containing pyramids Parynchema is the functional unit of the kidney Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-2 Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-3 Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-4 Nephrons – selectively secretes & reabsorbs ions & filtrates (fluid, wastes, electrolytes, acids, bases) Glomerulus – capillaries filter large plasma proteins & blood cells Tubules (PCT, DCT, Loop of Henle) – reabsorbs electrolytes, filters fluid & converts it into urine Bowman’s Capsule - surrounds the glomeruli Glomerular filtrate (electrolytes, glucose, amino acids, metabolic waste) from the blood is filtered, enters a fluid filled space (Bowman’s space), then enters PCT (proximal convoluted tubule) Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-5 Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-6 Excretion - the removal of end waste products from body fluids Elimination - the discharge of waste products into the environment Homeostatic regulation of blood plasma Regulating blood volume and pressure Regulating plasma ion concentrations Stabilizing blood pH Conserving nutrients & controlling electrolyte balance Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-7 ADH is produced by hypothalamus and secreted from the posterior lobe of pituitary gland ADH secretion is stimulated by dehydration or high sodium intake & by a decrease in blood volume ADH makes the DCT & collecting duct permeable to water Water is drawn out of tubules by osmosis & returns to blood; concentrated urine remains in tubules to be excreted ADH is primarily responsible for reabsorption of water by the kidneys Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-8 When sodium increases, extra water is retained to preserve osmotic pressure Increased sodium & water increases blood volume & blood pressure When BP increases, glomerular filtration increases, & extra water & sodium are lost; blood volume is reduced, returning BP to normal Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-9 Increases in serum potassium stimulates the secretion of aldosterone Aldosterone stimulates the DCT to secrete potassium This action returns the serum potassium concentration to normal Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-10 Blood pH is controlled by maintaining the concentration of buffer systems Carbonic acid & sodium bicarbonate form the most important buffers for neutralizing acids in plasma Normal arterial pH is maintained by keeping the ration of concentration of sodium bicarbonate to carbon dioxide at 20:1 Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-11 Chief Complaint (onset, location, duration) Renal Symptoms ( wt. gain >2lbs./day) Predisposing Risk Factors (infections, OTCs, HTN) Medical History Previous Diagnostic Studies Current Medication Usage NSAIDs, antibiotics, HTN meds, iodine dyes) Social History and Family History Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-12 Inspection of flank & abdomen Bleeding Grey-Turner’s sign – flank discoloration (trauma) Abdominal distention or firmness Blood in urine usually indicates bladder, not kidney trauma Volume Depletion/ Overload Neck veins nondistended supine (hypovolemia); remain distended at 45° > 2cm above sternal notch (overload) Skin turgor & dryness of the mouth Edema Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-13 Edema (cont’d) Definition: the presence of fluid in interstitial space Can indicate volume overload However, loss of albumen from vascular space (d/t circulatory compromise) can cause peripheral edema with hypovolemia or normovolemia A key feature to distinguish the two is that edema does not reverse with elevation of extremity when volume overload Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-14 Auscultation Heart 3rd or 4th sound may be heard with bell of stethoscope Increased HR WITH decreased BP (hypovolemia) Friction rub – pericarditis d/t uremia Blood pressure Orthostatic hypotension = drop in SBP >20; DBP >10; or rise in HR >15 bpm Lungs – crackles, dyspnea, gasping with periods of apnea = severe acid-base imbalance Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-15 Palpation To determine shape & size of kidneys Rarely done in critically ill pts. Capturing – placing one hand posteriorly under flank & the other anteriorly below rib cage, then bringing them together while pt. exhales Right kidney is more easily palpable (lower) Abnormal: mass (cancer), irregular surface (polycystic kidney), size differences, extending significantly lower than rib cage (trauma) Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-16 Percussion Kidneys (dull is normal) – pain may indicate infection or trauma Abdomen (to assess fluid status) Ascites or severe fluid distention (dull) Fluid wave (Figure 19-1 p. 394) differentiates ascites from distortion d/t solid bowel contents Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-17 Other Observations Fluid and electrolyte imbalances Mental status changes Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-18 Weight Check weight on admission & daily Weight gain or loss > 2lbs/ day indicates fluid rather than nutritional factors Differences in wt. from day to day are used to calculate the