Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
9.18
Metal Complexes as Drugs and
Chemotherapeutic Agents
N. FARRELL
Virginia Commonwealth University, Richmond, VA, USA
9.18.1 INTRODUCTION
9.18.1.1 Biological Assays
9.18.2 PLATINUM COMPLEXES AS THERAPEUTIC AGENTS
9.18.2.1 Clinically Used Anticancer Agents. Cis-platinum Compounds
9.18.2.2 Platinum Compounds in Clinical Trials
9.18.2.2.1 AMD473 (ZDO-473)
9.18.2.2.2 JM-216 (Satraplatin)
9.18.2.2.3 Poly (di and tri)-nuclear platinum complexes
9.18.2.2.4 Transplatinum compounds
9.18.3 NONPLATINUM ANTICANCER AGENTS
9.18.3.1 Ruthenium Complexes
9.18.3.2 Arsenic Trioxide
9.18.3.3 The Mitochondrion as Target. Gold–phosphane Complexes
9.18.3.4 Manganese-based Superoxide Dismutase Mimics
9.18.3.5 Titanium Compounds
9.18.3.6 Gallium Nitrate
9.18.4 ANTIBACTERIAL AGENTS
9.18.4.1 Silver and Mercury Salts
9.18.4.2 Bismuth-containing Antiulcer Drugs
9.18.4.3 Metal-containing Drugs as Antiparasitic Agents
9.18.5 PHARMACODYNAMIC USES OF METAL COMPLEX DRUGS
9.18.5.1 Lithium Carbonate
9.18.5.2 Vanadium Complexes in Diabetes
9.18.5.3 Gold Compounds as Antiarthritic Agents
9.18.5.4 Nitric Oxide in Physiology and Medicine
9.18.5.5 Lanthanum Carbonate
9.18.6 REFERENCES
9.18.1
809
810
812
812
817
817
818
819
823
825
825
826
827
827
829
830
830
830
831
831
832
832
833
833
834
834
834
INTRODUCTION
The medicinal uses and applications of metals and metal complexes are of increasing clinical and
commercial importance. Monographs and major reviews, as well as dedicated volumes, testify to
the growing importance of the discipline.1–11 Relevant reviews are to be found throughout annual
series, for example Metal Ions in Biological Systems12 and Coordination Chemistry Reviews.13
The field of inorganic chemistry in medicine may usefully be divided into two main categories: firstly,
ligands as drugs which target metal ions in some form, whether free or protein-bound; and
secondly, metal-based drugs and imaging agents where the central metal ion is usually the key
feature of the mechanism of action.14 This latter class may also be conveniently expanded to
include those radionuclides used in radioimmunoimaging and radioimmunotherapy (Chapter 9.20).
A reasonable estimate of the commercial importance is approaching US$5 billion annually
809
810
Metal Complexes as Drugs and Chemotherapeutic Agents
for the whole field. A list of clinically used chelating agents may be found in most pharmacopoeia,15
while new chelating agents continue to be sought.15,16 The use of chelating agents in the treatment
of Wilson’s disease is a good example of how medical problems due to free metal ion (CuII)
toxicity may be ameliorated by chelating agents.17 The extensive work on matrix metalloproteinases likewise represents a case study in design of small organic ligands as drugs to inactivate a
metalloenzyme.18,19 Overexpression of these zinc-containing enzymes is associated with several
diseases including arthritis and cancer, so inhibition of the zinc active site is a reasonable drug
development strategy. Indeed, enzymatic zinc is an attractive target because of the diversity of its
structural and catalytic roles in enzymes.20,21 This chapter is restricted to the uses of well-defined
inorganic compounds as drugs and chemotherapeutic agents. Current uses and prospective uses, as
well as those of essentially historical relevance, are covered. An important distinction to be made is
between drugs as chemotherapeutic agents, whose function is to kill cells, and drugs acting by a
pharmacodynamic mechanism—whose action must be essentially reversible and/or short-lived.22
9.18.1.1
Biological Assays
Most therapeutic agents and drugs will first be tested in tissue culture on a suitable model system. For
prospective anticancer drugs, for example, in vitro data obtained by proliferation or colony formation
assays give useful initial information on the cytotoxicity of the agents. The preponderance of human
tumor tissues now available with well-defined genetic makeup and detailed information of up- or
downregulation of critical genes now means that the relevance of murine (mouse-derived) tumor
models such as P388 and L1210 leukemias is somewhat diminished, although useful for preliminary
data and also for historical and comparative purposes. In vivo assays also rely initially on the murine
models for determination of pharmacokinetic properties, but the use of human tumor xenografts,
while significantly more expensive than murine models, is also considered more relevant to the real
situation. In evaluating true drug efficacy, attention must also be paid to routes of administration:
a method where drug is delivered intraperitoneally to a tumor growing in the intraperitoneal cavity
(ip/ip) is common but not as relevant to a clinical situation as intravenous administration to a tumor
growing subcutaneously (sc/iv). The term ‘‘antitumor activity’’ should be reserved for data obtained
on tumor regression in animals and not used for cytotoxicity data obtained from tissue cultures.
Phase I clinical trials assess safety and dose-limiting toxicity of prospective drugs and may be
achieved with a relatively small number of patients. phase II clinical trials usually assess single-agent
efficacy in defined diseases, i.e., ovarian cancer or relapsed ovarian cancer etc.; they generally involve
many patients and may take a significant amount of time before statistically useful data are obtained.
phase III studies may assess efficacy in combination regimens, as the chemotherapy of most cancers is
treated in this manner. An overview of the drug development and approval process is available
through web sites of agencies such as the US Food and Drug Administration23 and the National
Cancer Institute Developmental Therapeutics program.24
The application of inorganic compounds to medicine requires detailed examination of the
fundamental aqueous chemistry of the proposed drug, including its pharmacokinetics, the metabolic fate in blood and intracellularly, and the effects of the drug on the target of choice.
Coordination and organometallic complexes present a wide variety of coordination spheres,
ligand designs, oxidation states, and redox potentials, giving the ability to systematically alter
the kinetic and thermodynamic properties of the complexes toward biological receptors.
The toxicology of inorganic compounds in medicinal use, especially those containing the heavy metals,
confronts the ‘‘stigma’’ of heavy metal toxicity; but therapeutic windows are rigorously defined to
minimize such side effects—the usefulness of any drug is a balance between its toxicity and activity.
The toxicity of a compound may derive from its metabolism and unwanted ‘‘random’’ protein
interactions. Human serum albumin is of fundamental importance in the transport of drugs, metabolites, endogenous ligands, and metal ions.25 The crystal structure, combined with physical and
biophysical studies, allows visualization of likely binding sites of many potential inorganic drugs.26
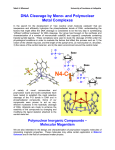
Abundant cysteine-rich small peptides, especially glutathione (GSH) (Figure 1a), and proteins such as
metallothionein27 represent detoxifying but also deactivating pathways for inorganic drugs. A further
source of metal ion/protein interactions is provided by transferrin, whose natural iron-binding site is
accessible to many metal ions of similar radius and charge including Ru2þ, Ga3þ, and Al3þ.28
The nature of the target to be attacked by any drug obviously depends on the specific
application. Many cytotoxic metal complexes target DNA because of its importance in replication
and cell viability. Coordination compounds offer many binding modes to polynucleotides, including outer-sphere noncovalent binding, metal coordination to nucleobase and phosphate backbone
811
Metal Complexes as Drugs and Chemotherapeutic Agents
(a)
HS
H
N
O
–O
O
O
N
H
O
O–
NH3+
Glutathione
O
O
H2N
H2N
OH
OH
HS
S
Methionine
Cysteine
NH2
NH2
(b)
N
N
N
O
–O
P O
O
N
–O
O
P O
O
O–
–
H
H
H
OH
H
OH
2'-Deoxycytidine-5'-Monophosphate
2'-Deoxyadenosine-5'-Monophosphate
O
O
N
N
O
–O
P O
HN
NH
N
O
O
NH2
–O
O
O–
P O
N
O
O–
H
H
OH
2'-Deoxyguanosine-5'-Monophosphate
Figure 1
N
O
O
N
H
H
OH
2'-Deoxythymidine-5'-Monophosphate
(a) Structures of common sulfur-based amino acids and tripeptides. (b) Structures of nucleic acid
monophosphates capable of metal binding.
sites, as well as strand cleavage induced by oxidation using redox-active metal centers. The purine
and pyrimidine mononucleotide building blocks are depicted in Figure 1b. The later transition
metals such as platinum and ruthenium favor binding to electron-rich nitrogens on the bases,
especially guanine N7. Titanium and early metals may display a mixture of nucleobase and
812
Metal Complexes as Drugs and Chemotherapeutic Agents
Table 1
Element
Medical and prospective medical uses of inorganic compounds.a
Compound
Uses
Approved agents (mostly US or worldwide):
Li
Li2CO3
Manic depression
Fe
[Fe(NO)(CN)5]2
Vasodilation
Ga
Ga(NO3)3
Hypercalcemia of
malignancy
As
As2O3
Anticancer agent
Ag
AgNO3
Disinfectant
Ag(sulfadiazene)
Antibacterial
Sb
SbIII(tartarate)
Pt
cis-[Pt(amine)2X2]
Au
Au(PEt3)(acetylthioglucose)
Bi(sugar)
polymers
Hg-organic
compounds
Bi
Hg
Agents in clinical trials:
Pt
Polynuclear
PtIV species
Mn
Ru
V
Ln
Mn chelates
trans-[RuCl4
(Me2SO)(Im)]
VO(maltate)2
Ln(CO3)3
Antiparasitic,
leishmaniasis
Anticancer agents
Trade names/comments
Camcolit; Cibalith-S; Lithane (of many)
Nipride. For acute shock. NO release
Ganite. Possible anticancer agent. In clinical
trials for use in lymphomas
Trisenox. Use in acute promyelocytic leukemia
Neonatal conjunctivitis
Flamazine; Silvadene; treatment of burns.
