Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Surveys of scientists' views on climate change wikipedia , lookup
Global warming wikipedia , lookup
Attribution of recent climate change wikipedia , lookup
Effects of global warming on humans wikipedia , lookup
Public opinion on global warming wikipedia , lookup
Climate change feedback wikipedia , lookup
Climatic Research Unit documents wikipedia , lookup
Climate change in Tuvalu wikipedia , lookup
Physical impacts of climate change wikipedia , lookup
Global warming hiatus wikipedia , lookup
Climate change, industry and society wikipedia , lookup
North Report wikipedia , lookup
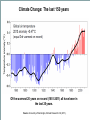
Emerging Vibrio risk in the Baltic Sea in response to ocean warming Dr Craig Baker-Austin Centre for Environment, Fisheries and Aquaculture Science (Cefas) Weymouth, Dorset, United Kingdom [email protected] EURL for monitoring bacteriological and viral contamination of bivalve molluscs. Climate Change: The last 150 years Of the warmest 20 years on record (1851-2011) all have been in the last 25 years. Source: University of East Anglia, Climate Research Unit (2011). Recent surface seawater temperature changes (IPCC fourth assessment report 2007). Source: IPCC Fourth Assessment Report (2007). Vibrio wound infections - differing levels of severity V. vulnificus. Most dangerous Vibrio pathogen. Causes necrotising (tissue death) wound infections. Very high mortality rate (20-25%), can lead to 60% mortality rate if infection progresses to septicaemia (blood poisoning). At risk groups – the elderly, diabetics, individuals with liver dysfunction and/or compromised immune systems. Picture courtesy: Ruppert et al. (2004). Picture courtesy: Ottavianii et al. (2010). V. cholerae (non O1/O139). Second most dangerous Vibrio pathogen. As with V. vulnificus can cause necrotic wound infections, although many cases involve reoccurring ear infections. Mortality rate much lower, but can increase significantly in at risk groups – particularly where the elderly, those with liver complaints, and persons with compromised immune systems are involved. V. parahaemolyticus and V alginolyticus. Amongst the least pathogenic Vibrio infections. Few fatalities, and very rarely progress to more serious infections. Can usually be treated with antibiotics and/or topical treatments. Normally cut/wound infections and ear infections associated with swimming. Picture courtesy: Reilly et al. (2011). Poleward expansion of Vibrio disease? Alaska, USA V. parahaemolyticus (2004) NW Spain V. parahaemolyticus (1999, 2004) Baltic Sea Vibrio spp. (1994, 2004, 2006) Vladivostok, Russia Vibrio parahaemolyticus (1997) Pacific NW, USA V. parahaemolyticus (1997) Chile V. parahaemolyticus (2003 ongoing) New Caledonia V. vulnificus (2008/9, 2012) y = 0.0682x + 16.359 R² = 0.679, p> 0.001 19 18.5 18 Vibrio risk threshold 17.5 17 16.5 16 15.5 2007 2002 1997 1992 1987 15 1982 Sea surface temperatures (Celcius) Average summer (June-September) sea surface temperatures, Europe 1982-2009 Year Regionally, Europe’s seas are warming faster than anywhere else on Earth Source: Baker-Austin, C., et al. (2012) unpublished data Current rates of warming White Sea – Maximum SST change: 1.49 ± 0.03 (°C/decade ± s.e.m.) Gulf of Finland – Maximum SST change: 1.00 ± 0.02 (°C/decade ± s.e.m.) Danish/German border – Maximum SST change: 0.91 ± 0.02 (°C/decade ± s.e.m.) Source: http:www.CoastalWarming.com Only one of environment on Earth warming as fast Hudson Bay, Canada – Maximum SST change: 1.44 ± 0.02 (°C/decade ± s.e.m.) Baltic Sea area – the ‘crucible of climate change’ Picture courtesy: Joaquin Trinanes, USC, Spain Sea surface salinity in Europe Optimal Vibrio growth Possible Vibrio risk? Source: Baker-Austin et al Nature Climate Change (2012). Notable recent Vibrio outbreaks in Europe Spain (1999) – 64 cases of V. parahaemolyticus traced to shellfish consumption (Lozano-León et al. 2003). Spain (2004) – 80 cases of V. parahaemolyticus. Pandemic strain (O3:K6) identified at outbreak Spain (1989) – 8 cases of V. (Martinez-Urtaza et al. parahaemolyticus associated with 2005). fish and shellfish consumption. Baltic (1989-2010) – Numerous reported cases of wound infections (Vibrio spp.) in the Baltic Sea area. Almost all recreational exposure to seawater during summer months. Numerous fatalities linked to V. vulnificus and non-O1 V. cholerae infections. Italy (2004) and France (2005) - several V. parahaemolyticus O3:K6 strains identified based on retrospective analysis of clinical cases. Sporadic V. cholerae (non O1) cases. Source: Baker-Austin, C., L. Stockley, R. Rangdale, and J. Martinez-Urtaza. Environmental occurrence and clinical impact of Vibrio vulnificus and Vibrio parahaemolyticus: a European perspective. Environmental Microbiology Reports, 2010. Baltic Sea published Vibrio cases All from 4 years...2006, 2003, 1997 & 1994 Summer (May-Sept) SST warming trends in the Baltic, 1982-2010 Key 6 12 25 50 75 Temperature (Celsius) Number of days 23 22 21 ** 20 19 18 Year Source: Baker-Austin et al unpublished (2012). 