amt. of fluid to remove during dialysis Intake and Output Urine Oliguria = <30ml/ hr or 400 ml/ day Anuria = < 100 ml/ day Insensible losses (perspiration, stool, lung vapor) Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-19 Hemodynamic Monitoring CVP – most common cause of acute renal failure requiring monitoring is severe sepsis & septic shock PAOP – “wedge pressure” MAP (70 – 100 mmHG) = SBP + (2 x DBP) 3 Cardiac Output Cardiac Index = CO BSA Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-20 Blood Serum Analysis Blood Urea Nitrogen (BUN) A by-product of protein & amino acid metabolism Normal value = 5 – 25 mg/dl Increased when kidney function deteriorates d/t increased in GFR and decreased urea excretion As BUN increases, uremia symptoms become more pronounced BUN is never evaluated in isolation (must also know creatinine level) because a decrease in GFR, therefore an increase in BUN, may also be r/t hypovolemia, dehydration, nephrotoxic drugs, or prolonged hypotension Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-21 Blood Serum Analysis (cont’d) Creatinine A by-product of muscle & normal cell metabolism Appears in serum in proportion to body muscle mass Normal = 0.5 – 1.5 mg/dl Is easily excreted by renal tubules & not significantly reabsorbed or secreted in tubules Creatinine clearance – measuring the amount of creatinine in urine & blood over 24 hrs. provides a reliable & accurate estimate of GFR (kidney function) Normal = 110 to 120 ml/ min (Box 19-3 p.396) Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-22 Blood Serum Analysis (cont’d) Osmolarility Reflects the concentration or dilution of vascular fluid & measures the dissolved particles in the vascular fluid Normal = 275 – 295 mOsm/L Elevated Osmolarility indicates hemoconcentration or dehydration Decreased Osmolarility indicates hemodilution or volume overload ADH regulates serum Osmolarility (increases to increase water resorption & decreases to increase excretion) Bedside calculation = (2 x Na) + (BUN/3) + (Gluc/18) Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-23 Blood Serum Analysis Anion Gap Is a calculation of the difference between the measurable extracellular cations (mainly Na) & the measurable intracellular anions (mainly chloride & bicarb.) Represents the remaining unmeasurable ions in the extracellular fluid (phosphates, sulfates, ketones, lactate) Normal = 1 – 12 mEq/L An increased anion gap level reflects overproduction or decreased excretion of acid products (metab. acidosis) & a decreased anion gap indicates metab. alkalosis) Na+ – (Cl- + HCO3-) Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-24 Blood Serum Analysis (cont’d) Hemoglobin and Hematocrit H & H levels can indicate increases or decreases in intravascular fluid volume Hemoglobin (Hgb) transports O2 & CO2 & is important in cellular metabolism & acid-base balance (13.5-17.5 g/dl) Hematocrit (Hct) is the proportion of RBCs in a volume of whole blood. > 54% indicates fluid volume deficit & < 37% may indicate fluid volume excess (normally 3x the Hgb level) Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-25 Blood Serum Analysis (cont’d) Albumin More than 50% of total plasma protein is albumen Is made in the liver & is responsible for maintaining colloidal osmotic pressure which hold fluid in vascular space Normal = 3.5 – 5 g/dl Blood vessel walls prevent albumen from leaving the vascular space Decreased levels of albumen creates edema (burns, sepsis, renal failure, protein malnutrition, liver disease/ injury, severe portal HTN → ascites) Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-26 Urine Analysis (Table 19-3 p.397) Urine pH Specific Gravity / Osmolality Glucose Protein Electrolytes Urea Hematuria WBC/ Bacteria Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-27 24 Hour Urine Collection (Silvestri p. 928) Creatinine clearance Uric acid test (gout & kidney disease) Vanillylmandelic test (pheochromocytoma – tumor of the adrenal gland)-avoid certain foods x 2 days Nursing Considerations Encourage fluids Avoid tea, coffee & some medications Discard 1st sample (start time)/ keep last sample (end time) Keep collections on ice or refrigerated Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-28 KUB – to evaluate presence of calculi & masses Bladder scanning (US) – bladder volume; cysts CT/ MRI – provide cross-sectional views IV Pyelography (IVP) – internal kidney tissues Renal angiography – renal blood flow Cystoscopy/ biopsy – bladder mucosa examined for inflammation, calculi or tumors Renal biopsy (closed vs. open) – to obtain kidney tissue sample Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-29 Describe the stages of acute tubular necrosis. Identify the priorities of nursing management in acute renal failure. Identify the differences among hemodialysis, peritoneal dialysis, and continuous renal displacement therapy. Describe the etiologies of acute renal failure. Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-30 Definition: characterized by a sudden decline in glomerular filtration rate (GFR) Waste product retention Electrolyte, acid-base, & fluid volume imbalances Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-31 Etiology (Box 20-2 p.402) Pre-Renal: any condition that ↓ blood flow, BP, or renal perfusion before arterial blood reaches the kidney Intra-Renal: any condition that produces an ischemic or toxic insult directly at the site of the nephron Post-Renal: any obstruction that hinders the flow of urine from beyond the kidney Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-32 Acute Tubular Necrosis (Intra-Renal): results from injury that damages the renal tubular epithelium and may extend to basement membrane Over 90% of episodes of acute renal failure are d/t ATN as a result of ischemic or toxic injury (Box 20-3) Ischemic Injury – occurs as a result of vasodilation associated w/ sepsis (prolonged hypotension or low CO) Nephrotoxic Injury – common cause is radiopaque (contrast) dye Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-33 Description Abrupt decline in glomerular filtration rate (GFR) Retention of metabolic waste products Disruption of fluid volume Mortality is high without treatment Associated complications are frequent Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-34 Pathophysiology Tubular obstruction – cellular debris accumulates due to lack of filtrate/ blood flow Tubular edema exacerbates obstruction Tubular cell injury - ischemia Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-35 Onset Phase From when an insult occurs until cell injury GFR decreases because of impaired renal blood flow & decreased glomerular filtration pressure Lasts hours to days, depending on cause If tx is initiated during this time, irreversible damage can be alleviated Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-36 Oliguric / Anuric Phase Lasts 5 – 8 days in nonoliguric patients & 10 – 16 days in oliguric patients Necrotic cellular debris in the tubular space blocks the flow of urine & causes damage to tubular wall & basement membranes GFR is greatly reduced Increased BUN (azotemia) & creatinine Hyperkalemia, hyperphosphatemia, hypocalcemia Metabolic acidosis, Changing anion gap Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-37 Diuretic Phase Lasts 7 – 14 days Characterized by an increase in GFR & sometimes polyuria Tubular obstruction has passed, but edema & scarring are present GFR returns before the ability of the tubules to function normally and the kidney can remove volume but not solutes Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-38 Recovery Phase Both oliguric & nonoliguric patients will have increased urine output Renal function slowly returns to normal or near normal If renal parenchymal damage has occurred, BUN & creatinine levels may never return to normal Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-39 Normal Laboratory Assessment (Table 20-3 p.404) Sodium: 135 – 145 mEq/L Potassium: 3.5 – 4.5 mEq/L Chloride: 98 – 108 MEq/L Calcium: 8.5 – 10.5 mg/dl Phosphorus: 2.7 – 4.5 mg/dl Magnesium: 1.5 – 2.5 mEq/L Bicarbonate: (CO2) 24 – 28 mEq/L Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-40 Assessment & Diagnosis Acidosis (pH below 7.5) is one of the trademarks of ARF Radiologic Findings – CT scan & angiography Hemodynamic Monitoring Fluid Balance Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-41 Underlying chronic kidney disease RIFLE (risk, injury, failure, loss, end-stage kidney dis.) Older Age (> 65 years) Heart Failure-HTN- or cardiovascular disease Respiratory Failure-54%-84% with ARF had Resp failure Sepsis-shock, renal hypoperfusion-inflammatory changes Trauma-crushing injuries and Rhabdomyolysis Contrast-Induced Nephrotoxic Injury(1% of all contrast procedures) Copyright © 2004, Elsevier (USA). All Chapter rights reserved. 19-42 Hemodynamic & Fluid Balance Monitoring Hemodynamic Monitoring (CVP, PAOP, CO, CI) Daily weight Physical assessment ECF depletion sx: thirst, ↓ skin turgor, lethargy Intravascular fluid overload sx: pulm. congestion, ↑ heart failure & BP Edema Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-43 Medical Management (Electrolytes) Hyperkalemia ECG changes: peaked T waves, widening QRS, VT/F Tx: diuretics; 10U insulin & 50 ml 50% dextrose (to force K into cells); Kayexalate (binds K in bowel) Hyponatremia tx w/ fluid restriction or dialysis Hypocalcemia tx w/ supplements, Vit. D & synthetic calcitrol Lower phosphorus levels (to increase calcium) with binding agents (PhosLo, Renagel, Fosrenol) Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-44 Hyperkalemia Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-45 Medical Management (Goals) Prevention Correcting the causative mechanism Regeneration of functional capacity Management is based on category of ARF Pre-renal Intra-Renal Post-Renal Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-46 Medical Management (Volume) Fluid Resuscitation (NS) for trauma, hemorrhage, hypotension, contrast dye injury Crystalloids and Colloids (volume management) Crystalloids (NS 0.9% & 0.45%, LR w/ caution-contains K) Colloids expand IV volume (albumen, Hetastarch) Fluid Restriction to prevent circulatory overload & interstitial edema with oliguria Fluid Removal – diuretics, hemodyalisis Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-47 Pharmacologic Management (Table 20-7) Diuretics stimulate urinary output (controversial) Loop (Lasix) – inhibit