1% cream
Tartar Emetic Stibophen; Astiban
Platinol; Paraplatin; Eloxatine
Testicular, ovarian, colon cancers
Ridaura. Orally active
Rheumatoid
arthritis
Antiulcer; antacid
Pepto-Bismol; Ranitidine Bismutrex; De-Nol
Antibacterial
Thiomersal; mercurochrome (amongst many)
Antifungal
Slow release of Hg2þ
Anticancer agents
BBR3464, Satraplatin, AMD-473
Anticancer agents
Anticancer agent
Expands spectrum of activity of cisplatin;
overcomes resistance; oral activity?
SOD mimics
NAMI-A; antiangiogenic?
Type II diabetes
Hyperphosphatemia
BMOV; insulin mimetic
Fosrenol; phosphate binder
a
Principal uses as medicinal agents. Other ‘‘trivial’’ or topical uses as ointments; antacids and skin desiccants for individual elements
(especially Zn, Mg, and Al) may be found throughout.14
phosphate backbone binding. The accessibility of different oxidation states of metals such as Fe,
Cu, Co, Ru, Mn, etc. may allow for redox chemistry resulting in strand breakage. Noteworthy in
this respect is the anticancer antibiotic bleomycin, whose mode of action on target DNA is strand
scission mediated by Fe binding to the drug.29,30
Cytotoxic agents reduce the proliferation of a tumor but lack of selectivity between normal and
malignant tissue may render many agents of little clinical utility. Drug discovery in general has
been transformed by rapid advances in the understanding of the cell’s molecular biology coupled
with information sciences.31 Cancer treatment strategies especially have evolved in favor of agents
targeted toward specific pathways, notably those involved in cell signaling.32 A challenge for the
medicinal inorganic chemist is the placement of coordination chemistry within this new paradigm.
This section reviews both established and evolving approaches to uses of inorganic-based drugs
with emphasis on the most recent literature. The major clinical application and promising
preclinical areas are summarized in Table 1.
9.18.2
9.18.2.1
PLATINUM COMPLEXES AS THERAPEUTIC AGENTS
Clinically Used Anticancer Agents. Cis-platinum Compounds
Cisplatin, (cis-[PtCl2(NH3)2], also known as cis-DDP) ((1), Figure 2) is perhaps the best known
example of a small molecule metal-containing drug. The clinically used platinum complexes are
shown in Figure 2. The history of the discovery and development of cisplatin remains a remarkable scientific story.33 Its use and effectiveness in cancer chemotherapy since the entry into the
clinic in the late 1970s has been thoroughly documented.34–36 Cisplatin is cited for treatment of
813
Metal Complexes as Drugs and Chemotherapeutic Agents
O
H3N
Cl
H3N
Cl
H3N
O
Pt
Pt
H3N
H2
N
O
Pt
O
N
H2
(3)
(1)
O
(2)
O
H3N
O
O
H2
N
O
(4)
O
O
Pt
Pt
H3N
O
O
N
H2
O
( 5)
Figure 2 Structures of the clinically used platinum anticancer agents.
germ-cell cancers, gestational trophoblastic tumors, epithelial ovarian cancer, and small cell lung
cancer as well as for palliation of bladder, cervical, nasopharyngeal, esophageal, and head and
neck cancers.37–39 The use of cisplatin (usually as a principal component of combination regimens) has rendered at least one cancer, testicular cancer, curable and is significant in treatment of
ovarian and bladder cancers. Typical doses range from 20 mg/m2 to 100 mg/m2, usually for up to
five consecutive days. Despite this success, there is still a limited range of tumors sensitive to
cisplatin intervention—some cancers are inherently resistant.40,41 A further disadvantage is the
onset of clinical (acquired) resistance after treatment with the drug. The side effects of cisplatin
treatment are severe and include the dose-limiting nephrotoxicity, neurotoxicity, ototoxicity, and
emetogenesis. The ‘‘second-generation’’ compounds based on the cisplatin structure were developed in attempts to improve toxicity and/or expand the range of useful anticancer activity.
Carboplatin (2) entered the clinic in 1998, principally in response to the necessity to reduce the
toxic side effects of the parent drug. Despite this lower toxicity, carboplatin is essentially active in
the same set of tumors as cisplatin and a broader spectrum of activity is not indicated.42 For some
tumors, cisplatin appears to be therapeutically more effective than carboplatin (germ cell tumors,
head and neck, and bladder) whereas for lung cancer and ovarian cancer effectiveness is comparable.43 The choice of the most appropriate analog is a function of the cancer being treated, treatment
intention (palliative or curative), and other component drugs used in combination.
Since the advent of cisplatin in the clinic, the consistent goals for drug development have been
improvement of toxicity profile, circumvention of resistance, and expansion of the tumors sensitive
to treatment by cisplatin. The importance of circumventing resistance was recognized very early on
and reports of the activity of complexes containing 1,2-diaminocyclohexane (dach) in murine L1210
resistant to cisplatin date back to 1978.44 After approval and use in Europe for a number of years,
oxaliplatin (3) was finally granted approval for use in the US in August 2002 for colorectal cancer in
combination with 5-fluorouracil (5-FU).45,46 Little information is available on nedaplatin (4) and
lobaplatin (5), which have been approved for use in Japan and China, respectively.
DNA is accepted to be the cellular target of cisplatin. The natural sequence of scientific understanding has developed from a detailed structural understanding of the cisplatin–DNA interaction
to the biological consequences of these adducts. In this respect, the field has also kept pace with the
understanding of cellular cancer biology over the same period. Thus, it is not the DNA adduct per se
but the downstream effects of protein recognition and cell signaling events that are the ultimate
causes of cell death. In essence, the two major pathways a cell must take upon receiving an ‘‘insult’’
such as a chemotherapeutic drug, or indeed a mutagenic lesion in any fashion, are (i) to repair the
damage, or (ii) or initiate the pathway to apoptosis (programmed cell death). The factors that affect
cisplatin cytotoxicity, whether in sensitive or resistant cells, are summarized in Figure 3. DNA
damage by chemotherapeutic agents is in many cases mediated through the p53 pathway.47 Cisplatin damage to DNA stimulates apoptosis via a p53-dependent pathway, although in some cell lines
or tumor types a p53-independent pathway has been observed.48,49
Resistance to cisplatin is multifactorial and has been shown to be due to a combination of
decreased cellular accumulation of cisplatin, increased efflux of platinum from the cell,
814
Metal Complexes as Drugs and Chemotherapeutic Agents
Figure 3 A general scheme for cellular response to platinum-induced DNA damage.
increased cytoplasmic detoxification (through increased levels of cellular thiols such as GSH),
or enhanced repair/tolerance of platinum-DNA adducts.50,51 Cellular accumulation of cisplatin
is a much more complicated process than previously thought—both active and passive diffusion
pathways are now thought to exist.52 The establishment of resistant cell lines with characterized
and calibrated mechanisms of action has aided greatly in advancing a molecular approach to
overcoming resistance.53,54 Coupled with this understanding has been the necessity to understand the fate or metabolism of cisplatin in the biological milieu and explain the pharmacokinetic profile of the drug. For the purposes of this review, the major outlines of the biological
understanding will be reviewed with reference to key understandings and most recent comprehensive reviews.
The rate-limiting step in DNA binding is aquation of the PtCl bonds. The major products of
the aquation of cisplatin are the mono- and bisaqua species cis-[Pt(NH3)2(H2O)Cl]þ and
cis-[Pt(NH3)2(H2O)2]2þ, respectively (Figure 4).
Deprotonation gives inert hydroxo species, which may also form dinuclear and trinuclear
hydroxo-bridged species in concentrated solution. Calculation of the pKa of the coordinated
water molecules coupled with equilibrium constants for both aquation and deprotonation reactions allows calculation of speciation in biological medium.55,56 The compound, and its direct
structural analogs, form adducts between neighboring guanine residues on DNA, forming
d(GG) 1,2-intrastrand and d(GC) interstrand cross-links, shown schematically in (Figure 5).
Minor lesions, which have consequently received somewhat less attention, are 1,2-intrastrand crosslinks formed between an adenine and a guanine in a d(AG) adduct as well as a 1,3-intrastrand crosslink where two platinated guanines are separated by one base pair—d(GNG).