2010 2009 2008 2007 2006 2005 2004 2003 2002 2001 2000 1999 1998 1997 1996 1995 1994 1993 1992 1991 1990 1989 1988 1987 1986 1985 1984 1983 1982 17 Temperature analysis • Infrared remote sensing makes use of sensors to detect infrared radiation emitted from the Earth's surface. Satellites can be used to remotely detect and measure the thermal infrared region. This radiation is emitted from warm objects such as the Earth's surface. They are used in satellite remote sensing for measurements of the Earth's land and sea surface temperature. • For this work we have used the NOAA Polar orbiting environmental satellite datasets. The dataset available is immense. We can effectively scrutinise any region of the earth down to 1km resolution, daily from 1982-2011 for sea surface temperature (SST). Sea surface salinity data from buoys/robotic instruments. • We have also used long-term sea surface temperature records, such as the Hadley Met Office and ICES data. Accurate information goes back to the mid 19th Century (150+ years of information). Epidemiological analysis • Across Europe (and often elsewhere) Vibrio infections are not generally reported, as they are not notifiable pathogenic agents. This lack of epidemiology is problematic in terms of assessing clinical impact. • To circumvent this, we obtained information from vibrio cases in the Baltic from several different sources: 1) Published peer-reviewed papers (web of science, scopus, NCBI, internet search engines). 2) Grey literature - such as newspaper reports, bulletins from EU reference laboratories and European surveillance websites (e.g. EpiNorth, EuroSurveillance), PhD & MSc theses. 3) Official statistics - from EU countries with some reporting capacity for vibrios, such as Sweden, Finland, Germany. 4) Anecdotal reports – cases reported by experts (academic and government scientists) in and around the Baltic. • Where available, information regarding the timing, geographical location and agent responsible was subsequently gathered. Cases that were not domestically acquired were removed and where suspected (e.g vibrio cases reported during the winter) were subsequently removed from final analysis. Epidemiological data • Large number of cases reported in and around the Baltic Sea & Eastern North Sea area were identified from 1977-2010. 272 cases (96%) from Baltic Sea area. Where reported, most cases reported are V. vulnificus and V. cholerae (non O1/O139) wound infections. The vast majority reported from 1997 onwards (234 cases, 85%). • The numbers of cases appears to follow national quality of monitoring – Finland and Sweden have the best overall datasets - and highest numbers of cases (125 and 68, respectively). • Significantly, there were numerous fatalities (e.g. Sweden, Germany & Poland 2006, Germany 2003 & 2010, Denmark 1994). Most fatalities caused by V. vulnificus (10) and V. cholerae (4). • Where specific timings of infections were reported, the vast majority occurred during the summer May-October (~90 %). Several years are of particular interest: 2006 (66 cases), 2003 (19 cases), 1997 (21 cases) 1994 (21 cases) and 2010 (35 cases). Crucially, these are extremely hot summers. 2006 European heatwave • The 2006 European heatwave was an exceptional period of warm weather lasting over a month – 26th June 2006 to 30th July 2006. • Across most of western Europe, July 2006 was the warmest month since official measurements began. Temperatures peaked during the end of July in the Baltic region (24th-29th July).* • A huge number of Vibrio cases started emerging in the Baltic - V. vulnificus, V. cholerae (non-O1/O139), V. parahaemolyticus and V. alginolyticus. • Most cases were wound infections, attributed to recreational exposure to seawater. Baltic Sea -and Maximum temperature andSea clinical cases Temperature reported vibrio cases in Baltic area (1982-2010) 2006 60 22 ºC 40 21 ºC * 20 20 ºC Year Source: Baker-Austin Baker-AustinetetalalNature unpublished Climate (2012). Change (2011). 