Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
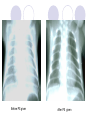
Neonatal Respiratory Distress Syndrome (NRDS ) Purpose To be familiar with etiology and mechanism To master clinical manifestation and differential diagnosis To master prevention and treatment Introduce NRDS is primarily developmental deficiency in the amount of pulmonary surfactant (PS) , at the air-liquid interface of the lung RDS also called hyaline membrane disease (HMD) Introduce RDS is a disease primarily of the premature infant Pulmonary hyaline membranes and atelectasis are findings at autopsy Etiology and Mechanism PS produced and released by type II alveolar cells PS appears after 18-20 weeks of GA Mature levels of PS are usually present after 35 -36weeks of GA Surfactant production and composition Protein (include SP-A,B,C,D) Total lipid 13% 80% Phosphatidyl choline (also called lecithin) Phosphatidylglycerol Sphingomyelin Others: Cholesterol Lysophosphatidylcholine Lecithin/ Sphingomyelin (L/S): an important index of maturation of lung (amniotic fluid) Function of PS PS cover the surface of alveolus degrade the alveolar surface tension to prevent detelectasis of alveolus stabilize pulmonary alveolar pressure prevent fluid exudation from blood capillary to alveolus. Surfactant(mcg/100g) 30 Surfactant and maturity 20 10 0 24 27 30 33 36 Gestationsal age(weeks) 39 Normal lung RDS PS ↓ → surface tension↑ → atelectasis → hypoxia and acidosis → pa vasoconstriction → right–to-left shunting → ischemic injury to the vascular bed of lung→ effusion of proteinaceous material → pulmonary hyaline membrane→ hypoxia and acidosis ↑↑ Who Is Risk baby? Preterm infant Majority of neonates with RDS are preterm infants. The incidence is inversely proportional to gestational age(GA) Who Is Risk baby? Infants of diabetic mothers (IDM) promote Glucocorticoid synthesis of PS restrain High concentration of insulin Synthesis of PS decrease when PH, temperature and pulmonary blood volume of body decrease. asphyxia in perinatal period, low temperature, mother with hypotension, placental abruption, placental previa, etc may induce NRDS. Clinical Manifestations 1. The infant with RDS is mostly premature 2. Respiratory distress usually occur and represent progressive worsening within 6 hours after birth Clinical Manifestations Manifestatons of respiratory distress Tachypnea: increase ventilatory capacity Flaring of alaenasi Expiratory grunt Three depression sign when inspiration Clinical Manifestations Manifestatons of respiratory distress Cyanosis Severe case presents shallow respiration, respiratory rhythm irregular, apnea. Physical examination: thin and flat of bony thorax, respiratory sound is weak, fine moist rales when exudation in alveolus. Clinical Manifestations 3.Patent ductus arteriosus (PDA): with recovery of patient’s condition, pulmonary pressure decrease, about 30%of patients present PDA. If patient’s condition of NRDS is obviously improved, sudden present demand for oxygen increasing, metabolic acidosis difficult corrected, difficult feeding, apnea, and continuous machinery murmur, like rolling thunder on L 2nd intercostal space can be heard, PDA should be considered. 4. The clinical manifestation is progressive worsening. Uncomplicated cases are characterized by worsening of the disease for 2~3 d with recovery at 72 hr 5. If respiratory distress occur after 12hr, NRDS should not be considered commonly. Auxiliary examination laboratory examination X-ray laboratory examination Gastric fluid oscillation test (foam test) Fetal lung maturity mensuration L/S of amniotic fluid L/S ≥2 fetal lung maturity L/S 1.5~2 doubt L/S<1.5 immaturity X-ray Ground glass air bronchogram white-out lung pulmones present universalistic permeation decrease a fine reticular granularity of the parenchyma universalistic alveolus atelectasis aerated bronchus clear display the whole lung field is white Treatment 一. Specific therapy 1. Surfactant replacement such as Survanta, Exosurf , Curosurf PS should be given under conditions of mechanical ventilation. adequate PS should be given as soon as diagnosis, within 24hr, through trachea, 2-4times according to disease. Before PS given After PS given 2.Continuous positive airway pressure (CPAP) Indication:FiO2(fraction of inspiratory oxygen)>0.4, PaO2<50mmHg or TcSO2<90%. CPAP may be administered by nasal prongs, veil, tracheal intubation 3. mechanical ventilation Indication: ⑴FiO2=0.6, PaO2<50mmHg or TcSO2<85%(exclude congenital heart disease). ⑵PaCO2>60-70mmHg and PH<7.25 ⑶severe or drug ineffective apnea 4.Closure of the patent ductus arteriosus(PDA ) Limit volume of fluid indomethacin , 0.2mg/kg.time, at 0,12, 36hr after diagnosis. Surgery 二 . Supportive management 1. Maintain a neutral thermal temperature 2. Administer adequate fluids and electrolytes, prevent fluid overload. 3. Correct acid-base disturbances 4.oxygen modus: nasal catheter veil head net monitor FiO2(fraction of inspiratory oxygen) keep PaO250~70mmHg and TcSO2 90%~ 95%(transcutaneous oxygen saturation) 5. antibiotic principle: shouldn’t be used. If infection of newborn occur, antibiotic should be used. Prevention 1. Prevent premature labor 2.Predict the risk of RDS by testing of amniotic fluid : ( L/S >2.0 ), indicates fetal lung maturity 3.Accelerate fetal lung maturation Administration of Dexamethasone to women 48hr before delivery 4. Administration PS If infant is preterm (24~34week of GA), PS should be given within 30 min, not more than 24hr after birth. Differential diagnosis 1. Meconium pneumonitis(胎粪性肺炎) Gestational age Full term infant Etiology Hypoxia History Meconium –stained amniotic fluid Clinical manifestations Signs appear quickly after birth, barrel-shaped chest, Prolonged expiration, and rales may be audible. Hyperinflation, irregular, streaky densities with areas of atelectasis, Pneumothorax Radiologic features Differential diagnosis 2.Wet lung (transient tachypnea of newborn, TTN) Gestational age Etiology fullterm infant absorption of amniotic fluid delay Clinical manifestations tachypnea after few hours (>60~80time/min) feeding well crying aloud, reflex good Radiologic features Hyperinflation Lung markings increase, patch shadow symptomatic treatment recovery after 2-3days. 3. Infectious pneumonia Gestational age Each Gestational age Etiology Bacteria, virus and other microbe History Infection, Prolonged rupture of membranes, URI Clinical manifestations May occur at any time with nasal obstruction, coughing, Tachypnea Radiologic features The sign is indefinite Pneumonia