L
OH2
1+
Pt
k1a
L
k2a
Cl
L'
Cl
L
Cl
L'
Pt
L'
OH2
2+
Pt
k1b
L
Cl
1+
Pt
L'
OH2
k2b
OH2
Figure 4 Hydrolysis scheme for cisplatin-based anticancer agents. Where L ¼ L0 ¼ NH3 cisplatin is indicated.
When L ¼ NH3 and L0 ¼ 2-picoline or cha the rates of aquation of the trans-chloride ligands are different.
Metal Complexes as Drugs and Chemotherapeutic Agents
815
Bifunctional cisplatinum DNA adducts
1,2-Intrastrand cross-link
1,3-Intrastrand cross-link
Interstrand cross-link
Bifunctional transplatinum DNA adducts
Interstrand cross-link
Figure 5
Interstrand cross-link
Schematic depiction of cross-links formed by both cis- and trans-platin.
The application of {1H,15N}HSQC NMR techniques has proven to be very informative in
elucidating detailed kinetic parameters for both aquation and DNA-binding processes. Platinated
DNA may be observed at low (mM) concentrations because only 1H and 15N resonances
derived from platinum am(m)ine species are seen and the 15N shifts are strongly influenced by
the trans ligand.57,58 The monoaquated species is the most likely reactant with DNA, although
evidence has also been put forward for the importance of the cis-[Pt(NH3)2(H2O)2]2þ species in
this regard.59 The hydrolysis of carboplatin involves the displacement of the chelating cyclobutane-1,1-dicarboxylate from the coordination sphere and is unsurprisingly very slow. In the
presence of acid, the process resembles the successive displacement of two monodentate carboxylates.60 In keeping with the kinetic inertness of carboplatin, significantly higher doses are
required for both equivalent levels of DNA platination compared to cisplatin and also to generate
equitoxic and equivalent antitumor effects—clinical doses are 800–900 mg/m2.36 The benefit, of
course, is reduced nephrotoxicity as the drug may be excreted essentially intact.
The well-known affinity for sulfur binding of PtII has led to detailed study of interactions with
GSH, metallothionein, and human serum albumin.61,62 Interestingly, direct substitution of the
Pt—Cl bonds by sulfur donors such as cysteine and GSH, without the necessity for prior
aquation, is indicated from kinetic studies.63,64 Eventually, binding of the thiolate also results in
displacement of the ammonia ligands by chelation of the tripeptide moiety.65 Novel binding
modes involving N-ligation from deprotonated amide bonds as well as sulfur have been deduced
from the reaction of [PtCl2(en)] (where en ¼ ethylene 1,2 diamine) and GSH.66 Platinum-thiolate
species [Pt-RS] display a great tendency to form dinuclear bridging structures {Pt-(RS)-Pt} as
the bound thiolate is even more nucleophilic than free ligand.67 The crystal structure of [Pt2(-Nacetylcysteine)2(2,20 -bipyridine)2] confirms the bridging propensity of thiolate.68 Methionine
metabolites such as [Pt(Met-S,N)2] have been identified from the urine of cisplatin-treated
patients, emphasizing the importance of this amino acid in the biotransformation of the drug.69
The mechanism of formation has been studied—the metabolite exists predominantly as the cis isomer
(cis:trans ¼ 87:13).70 Methionine interactions with carboplatin and the formation of a stable ringopened species may provide a chemical understanding of the activation of this inert drug.71
A combination of 2D NMR techniques, chemical modification of the protein, and gel filtration
chromatography identified the dominant binding site on Human Serum Albumin (HSA) as involving
methionine rather than the expected Cys-34.62 The propensity of platinum binding to sulfur has also led
to use of sulfur compounds as rescue agents in cisplatin toxicity.63 In these cases, a balance must be
found between overcoming toxicity and reduction of antitumor efficacy through competitive binding.
The binding of Pt to DNA is irreversible and is kinetically controlled. Platinum may be removed
from DNA by strong nucleophiles such as CN. NMR methods have also provided new insight into
816
Metal Complexes as Drugs and Chemotherapeutic Agents
the kinetics and mechanism of DNA binding by cisplatin and other mononuclear analogs.
The sequence dependence on the rate constants for monofunctional and bifunctional adduct
formation have been cataloged.72 The structural consequences of bifunctional binding for the
major intrastrand and interstrand adducts have now been elucidated in great detail (Figure 6).73
The requirement to bind two adjacent guanines on the same strand of DNA to form the intrastrand
adduct, whilst maintaining the square-planar geometry of PtII, places considerable steric restraints on
the final structure. Molecular and biological studies have confirmed that the principal effect of
bifunctional intrastrand binding to DNA is a bending of the helical axis toward the major groove—
exact measurements of bending angle vary to some extent with technique but a typical value of
approximately 30–35 is often quoted from gel electrophoresis studies.72 The high resolution X-ray
crystal structure of the 1,2-intrastrand adduct in the sequence d(CCTCTG*G*TCTCC)_d(GGAGACCAGAGG) shows the helix bending of approximately 50 toward the major groove.75 The
DNA is a mixture of conformations—B-form on the 30 -side of the adduct and the more condensed
A-form on the 50 -side. In agreement with the possibility that the A-form is induced by crystal packing
forces or the concentrations of cations in the crystallization procedure, the DNA remains in the
B-form in solution.76 The d(ApG) adduct appears to be similarly kinked.77 Spectroscopic (especially
NMR) studies on the sequence dependence of the adduct have been reviewed.72,78,79 Carboplatin, as
might be expected, gives the same adducts on DNA as cisplatin since loss of the dicarboxylate
produces the same cis-{Pt(NH3)2}2þ moiety. Interestingly, the crystal structure of the oxaliplatin
adduct of the same dodecanucleotide shows the overall geometry to be very similar to the cisplatin
case, with a bending of approximately 30 toward the major groove. The enantiomerically pure
(R,R)-dach ligand results in a hydrogen bond between the pseudoequatorial NH hydrogen and the
O-6 atom of the 3-guanine, emphasizing the importance of chirality in mediating biological properties.80 These results confirm the findings that the oxaliplatin-induced damage of cellular DNA and its
consequences are very similar to those of cisplatin.81,82
The interstrand cross-link also induces DNA bending.72 X-ray and NMR studies on this adduct
show that platinum is located in the minor groove and the cytosines of the d(GC) base pair
involved in interstrand cross-link formation are ‘‘flipped out’’ of the helix stack and a localized
‘‘Z-form’’ DNA is observed.83–85 This is a highly unusual structure and very distorting—implications for differential repair of the two adducts have been addressed. Alternatively, the interstrand
cross-link of the antitumor inactive trans-DDP is formed between a guanine (G) and its complementary cytosine (C) on the same base pair.86,87trans-DDP is sterically incapable of producing
1,2-intrastrand adducts and this feature has been cited as a dominant structural reason for its lack
of antitumor efficacy. It is clear that the structural distortions induced on the DNA are very
different and likely to induce distinctly different biological consequences.
Cisplatin-adducted DNA is recognized by a host of proteins.52,72,73,88,89,90 Two general classes
of protein may be identified—those that specifically recognize the platinated sites as a first step in
their repair, and those that bind to such sites because of structural similarity to the protein’s
natural binding sites. DNA repair occurs primarily through the nucleotide excision repair pathway and proteins of the first class include the human excision repair complex, mismatch repair
proteins, XPA, and RPA (single stranded binding proteins involved in DNA replication and
repair) proteins. DNA damage induced by cisplatin is recognized by proteins containing the
B-DNA
1,2-Intrastrand cross-link
1,2-Interstrand cross-link
Figure 6 (see color plate 10) Structures of the major cisplatin/DNA adducts.
817
Metal Complexes as Drugs and Chemotherapeutic Agents
so-called high mobility group (HMG) domain motif. The exact function of these nuclear but
extrachromosomal DNA binding proteins is still a matter of debate but they bind strongly to
unusual noncanonical DNA structures, such as cruciform DNA.91 A common feature of all
HMG domain proteins is their ability to bend DNA. Several HMG domain proteins recognize
cisplatin-DNA adducts but not those of the clinically ineffective adducts of trans-DDP or the
monofunctional [PtCl(dien)]þ (where dien ¼ diethylenetriamine). This preferential recognition has
led to the suggestion that proteins with high binding affinity for cisplatin-damaged DNA may
shield the polynucleotide from cellular repair. The structural characterization of the recognition
motifs of HMG protein and cisplatin-adducted DNA give insight into the molecular details of protein
recognition.92 Domain A of the structure-specific HMG-domain protein, HMG1, binds to the
widened minor groove of a 16-base pair DNA duplex containing a site-specific 1,2-GG intrastrand
cross-link. The DNA in the protein complex is bent significantly further than in the Pt-DNA adduct
alone, and a phenylalanine moiety intercalates into a hydrophobic notch created at the platinated
d(GpG)-binding site. The importance of an intercalating protein residue such as phenylalanine in
forming the bend and in contributing to the affinity toward platinated DNA was confirmed by sitedirected mutagenesis where removal of the intercalating moiety reduced binding affinity.93
9.18.2.2
Platinum Compounds in Clinical Trials
The need for new agents in cancer chemotherapy is apparent from the inability to predictably cure
or induce remissions in common tumors such as breast, lung, colon, or prostate cancer. New
cytotoxic agents building on our experience and knowledge of the current armamentarium
continue to play an important role in the clinical management of cancer. Approximately 28 direct
structural analogs of cisplatin entered clinical trials but most have been abandoned through a
combination of unacceptable toxicity profile and/or lack of improved or expanded anticancer
efficacy.38 For new, direct structural analogs of cisplatin to find clinical use exceptional properties
would need to be found.38 Currently, there are three principal drugs ((6)–(8); Figure 7) in clinical
trials—the approaches to their development represent examples of steric control of reactivity,
control of oxidation state and ligand lipophilicity aimed at producing orally active agents, and
manipulation of new structures to produce structurally new DNA adducts.