2010 2009 2008 2007 2006 2005 2004 2003 2002 2001 2000 1999 1998 1997 1996 1995 1994 1993 1992 1991 1990 1989 1988 1987 1986 1985 1984 1983 1982 0 Temperature (Celsius) Number of reported cases per year 80 Changing seasonality – more ‘vibrio’ days in the Baltic 2000-2010 1854-2010 By 2050 By 2020 (IPCC fourth assessment report 2007 Source: Baker-Austin et al Nature Climate Change (2012). Adding relevant epidemiological risk factors • Seawater temperature and salinity are not the only factors that increase potential risk of recreational (or shellfish)-associated vibrio infections. • Other physiochemical variables (e.g. Zooplankton abundance, recent mixing events etc) that are likely to play a role in reducing or increasing vibrio numbers. • We are currently in the process of using additional epidemiological risk factors alongside the salinity-temp data to refine ‘risk’. Number of reported cases as well as population density may play a significant role in determining risk levels. • Several key data issues remain here – including overall poor epidemiology data in Europe, hampering efforts to improve and refine risk models. Ave. summer temp Reported cases Baltic, 2006 Ave. salinity Population density Vibrios and future epidemiological trends • Underlying conditions. The number of people with underlying risk factors for vibrio infections are increasing steadily, across the EU and elsewhere – these include individuals with liver dysfunction, diabetes and compromised immune systems. • Ageing population. Another major risk factor for vibrio infections (particularly V. vulnificus & V. cholerae non-O1). The UN predicts that by 2050 the number of people aged over 65 will be 33%, and will have increased by 20% compared to 1950. • Contact with water. More people living by, and in contact with marine water. 30+ million people live within 5 km of Baltic – enormous potential for exposure during warm weather episodes. • Behavioural factors. Long-standing ‘old wives tale’ of washing open wounds in seawater to sanitise cuts and grazes. A major risk factor – should be discouraged, especially during summer months. Visible cases Vibrio epidemiology – the tip of the iceburg Vibrio case correctly identified and reported – data made nationally and/or internationally available to Vibrio community Data not made publically available to Vibrio community Invisible cases Vibrio not notifiable agent – data not forwarded to national or regional epidemiology centre No formal identification of agent responsible Misdiagnosis of Vibrio illness Case not serious or self limiting and subsequently not reported Source: Baker-Austin et al unpublished (2012). Challenges and opportunities • The Baltic Sea and North Sea have both recently been described as the ‘Crucible of Climate Change’. The Baltic and North Sea are the fastest warming marine ecosystems on Earth, where already huge ecosystem-level changes are being detected. There are many challenges and opportunities presented by this. • Datagaps: Huge data gaps in Europe - namely poor vibrio epidemiology, a lack of joined-up surveillance systems and a means of reporting cases to a centralised body in a timely manner. The COVIS (Cholera and Other Vibrio Illness Surveillance system) in the USA is an excellent template to improve the situation in Europe. Baltic Sea risk map, 27th July 2006 Developing a dedicated pan–European vibrio network 1. Centralised data sharing resource for vibrio experts in Europe. 2. System of reporting vibrio infections to a central body. 3. Advice for the detection, treatment and prevention of vibrio infections. 4. Centralised resource for dissemination of strains for research, diagnostic purposes etc. 5. Online resource where remote sensing-based risk maps can be accessed. COVIS report form, courtesy CDC Future work • Predicting and managing risk. Most Vibrio infections acquired in Europe are preventable. Minimising risk using appropriate education programmes for at risk groups may be an effective means of reducing the clinical impact of these pathogens. • Improving epidemiology. There is a dire need to improve the basic epidemiology of vibriosis in Europe, such as the timing, location, probable route of exposure and agent responsible. Improving the epidemiology requires coordination and effort across Europe, including clinical microbiologists, public health practitioners and epidemiologists. We have a template to achieve this though – such as reporting systems in the USA, Far East, where vibriosis is more comprehensively and systematically reported. • Availability of tools to predict, track and elucidate outbreaks. The availability of molecular tools, such as genome sequencing will allow us to identify sources of outbreaks, identifying evolutionary relationships between strains and potentially identify areas where cases may emerge. Acknowledgements • Joaquin Tristanes and Dr Jaime Martinez-Urtaza, University of Santiago de Compestela, Spain • Dr Rachel Hartnell, Dr Nick Taylor & Dr David Lees • Professor Anja Siitonen, THL, Helsinki, Finland • Professor James D. Oliver, UNC Charlotte & Dr Angelo DePaola, FDA, Dauphin Island, Alabama, USA