Na & Cl (Monitor electrolytes) Thiazides (Zaroxolyn, Diuril) – in addition to Lasix since they work on distal tubule to inhibit Na & Cl Osmotic (Mannitol) - ↑ flow of fluid from tissues by ↑ plasma osmolality K-sparing (Aldactone) – exerts (weak) effect on collecting tubule/ used in heart failure (monitor for hyperkalemia) Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-48 Pharmacologic Management (cont’d) Dopamine (renal dose) to stimulate renal blood flow Acetylcysteine (Mucomyst) to vasodilate tubule & “scavenge” free radicals Fenoldopam (Corlopam) to lower blood pressure Dietary – Phosphorous Binders Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-49 Nutrition – restrict potassium, sodium, phosphorous, protein, & fluids. Encourage carbs. Nursing Management Infection Control Optimize Fluid Balance Electrolyte Balance Prevent Anemia (kidney no longer produces erythropoitin) Patient Education Nursing diagnoses on p. 400 Box 20-3 Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-50 Hemodialyzer Exchanges of fluid, electrolytes, & toxins from blood to dialysate bath through osmosis/ diffusion Ultrafiltration – transmembrane pressure & results in fluid extraction Anticoagulation – to prevent clotting Dialysis Process (Figures 20-4 & 20-6Definition Separating from the blood Indications (Box 20-4) Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-51 Vascular Access for Hemodialysis Temporary Acute Access (Fig 20-5) Subclavian vein catheters Femoral vein catheters Permanent/ Chronic Access (Fig 20-5) AV Fistula (27%)– joining peripheral radial artery & cephalic vein AV Grafts (47%)-synthetic graft between radial artery & cephalic vein AV Shunt (23%) – temporary tunneled catheter Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-52 Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-53 Medical Management When to begin hemodialysis When and where to place vascular access Exact quantity of fluid and/ or solute removal based on lab results and weights Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-54 Nursing Management Care of hemodialysis vascular access Assess patency (thrill & bruit) Assess extremity circulation No BPs, IVs, labs Heparinize Patient education Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-55 Venous blood is circulated through a highly porous hemofilter using venous catheter (Figure 20-3) The advantage is the continuous removal of fluid from plasma, or ultrafiltrate, & IV replacement which is controlled over many hours to several days) Indications (Box 20-6) Contraindications Hematocrit > 45% Terminal illness Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-56 Four CRRT methods SCUF – Slow Continuous Ultrafiltration CVVH – Cont. Venovenous Hemofiltration CVVHD – Cont. Venovenous Hemodialysis CVVHDF – Cont. Venovenous Hemodiafiltration Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-57 Complications of CRRT (Table 20-11) Decreased Ultrafiltration Rate Filter Clotting Hypotension Fluid and Electrolyte Changes Bleeding Access Dislodgment Access Infection Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-58 Medical Management of Hemodialysis and CRRT Choice of blood purification method is a medical decision Often the acute clinical diagnosis, physician preference, availability of CRRT, & physician/ RN knowledge of CRRT are deciding factors Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-59 Nursing Management of Hemodialysis and CRRT Surveillance for side-effects of dialysis Monitoring fluid balance Accurate I & O Maintaining catheter patency Preventing infection Patient education Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-60 Indications Renal failure (uremia) Volume overload Electrolyte imbalance Hemodynamic instability Lack of access to circulation Removal of high molecular weight toxins Inability to anticoagulate (i.e.: subdural bleed) Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-61 Contraindications Recent abdominal surgery Hx of abdominal surgeries w/ adhesions/ scarring Significant pulmonary disease Need for rapid fluid removal Peritonitis Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-62 Infection – most significant risk Medical Management – used for long term end-stage renal failure Nursing Management Prevention Detection of complications (Table 20-12) p.414 Patient education for self-management Catheter placement (Figure 20-7) Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-63 Living Donor Surgery Cadaver Donor Surgery Recipient Surgery Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-64 Fluid Status Electrolyte Imbalance ↓K, ↓Mg, ↓Ca Bleeding Risk- Hct/Hgb Urine Output-q 30’, assess bladder decompression, clots Immunosuppressive Therapy Polyclonal antithymocyte/ antilymphocyte compound Monoclonal antibody compound Infection Risk Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-65 Rejection Rescue therapy if biopsy is positive High dose IV steroids (mild rejection) Monoclonal antibody (mod. to severe rejection) oral immunosuppressant (chronic rejection) Treatment goal: to create a balance among medications that allows the patient to fight off most infections & yet avoid rejection Copyright © 2004, Elsevier (USA). All rights reserved. Chapter 19-66