9.18.2.2.1
AMD473 (ZDO-473)
As understanding of the mechanisms of platinum resistance has increased, more rationally
designed platinum derivatives have been synthesized. One approach has been to insert steric
O
Cl
H3N
O
H3N
Pt
N
H2 O
Pt
Cl
Cl
Cl
N
CH3
O
(7)
(6) (JM-216)
4+
H3N
NH2(CH2)6H2N
Pt
Cl
NH3
H3N
Pt
NH3
H 3N
Cl
Pt
NH2(CH2)6H2N
( 8) (BBR3464)
Figure 7 Platinum-based drugs in clinical trials.
NH3
818
Metal Complexes as Drugs and Chemotherapeutic Agents
bulk at the platinum center to retard the kinetics of substitution in comparison to cisplatin.94,95
AMD473 (cis-[PtCl2(NH3)(2-methylpyridine)], also known as ZDO-473 (7)) (AnorMED; http://
www.anormed.com) is a molecule that was designed specifically to circumvent thiol-mediated drug
resistance by sterically hindering its reaction with GSH while retaining the ability to form
cytotoxic adducts with DNA.96 GSH competes for platinum binding and may diminish DNA
platination, thus reducing cytotoxicity. The rate of aquation of AMD473 is 2–3 times slower than
that of cisplatin,97 and interstrand cross-link formation is much slower. The DNA binding is
similar to cisplatin, and the complex forms a highly stereoselective adduct on DNA, but not for
reactions with mono- and dinucleotides.98 In cell lines with previously determined mechanisms of
cell resistance, AMD473 showed little cross-resistance compared with cisplatin or carboplatin.
This partial or complete circumvention of acquired platinum drug resistance makes this a promising compound for clinical development. It is currently undergoing phase II trials where it has
shown linear pharmacokinetics and evidence of antitumor activity in ovarian cancer patients.
It has a manageable side effect profile; the dose-limiting toxicity was a reversible, dose-dependent
thrombocytopenia. Nonhematological toxicities (nausea, vomiting, and metallic taste) were mild.
No nephrotoxicity, peripheral neurotoxicity, or ototoxicity has been observed.99
9.18.2.2.2
JM-216 (Satraplatin)
Another avenue in platinum chemistry is to manipulate chemical and biological properties
through oxidation number. Indeed, the early Rosenberg studies recognized the PtIV complex
cis-[PtCl4(NH3)2] as an active anticancer agent.33 A number of PtIV compounds have since
undergone clinical trials—including cis-[PtCl4(1,2-dach)], known as tetraplatin, and cis,cis,cis[PtCl2(OH)2(PriNH2)2], known as CHIP or Iproplatin. These compounds have been abandoned
because of either undesirable side effects or lack of a significantly enhanced therapeutic range
compared to cisplatin.38 Potential oral activity of JM-216 (6) is achieved by carboxylation of the
Pt-OH groups as well as replacement of one NH3 group by the more lipophilic cyclohexylamine
(cha). Interestingly, trans-PtIV compounds were also tested because their kinetic inertness give
more reasonable in vivo activity than their analogous PtII compounds (see Section 9.18.2.2.4).100
The cytotoxicity is dependent on the reduction potential of the PtIV compound, allowing suitable
modification of pharmacokinetic parameters.101 Biological reducing agents, however, such as
GSH, reduce PtIV readily.102,103 The general synthetic scheme for JM-216 is shown in Figure 8104
In practice use of I in the first step to give cis-[PtCl(I)(NH3)(cha)] (mixture of isomers) followed
by conversion to the dichloride greatly facilitates synthesis.
–
H3N
Cl
Pt
Cl
H3N
cha
Cl
Pt
cha
Cl
Cl
H2O2
O
O
H3N
Pt
cha
O
Cl
Cl
O
R
O
O
R
OH
H3N
Pt
Cl
cha
OH
O
(6) (JM-216)
Figure 8 Preparation of JM-216.
Cl
Metal Complexes as Drugs and Chemotherapeutic Agents
819
Despite the reputed inertness of PtIV compounds, JM-216 undergoes rapid biotransformation
in human red blood cells.105 The PtII complex cis-[PtCl2(NH3)(cha)] is the major metabolite.106
The consequences of DNA binding are again similar to those of cisplatin, as expected from the
general similarity of the cis-dichlorodiam(m)ineplatinum structure.107 An interesting difference
between the cha and pyridine groups is that in the former case stereoisomers are seen in the 1,2intrastrand adduct—the cha group may reside either on the 30 or 50 end of the duplex. The
cytotoxicity of both the PtII and PtIV compounds has been examined extensively. The compound
was well tolerated orally.108,109 Interest has recently been revived in this agent.
9.18.2.2.3
Poly (di and tri)-nuclear platinum complexes
All direct structural analogs of cisplatin produce a very similar array of adducts on target DNA
and it is, therefore, not surprising that they induce similar biological consequences. This latter
consideration led to the hypothesis that development of platinum compounds structurally dissimilar to cisplatin may, by virtue of formation of different types of Pt-DNA adducts, lead to
compounds with a spectrum of clinical activity genuinely complementary to the parent drug.110–113
In terms of cellular biology, the cell signals (structure and conformation of Pt-DNA adducts as
outlined in Figure 3) must be altered to produce different cell signaling and protein recognition
and induction effects downstream of the platination event, which may be eventually reflected in an
altered pattern of antitumor activity. Polynuclear (dinuclear and trinuclear) bifunctional DNAbinding agents are amongst the best studied of these nonclassical structures. The class as a whole
represents a second, distinctly new structural group of platinum-based anticancer agents. The first
example of this class to advance to clinical trials is BBR3464 ((8), Figure 7).
The dinuclear structure is extremely flexible and capable of producing a wide series of compounds
differing in functionality (bifunctional to tetrafunctional DNA-binding), geometry (leaving chloride
groups cis or trans to diamine bridge), as exemplified in Figure 9.114 Further systematic variations
on nonleaving groups in the Pt coordination spheres (NH3 or a planar group such as pyridine or
quinoline) and linker (flexible, variable chain length) are also possible.115
The patterns of DNA modification induced by the various structural motifs have been examined and further related to cytotoxicity and antitumor activity.116,117 The necessity to concentrate
on a limited number of compounds identified the 1,1/t,t series (see Figure 9 for explanation of this
nomenclature) as having the most promising pattern of antitumor activity and DNA-binding.
Linker modifications have produced most success in terms of enhanced cytotoxicity. The presence
of charge and hydrogen bonding capacity within the central linker (either in the form of
a tetraamineplatinum moiety, or a charged polyamine linker such as spermidine or spermine),
Figure 9b, produces very potent compounds significantly more cytotoxic than the ‘‘simple’’
dinuclear species. Their biological activity varies with chain length and charge, although the
overall profile is similar.
(i) BBR3464. A trinuclear platinum clinical agent
The first polynuclear drug to enter clinical trials (in June 1998), and the first platinum drug not
based on the cisplatin structure, is the trinuclear compound denominated BBR3464 ((15), Figure 9b).
The structure, derived from general structures of trinuclear systems118 is notable for the presence
of the central Pt, which contributes to DNA affinity only through electrostatic and hydrogen
bonding interactions. The 4þ charge, the presence of at least two Pt coordination units capable of
binding to DNA, and the consequences of such DNA binding are remarkable departures from the
cisplatin structural paradigm.
In tissue culture, BBR3464 is cytotoxic at 10–100-fold lower molar concentrations than cisplatin
and displays activity in cisplatin-resistant cell lines.119 The profile of antitumor efficacy mirrors its
unique structure and is characterized by activity in human tumor (e.g., ovarian) xenografts resistant to
cisplatin and alkylating agents.120 Importantly, BBR3464 also consistently displays high antitumor
activity in human tumor xenografts characterized as mutant p53.121 These tumors are historically
insensitive to drug intervention. This important feature suggests that the new agent may find utility in
the over 60% of cancer cases where mutant p53 status is indicated. Consistently, cytotoxicity
displayed in mutant cell lines would suggest an ability to by-pass this pathway. In agreement,
transfection of p53 into p53-null SAOS osteosarcoma cells resulted in a marked reduction in cellular
820
Metal Complexes as Drugs and Chemotherapeutic Agents
Cl
H 3N
NH3
Cl
Pt
Pt
NH2(CH2)6H2N
Cl
Cl
(9)(2,2/c,c )
2+
Cl
H3N
Cl
Pt
Pt
H3N
2+
NH3
Cl
NH3
NH2(CH2)6H2N
H3N
Pt
Pt
NH3
H 3N
Cl
NH2(CH2)6H2N
(10)(1,1/c,c )
NH3
(11)(1,1/t,t)
1+
H3N
Cl
H3N
Pt
H3N
1+
Cl
NH3
Cl
Pt
NH2(CH2)6H2N
Pt
Cl
Cl
Pt
H3N
NH2(CH2)6H2N
(12 )(1,2/c,c )
Cl
(13)(1,2/t,c )
NH3
Cl
H 3N
Pt
NH3
Y
Pt
NH3
Cl
NH3
2+
(14) Y =
H2N
(15 ) Y =
H2N
NH2
NH3
N Pt
H2
NH3
(BBR3464)
(16) Y =
H2N
H2
N
(17) Y =
H2N
H2
N
4+
H2
N
NH2
4+
N
H2
NH2
3+
NH2
Figure 9 (a) Variation of structures of dinuclear platinum complexes depending on the coordination sphere of
the platinum. The structural notation describes the number of chloride ligands at each platinum center, followed
by the position of the leaving group at each site (cis or trans) with respect to the N atom of the bridging diamine.
(b) Variation of linker diamine within one class of dinuclear complexes producing both the trinuclear structure
and polyamine-bridged species.
Metal Complexes as Drugs and Chemotherapeutic Agents
821
sensitivity to BBR3464 but only a slight sensitization to cisplatin. In addition, in contrast to cisplatin,
the triplatinum complex was a very effective inducer of apoptosis in a lung carcinoma cell line carrying
mutant p53. Cell cycle analysis showed a dose-dependent G2/M arrest by BBR3464.122
In phase I clinical trials 47 patients, all of whom had previously failed standard treatments for
solid tumors, received the drug in the UK, Italy, and Switzerland on three different schedules.123,124
Dose-limiting toxicities have been defined as bone marrow depression and diarrhea. The latter is
treatable with loperamide. Signs of biological activity were seen. Notably one patient with
metastatic pancreatic cancer showed a partial response (for 4 months) and two further patients,
one with metastatic melanoma and one with bronchoalveolar carcinoma, also showed partial
responses. In a phase I trial in combination with 5-FU, a partial response in breast cancer was
observed.125 Furthermore, a reduction in tumor marker levels was observed in two patients, one
with ovarian cancer, and one with colon cancer. Phase II studies have shown partial responses in
cisplatin-resistant ovarian and nonsmall-cell lung cancer.126,127 The indications are that the profile
of clinical activity is different and complementary to the mononuclear platinum agents.
Cellular pharmacology studies showed enhanced cellular uptake of the charged polynuclear
platinum compounds in comparison to cisplatin.128,129 This in itself is very surprising given that
the ‘‘classical’’ structure–activity paradigms for platinum agents require complex neutrality. The
enhanced uptake is not sufficient to explain, by itself, the increased cytotoxicity of BBR3464.
Formation of BBR3464-induced interstrand cross-links in L1210/0 (murine leukemia) and U2-OS
(human osteosarcoma) cells peaks at the earliest time points observed. Their persistence over time
and very slow removal suggests that they are not good substrates for DNA repair. The cellular
response of HCT116 (human colon tumor) mismatch repair-deficient cells was consistent with a
lack of influence of mismatch repair status on BBR3464 cytotoxicity.121
(ii) DNA binding of polynuclear platinum compounds
The polynuclear platinum compounds stand in vivid contrast to mononuclear platinum complexes
because the predominant DNA lesions are long-range inter- and intrastrand cross-links where the
sites of platination may be separated by up to four base pairs. The consequent structural and
conformational changes in DNA are also distinct.
(iii) Aquation of dinuclear and trinuclear platinum agents
The hydrolysis profile of platinum complexes with monofunctional [Pt(amine)3Cl] coordination
spheres (e.g., mononuclear complexes such as [PtCl(dien)]þ or [PtCl(NH3)3]þ and the 1,1/t,t and
1,1/c,c dinuclear compounds of (Figure 9) differs from that of cisplatin.130 The aquation
rate constant is comparable, but the reverse chloride anation rate constant is much higher so
that the equilibrium favors the chloro form.131 For the dinuclear diaqua complex [{transPt(H2O)(NH3)}2-(H2N(CH2)6NH2)]4þ the pKa of the aqua ligands (pKa 5.62) is much lower
than in cis-[PtCl(H2O)(NH3)2]þ (pKa 6.41). For the trinuclear compound BBR3464 the aquation
rate constant is comparable to the dinuclear analog, but the chloride anation rate constant is
lower so that there is a significantly greater percentage of aquated species (30%) present at
equilibrium. The pKa of 5.62 for the aqua ligands is identical to the dinuclear case. Based on the
calculated equilibrium and dissociation constants, and assuming physiological pH (7.2), the
maximum tolerated dose (MTD) of BBR3464 in patients corresponds to 1.8 108 M and at
an intracellular chloride concentration of 22.7 mM the drug will be 98.7% in the dichloro form at
equilibrium. In blood plasma, at a [Cl] of 103 mM only 0.3% of the total is aquated.132
(iv) Reactions with oligonucleotides
Global DNA binding of polynuclear platinum compounds is characterized by very rapid binding,
a high level of DNA–DNA interstrand cross-links, unwinding of supercoiled plasmid DNA
typical of bifunctional DNA binding, and a sequence specificity different from that of cisplatin.133,134
Strong sequence preference for single dG or d(GG) sites was found and molecular modeling
suggested various possible adducts including 1,4-(G,G) and 1,6-(G,G) interstrand and 1,5-(G,G)
intrastrand cross-links, which were similar in energy (Figure 10).
822
Metal Complexes as Drugs and Chemotherapeutic Agents
1,4-Interstrand cross-link
1,5-Interstrand cross-link
1,6-Interstrand cross-link
Figure 10 (see color plate 11) Structures from molecular modeling of the major DNA adducts of BBR3464.
Due to the charged nature of polynuclear platinum complexes, ranging from 2þ to 4þ, it is not
surprising that binding to DNA occurs significantly more rapidly than for cisplatin. The binding
of polyamine-bridged dinuclear compounds is even faster than BBR3464, suggesting strong
preassociation or electrostatic binding prior to covalent attachment. Conformational changes
characteristic of the B ! A and B ! Z transitions have been observed in poly(dG)poly(dC)
and poly(dG-dC)poly(dG-dC) modified by all polynuclear platinum compounds.135–138 Ethidium
bromide binding favors the B-form of DNA, and intercalation into Z-DNA induced by NaCl or
[Co(NH3)6]3þ results in reversal to the B-form.139 In contrast, intercalation into A- and Z-form
DNA induced by dinuclear or trinuclear platinum compounds is inhibited indicating that the
conformational changes are essentially irreversible. The ability to maintain unusual DNA conformations in solution is a unique characteristic of polynuclear platinum compounds. Induced
A-like conformations in vivo are theorized to be control mechanisms for DNA binding proteins
like transcription factors.140 The biological function of Z-DNA is still not clearly defined;141 but
Z-DNA is known to form in the wake of RNA polymerase as DNA is transcribed.143 The
conformational ‘‘locking’’ into either A- or Z-form by polynuclear platinum compounds is likely
to have profound effects on DNA function. Antibodies raised to cisplatin-DNA adducts do not
recognize DNA adducts of dinuclear or trinuclear compounds.
An interesting and potentially important finding is that BBR3464 is preferentially bound to
single-stranded rather than double-stranded DNA.143 Comparison of single-stranded DNA,
RNA, and duplex DNA indicated that the reaction of BBR3464 with single-stranded DNA
and RNA was faster than with duplex DNA, and produced more drug–DNA and drug–RNA
adducts. BBR3464 binding to different nucleic acid conformations raises the possibility that the
adducts of single-stranded DNA and RNA may play a role in the different antitumor
efficacies as compared with cisplatin. Single-stranded DNA is present during transcription,
replication, recombination, and repair and is recognized by various single-stranded DNA
binding proteins.
The kinetics of the reaction of the self-complementary 12-mer duplex d(50 -A1T2ATGTA7CATAT-30 )2 with 15N labeled [{trans-PtCl(NH3)2}2-(H2N(CH2)6NH2)]4þ and BBR3464 indicated the
formation of 1,4-interstrand cross-links.144,145 Initial preassociation or electrostatic binding to
DNA is observed in both cases, as deduced by chemical shift changes in presence of DNA
immediately upon mixing. The time scale of the NMR experiment makes the weak preassociation
of cisplatin difficult to observe, although it may be observed with techniques such as quartz
crystal microbalance and mass spectrometry. The former system permits direct, real time detection of interactions between platinum complexes and surface immobilized oligonucleotides (in this
case 50 -GGGAAGGATGGCGCACGCTG-30 ).146 The closure rates to form bifunctional adducts
are significantly faster than the rate of closure to form a 1,2 GG intrastrand cross-link by cis[Pt(H2O)2(NH3)2]2þ. For the dinuclear compound, consideration of the 1H {Guanine H(8)} and
15
N shifts of the interstrand cross-link showed that an initially formed conformer converts into
another nonreversible final product conformer.
Metal Complexes as Drugs and Chemotherapeutic Agents
823
The 1,4-interstrand cross-link of BBR3464 with the self-complementary 50 -(ATGTACAT)2-30
has been characterized and analyzed by MS and CD, UV and NMR spectroscopy.147 The alternating
purine–pyrimidine sequence mimics the structural requirements for Z-DNA. NMR analysis of the
adduct shows the strong H8/H10 intraresidue cross-peaks for the platinated guanine residues,
consistent with a syn conformation of the nucleoside. More interestingly, a strong H8/H10
intraresidue cross-peak for the A7 resonance is also consistent with a syn conformation for this
base which is usually not observed for adenine residues and bases not directly involved in the
cross-link in oligonucleotides. Within the sequence covered by the cross-link, the bases appear to
be a mixture of syn and anti and Watson-Crick hydrogen bonding is maintained. The central
platinum unit resides in the minor groove. The observation of an altered conformation (Adenine
N7 syn) outside the binding site is unique and suggests the possibility of delocalized lesions beyond
the binding site. In contrast, long-range interstrand cross-linking agents such as CC-1065 and
Bizelesin do not show conformational changes beyond the environment of the binding sequence.148–150
These unusual cooperative effects are unique to this class of anticancer drug and are the first
demonstration of cooperative effects in solution for an anticancer drug.
(v) Site-specific intrastrand and interstrand cross-links of BBR3464. Bending, protein
recognition and nucleotide excision repair
Oligonucleotide duplexes containing various site-specific intra- and interstrand cross-links formed
by both dinuclear [{trans-PtCl(NH3)2}2m-(H2N(CH2)nNH2)]2þ and trinuclear compounds have
been prepared. The 1,2-intrastrand cross-link with one Pt unit each attached to two adjacent
guanines is formally the structural analog of the most prominent adduct formed by cisplatin.
The dinuclear intrastrand adducts distorted the DNA conformation in a way different from those seen
for adducts of cisplatin151–153 Bending induced in DNA by dinuclear interstrand cross-links is not
directed, and at approximately 10–12 is much less than that of cisplatin, as was duplex unwinding
(9 vs. 13 , respectively). As a result, gel retardation assays revealed only very weak recognition
of DNA adducts by HMG1 protein.154 For BBR3464 intrastrand site-specific adducts were
also prepared which create a local conformational distortion but without a stable curvature.155
Again, no recognition by HMG1domA and HMG1domB proteins was evident and it is clear that
the intrastrand DNA adducts of BBR3464 may present a block to DNA or RNA polymerases but
are not a substrate for recognition by HMG-domain proteins.
In general, DNA interstrand cross-links could be even more effective lesions than intrastrand adducts
in terminating DNA or RNA synthesis in tumor cells and thus could be even more likely candidates for
the genotoxic lesion relevant to antitumor effects of BBR3464.156 In addition, the interstrand cross-links
pose a special challenge to repair enzymes because they involve both strands of DNA and cannot be
repaired using the information in the complementary strand for resynthesis.157 Unlike the intrastrand
adduct, the interstrand cross-link is a poor substrate for nucleotide excision repair. These results validate
the finding that overexpressing the human nucleotide excision repair complex (ERCC1) was not
detrimental to the cellular sensitivity of BBR3464 in two ovarian cancer cell lines.158
These findings in sum suggest that these structurally distinct compounds produce a profile of
DNA damage that is quite distinct from that of cisplatin. Lack of recognition by proteins which
bind avidly to cisplatin-damaged DNA suggest that the mediation of antitumor properties of
polynuclear platinum compounds by cisplatin-like processes is unlikely. Thus, the structural
paradigm for antitumor activity based on the cisplatin structure is no longer valid—clinically
useful compounds may arise from study of new structures. Following this work, new dinuclear
compounds based on heterocycle azole and 4,40 -dipyrazolylmethane bridges have also been
described ((18)–(20), Figure 11).159–161 These agents again give a different spectrum of activity
to the dinuclear complexes with flexible diamine linkers.
9.18.2.2.4
Transplatinum compounds
The earliest ‘‘structure–activity’’ relationships indicated that the transplatinum geometry is inactive—
significantly higher doses must be given before any therapeutic effect is seen. In 1991, it was reported
that alteration of amine structure and the introduction of sterically hindered amines produced
cytotoxicity similar to that of cisplatin.162 The first examples used planar amines and a variety of
trans-[PtCl2(L)(L0 )] compounds have been synthesized and evaluated ((21)–(26), Figure 12).163
824
Metal Complexes as Drugs and Chemotherapeutic Agents
Cl
H3N
NH3
2+
Pt
Pt
H3N
Cl
N
N
NH3
NH
HN
(18 )
2+
N N
H3N
H3N
NH3
Pt
Pt
O
H
(19)
NH3
N
NH3
H3 N
N N
Pt
Pt
H3N
NH3
O
H
2+
(20)
Figure 11 Dinuclear platinum compounds based on heterocycle bridges.
In general, the cytotoxicity of these compounds was equivalent to cisplatin, and they maintained their activity in cisplatin-resistant cells. In many cases the activity of a trans complex was
actually comparable to that of the cis isomer.164 Later these general observations were confirmed
for a range of complexes in the trans geometry; examples of carrier ligands now include cha,
iminoethers, piperazine, and piperidine, as well as sterically hindered primary amines such as
isopropylamine.165–169 While their in vitro cytotoxicity is clearly comparable with cisplatin, no
exceptionally active compounds in vivo have been prepared. This fact may reflect some pharmacokinetic problems still associated with the trans geometry. While most emphasis on the differences between cis- and trans-platin has centered on the structures of their DNA adducts, the
different chemistry of the complexes themselves may also be important. This point is emphasized
by the enhanced antitumor activity of the PtIV compound (27) over its cytotoxic but antitumor
inactive PtII analog, trans-[PtCl2(NH3)(cha)].170 Solubility is still a major issue in the trans
complexes; the use of N,O-chelates in complexes such as [PtCl(NH3)(N,O-pyridine-2-acetate)]
(compound (28), in which the two N atoms are mutually trans) may solve this problem.171
Nevertheless, formally one may consider that trans-platinum complexes do indeed show in vivo
antitumor activity.
In the case of complexes such as (21) and (23) which have an extended planar ligand, a
significantly higher proportion of interstrand cross-links in DNA is formed in comparison to
either cis- or trans-platin.172 The steric effects of these planar ligands result in the formation of
structurally unique 1,2-interstrand cross-links like those formed by cisplatin, a unique example of
how steric effects may alter a nonactive lesion into an active one (Figure 13).173,174 Model studies
predicted this outcome by preparation of the monofunctional models trans-[PtCl(9-ethylguanine)
(NH3)(quinoline)] and comparison of substitution rates of the Pt—Cl bond by G or C mononucleotides.175,176 Interestingly, the iminoether compound (25) appears to form predominantly
monofunctional adducts with DNA.177
The DNA binding of trans-platinum complexes is thus quite rich and varied. The cellular
effects of such adduct formation also appear to be significantly different from those of cisplatin.
825
Metal Complexes as Drugs and Chemotherapeutic Agents
H3N
Cl
Cl
Pt
Cl
Cl
N
N
N
N
Cl
(22)
( 21)
( 23)
Me
Cl
NH2
Pt
NH Cl
H
OMe
OMe
N
Pt
N
Cl
N
Pt
NH Cl
H
Cl
(26)
O
OH
NH3
Pt
N
Cl
H2 OH
O
N
Pt
H3N
Cl
( 28)
( 27)
Figure 12
Cl–
H2N
+
Me
(25)
(24)
Cl
Cl
Pt
S
Cl
NH3
Pt
Trans-platinum compounds as potential anticancer compounds.
1,1-Interstrand cross-link
L = NH3
(trans-platin)
1,2-Interstrand cross-link
L = L'py, tz or
L = NH3 or dmso
and l' = quin, tz
1,2-Interstrand cross-link
L = NH3
(cis-platin)
Figure 13 Interstrand cross-links formed by sterically hindered trans-platinum compounds.
Optimization of the pharmacokinetic profile of trans-platinum compounds may eventually produce a clinically effective agent.
9.18.3
9.18.3.1
NONPLATINUM ANTICANCER AGENTS
Ruthenium Complexes
In the early development of analogs of the platinum compounds, complexes with ‘‘windows of
reactivity’’ similar to the platinum complexes were examined extensively. Whereas direct Ni and
Pd analogs of Pt complexes are too kinetically reactive to be of use as drugs, Ir and Os ammine
826
Metal Complexes as Drugs and Chemotherapeutic Agents
compounds are in general too inert. Ruthenium and rhodium have produced compounds with the
greatest promise, although no direct analogs have yet advanced to the clinic. In ruthenium
ammine complexes of the general series [RuCln(NH3)6n]zþ (where n ¼ 3, 4, or 5), fac[RuCl3(NH3)3]
showed good activity but was not sufficiently water soluble for extensive testing.178,179 Ruthenium-ammine compounds have a rich DNA chemistry which has been described by Clarke.
The guanine N7 site is the preferred binding site for the aqua species [Ru(H2O)(NH3)5]2þ, but metal
migration may occur to other nucleobases.180 GSH modulates DNA binding of Ru-ammine
complexes: GSH reduction of the RuIII compound [ClRu(NH3)5]2þ to the RuII state enhances its
DNA binding, but at [GSH]/[Ru] ratios >1 DNA binding is inhibited through eventual formation
of [(GS)(NH3)5RuIII]. Covalent binding of trans-[(H2O)(py)Ru(NH3)4]2þ to DNA occurs specifically at guanine N7.181 The pyridine ligand further stabilizes the RuII oxidation state, which may
lead to disproportionation of the generated RuIII species to RuII and RuIV species.182 Oxidative
damage to DNA through base-catalyzed air oxidation of guanine occurs in the presence of
{RuIII(NH3)5}-bound DNA. These and other aspects have been reviewed thoroughly.
A wide variety of Ru-based complexes, including carboxylate-bridged di- and trinuclear complexes, exhibit antitumor activity in animal models. The imidazole complexes trans-[RuCl4(L)2]
(where L ¼ imidazole, indazole) have good antitumor activity.183,184 Transferrin and serum albumin
may act as transporters of the metal complexes in blood, and DNA is considered the ultimate
target.185 Modification of the structural motif of the DMSO complexes cis/trans-[RuCl2(DMSO)4]
with imidazole ligands has led to an interesting clinical candidate, NAMI-A ((29), Figure 14).186 The
mechanism of action of this compound is not related to DNA binding; rather, it is an antimetastatic
agent.187 Metastasis (the process whereby tumor growth occurs distant from the original or primary
tumor site) is intimately linked with angiogenesis, the dynamic process that involves new blood
vessel formation. Inhibition of angiogenesis is an attractive approach to antitumor (antimetastatic)
therapy.188 NAMI-A is active against lung metastasis in vivo and tumor cell invasion in vitro.189–191
The molecular details by which NAMI-A exerts antimetastatic effects in vivo have not been
definitely determined, and may occur by multiple mechanisms. The solution chemistry of NAMI-A
involves both loss of Cl and DMSO. Interestingly, the antimetastatic activity is retained under a
wide variety of experimental conditions producing solvolyzed intermediates.192 The exact nature
of the active species may be difficult to resolve.
A noteworthy addition to Ru-DNA chemistry is the inhibition of topoisomerase II by the areneRu complex [RuCl2(DMSO)(6-C6H6)].193 Further variations on the arene theme produce cytotoxic
compounds of formula [(arene)Ru(en)Cl]þ.194,195 The crystal structure of the 9-ethylguanine adduct
[(arene)Ru(en)(9-EtG)]2þ shows interesting stacking between the arene and guanine rings.
9.18.3.2
Arsenic Trioxide
Platinum complexes are cytotoxic agents yet the paradigm in cancer chemotherapy has moved to
a more targeted approach, with special emphasis on signaling pathways. In this respect a
remarkable story is that of arsenic trioxide, As2O3 (Trisenox, Cell Therapeutics Inc, Seattle,
USA) which was approved by the FDA in September 2000 for treatment of acute promomyelocytic leukemia (APL) in patients who have relapsed or are refractory to retinoid and anthracycline
chemotherapy. An estimated 1,500 new cases of APL are diagnosed yearly in the US, of which an
–
NH
NH
N
Cl
Cl
Ru
Cl
O
Cl
S
N+
H
CH3
CH3
(29)
Figure 14 Structure of a potential ruthenium-based antimetastatic agent, NAMI-A.
Metal Complexes as Drugs and Chemotherapeutic Agents
827
estimated 400 patients will not respond to, or will relapse from, first-line therapy. The approval of
arsenic trioxide as a chemotherapeutic agent invokes the pioneering work of Ehrlich and the
development of Salvarsan for use in syphilis—the foundation stone for the science of chemotherapy.
The use of chelating agents in medicine may even be traced to a collaboration between Werner (the
father of coordination chemistry) and Ehrlich (the father of chemotherapy) to find less toxic arsenic
compounds for the treatment of syphilis.15 Arsenic has been used therapeutically for more than 2,000
years and was used in the 1930s for treatment of chronic myelogenous leukemia until supplanted by
newer chemotherapies.196,197 The past, present, and future of medicinal arsenic has been described
as a story of ‘‘use, dishonor, and redemption’’. Recent interest in arsenic trioxide initially arose
through Chinese reports of its efficacy and use.198 The recommended dose is 0.15 mg kg1 d1
until remission.199 Side effects are cardiotoxicity, skin rashes, and hyperglycemia.200
Arsenic trioxide apparently affects numerous intracellular signal transduction pathways and
causes many alterations in cellular function. Thus, the mechanisms of cell death induced by
arsenic trioxide are multiple: induction of apoptosis, inhibition of proliferation, and even inhibition of angiogenesis have all been reported.201 In cellular studies, arsenic trioxide inhibits
glutathione peroxidase, possibly through generation of arsenic–GSH conjugates, and increases
cellular hydrogen peroxide content.202 Consistent with a general role in redox processes, ascorbic
acid enhances arsenic trioxide-induced apoptosis of lymphoma cells but not of normal bone
marrow cells, by increasing cellular H2O2 content.203 Arsenic trioxide sensitivity is associated
with low levels of GSH in cancer cells.204 Apoptosis is apparent when cells are treated with low
concentrations of the drug; this effect is associated with the collapse of mitochondrial transmembrane potentials in a thiol-dependent manner.205 The combined effects have led to the suggestion
that arsenic trioxide may be situated as a novel mitochondriotoxic anticancer agent.206 Membrane
potential decreases and membrane permeability increases as a result of arsenic treatment, resulting in the release of messenger molecules for the degradation phase of apoptosis.
9.18.3.3
The Mitochondrion as Target. Gold–phosphane Complexes
Apoptosis is important in tissue homeostasis; inhibition of apoptosis may contribute to transformation of cells and/or chemotherapy resistance. The apoptosis factors leading to cell death are
mitochondrion-regulated. Mitochondria contribute to the regulation of energy production, metabolism, and redox status as well as apoptosis.207 The integral role of the mitochondrion in
programmed cell death is by now well recognized and means that the mitochondrion is a suitable
target for drug intervention.208 Mitochondrial DNA is also an attractive target because it is
significantly more sensitive to covalent damage than nuclear DNA, because of the lack of
protective histones and a limited capacity for repair. The pioneering work of Chen showed that
enhanced mitochondrial membrane potential is a prevalent cancer cell phenotype;209 lipophilic
cations accumulate inside mitochondria as a consequence of the higher membrane potentials.207
Treatment strategies directed at novel cellular targets but which are differentiated between normal
and tumor cells are attractive approaches to selective tumor cell killing.
The gold–phosphane complexes (30)–(33) (Figure 15) are examples of lipophilic cations which
may also have a role in mitochondrial toxicity.210,211 Whereas the role of gold salts in antiarthritis
therapy is intimately related to thiol binding, the tetrahedral diphosphane compounds are much
less reactive toward thiols.212,213 The lipophilic cation [Au(dppe)2]þ (where dppe ¼ 2-bis(diphenylphosphino)ethane) showed potent in vitro cytotoxicity with evidence of antimitochondrial
function214 but hepatotoxicity attributed to alterations in mitochondrial function curtailed clinical
trials. The solution chemistry of gold–diphosphane compounds is rich and the interchange
between mononuclear and dinuclear phosphane-bridged species has been extensively examined.57
Substitution of the phenyl groups by 2-pyridyl groups provides an opportunity to investigate
systematically the relationship of drug activity to lipophilicity.215,216 Compounds that are highly
active in vitro may be obtained. Alteration of the lipophilicity greatly affected cellular uptake and
binding to plasma proteins. Alterations in lipophilicity also affect host toxicity, allowing the
opportunity for optimization of pharmacokinetic properties.
9.18.3.4
Manganese-based Superoxide Dismutase Mimics
A significant amount of the O2 metabolized by the human organism is converted to the highly
reactive superoxide radical anion O2. Endogenous overproduction of O2 may cause considerable
828
Metal Complexes as Drugs and Chemotherapeutic Agents
+
R2P
PR'2
Au
Au
X
X
R 2P
PR'2
2+
R2P
Au
R 2P
Au
PR'2
R2 R2
P
P
Au
P
P
R2 R 2
Au
R2P
PR'2
(32)
( 31)
( 30)
PR'2
R2
P
Au
P
R2
2+
R2
P
P
R2
(33)
Figure 15 Structures of Au–phosphane compounds as potential mitochondrial poisons.
damage to biological systems. Superoxide has been shown to be a mediator of reperfusion
diseases, such as those occurring after a stroke, and has been shown to be associated with
development of inflammatory processes and also in the initiation of neurological disorders such
as Parkinson’s disease.217 The enzyme superoxide dismutase (SOD), either as the manganesecontaining MnSOD (present in the mitochondrion) or the dinuclear Cu/Zn-SOD (present in the
cytosol and extracellular space), performs the role of superoxide detoxification in normal cells and
tissue:218
O2 þ Mnþ þ 2Hþ ! H2 O2 þ Mðnþ1Þþ
O2
ðnþ1Þþ
ð1Þ
nþ
ð2Þ
2O2 þ 2Hþ ! H2 O2 þ O2
ð3Þ
þM
! O2 þ M
Overall:
Attempts to use the enzyme itself as a therapeutic agent have been partially successful in
animals, but not in humans.219 Pharmacokinetic problems, including delivery problems and
the short half-life in the blood, are major obstacles to use of the enzyme in humans. Cu/ZnSOD preparations (trade names Palosein, Orotein) are used to treat inflammatory diseases in
dogs and horses. Small molecule mimics of natural enzymes such as SOD (dubbed synzymes
for synthetic enzymes) may effect similar chemistry and thus be useful in treating disease
states brought on by an imbalance in superoxide. The considerations for successful application of this strategy are many: a compound must possess high chemical stability, SOD-like
activity, specificity under biological conditions, low toxicity, and favorable biodistribution.
Manganese chelate compounds such as (34) and (35), especially those based on cyclam
(1,4,8,11-tetraazacyclotetradecane) and N,N0 -bis(salicylaldehydo) ethylenediamine (salen), have
shown considerable promise in this regard (Figure 16).220–222 Rational design has produced an
optimal structure M40403 (35) which is a leading clinical candidate.223,224 This pyridine-based
macrocycle has been used as a cancer co-therapy with interleukin-2 (IL-2), an immune-stimulating
cytokine drug that is approved for use in metastatic melanoma and renal cell carcinoma. As
usual, the utility of IL-2 is limited by side effects, notably hypotension, and hospitalization is
necessary for many patients. Preclinical studies have shown that M40403 enhances the efficacy of
IL-2. A phase I, double-blind, placebo-controlled clinical trial of M40403 administered intravenously to 36 normal, healthy human subjects showed no dose-limiting side effects. A phase II
clinical trial is planned to assess the effectiveness of M40403 as co-therapy with IL-2 in patients
with advanced skin and end-stage kidney cancers (http://www.metaphore.com). Interestingly,
829
Metal Complexes as Drugs and Chemotherapeutic Agents
Cl
N
N
N
NH
Mn
O
A
Mn
HN
O
HN
NH
Cl
(35)
(34)
Figure 16
Manganese compounds as SOD mimics.
there is some indication that the salen-based compounds may involve catalase rather than SOD
activity (Equation 4):
H2 O2 þ 2Hþ ! 2H2 O
9.18.3.5
ð4Þ
Titanium Compounds
Two titanium compounds have had clinical trials in Germany. The titanocene compound
[TiCl2Cp2] ((36); known as MTK4) and budotitane (37), a -diketonate derivative, are structurally quite different compounds (Figure 17). Little information is available on the mode of action
of budotitane which is formulated in a mixture of glycols and water because of a lack of aqueous
solubility.225 Budotitane exists as a mixture of three cis isomers (37a–c) in thermal equilibrium, so
that no isomerically pure species have been isolated.226 Hydrolysis of the ethoxy groups is rapid—
the formulation slows this down and prevents formation of oligomeric oxo-bridged complexes.
The MTD of budotitane was 230 mg m2 and the dose-limiting toxicity was cardiac arrhythmia.227 The poorly defined aqueous properties and lack of details on the mechanism of action do
not bode well for this drug.
The phase I clinical trial of [TiCl2Cp2] indicated a MTD of 315 mg m2 for a single intravenous
infusion, and 185 mg m2 weekly.228 The dose-limiting toxicity was nephrotoxicity.229 A phase II
trial in renal cell cancer concluded that no advantage was gained by use of [TiCl2Cp2].230
Modifications on the basic [TiCl2Cp2] structure have included metal modification, Cp and
leaving group (Cl) substitution, as well as use of ionic metallocenes for improving aqueous
solubility.231
R1
R2
Cl
Ti
Cl
R4
O
O
Ti
O
OEt
OEt
O
R3
(36)
(37)
a: R1 = R3 = Me; R2 = R4 = Ph
b: R1 = R3 = Ph; R2 = R4 = Me
c: R1 = R4 = Me; R2 = R3 = Ph
Figure 17
Titanium anticancer agents that have undergone clinical trials.
830
Metal Complexes as Drugs and Chemotherapeutic Agents
DNA is purportedly the target of [TiCl2Cp2]. The somewhat naı̈ve early assertion that it could
act in a manner similar to cisplatin because of the similarity in ClCl distances has never been
upheld experimentally.232,233 Instead the aqueous chemistry of [TiCl2Cp2] is dominated by loss of
the Cp ring as well as hydrolysis of the Ti—Cl bonds. DNA interactions at pH 7 are very weak
and the adducts when formed do not suppress DNA-processing enzymes so there is doubt as to
whether DNA is the locus of action for these drugs. Ti–DNA interactions are dominated by
interaction with the phosphodiester backbone. Other biological effects observed for [TiCl2Cp2]
include inhibition of protein kinase C and DNA topoisomerase II activity, as well as inhibition of
collagenase type IV activity, suggesting some antimetastatic behavior. Titanium may also replace
iron in transferrin, allowing a possible uptake mechanism into tumor cells.234
9.18.3.6
Gallium Nitrate
The principal, approved use of Ga(NO3)3 (Ganite, gallium nitrate) is in treating hypercalcemia of
malignancy, by reducing the elevated Ca2þ in blood.235 This disorder is often associated with
bone cancers and is an acute-care condition in which rapid bone loss leads to life-threatening
levels of blood calcium. Gallium reduces the rate of bone loss by inhibition of the action of
osteoclasts, which produce acid onto the bone surface dissolving mineral and protein components.
Inhibition of this ‘‘proton’’ pump is thus a well-defined mechanism of action for gallium.
Relatively low levels (200 mg m2 day1) are effective. At therapeutic doses, it has few side effects
and is well tolerated. Most recent attention has focused on the activity of gallium nitrate against
malignancies, especially non-Hodgkin’s lymphoma, non-squamous cell carcinoma of the cervix,
and bladder cancer. Clinical trials under the auspices of Genta (http://www.genta.com) will
evaluate its efficacy on patients with low- or intermediate-grade non-Hodgkin’s lymphoma who
have failed prior chemotherapy. The results of phase II trials in non-small-cell lung cancer and
prostate cancer have also been reported.236,237
Gallium compounds may be designed to deliver the Ga3þ cation more effectively or selectively.
Combination with bisphosphonates has been suggested to improve oral availability of gallium.
Chelating agents such as 8-hydroxyquinoline,238 thiosemicarbazones239 and pyridoxal isonicotinoyl
hydrazone (Ga-PIH)240 give well-defined GaIII complexes.
9.18.4
9.18.4.1
ANTIBACTERIAL AGENTS
Silver and Mercury Salts
Silver and mercury salts have a long history of use as antibacterial agents.241–243 The use of
mercurochrome ((40), Figure 18) as a topical disinfectant is now discouraged. Silver sulfadiazene
(38) finds use for treatment of severe burns; the polymeric material slowly releases the antibacterial Agþ ion. Silver nitrate is still used in many countries to prevent ophthalmic disease in newborn
children.244 The mechanism of action of Ag and Hg is through slow release of the active metal
ion—inhibition of thiol function in bacterial cell walls gives a rationale for the specificity of
bacteriocidal action.
COONa
Ag+
N
N
O
N S
–
O
(38)
COONa
Br
Br
NH2
SHgEt
(39)
O
NaO
HgOH (40)
Figure 18 Silver- and mercury-based antibacterial agents.
O
831
Metal Complexes as Drugs and Chemotherapeutic Agents
9.18.4.2
Bismuth-containing Antiulcer Drugs
Bismuth compounds have been used for their antacid and astringent properties in a variety of
gastrointestinal disorders.245,246 The effectiveness of bismuth is due to its bacteriocidal action
against the Gram-negative bacterium, Helicobacter pylori. Usually the bismuth preparations are
obtained by mixing an inorganic salt with a sugar-like carrier (see Figure 19). Commonly used
agents are colloidal bismuth subcitrate (CBS), and bismuth subsalicylate (BSS). The mechanism
of action is complex and includes inhibition of protein and cell wall synthesis, membrane
function, and ATP synthesis. The most notable salts are tripotassiumdicitratobismuth, bismuth
salicylate, Pepto-Bismol (BSS), and De-Nol (CBS; (41)). The ‘‘sub’’ designation most likely arose
from stoichiometry of oxygen to bismuth. The combination of ranitidine (a histamine H2-receptor
antagonist) and bismuth citrate is marketed as Ranitidine Bismutrex for the management of
peptic ulcer and ulcers associated with H. pylori.247
Much progress has been made on the coordination chemistry of these preparations. Detailed
molecular characterization is obviously of primary importance in understanding chemical and
biochemical function. BiIII is highly acidic in aqueous medium and the oxygen-rich nature of the
sugar carrier ligands leads to formation of di- and polynuclear-bridged complexes, based on the
typical dinuclear unit (41) shown in Figure 19.248–251 The nature of the ranitidine/bismuth citrate
adduct has been examined and second coordination sphere effects were noted for the organic
amine.252 Methylthiosalicylate has also been used instead of salicylate, and discrete complexes
(e.g., (42)) have been comprehensively characterized.253,254 Bismuth (III) remarkably forms stable
complexes with GSH255 and transferrin.256 The latter observation may be correlated with the high
acidity of the BiIII ion.
9.18.4.3
Metal-containing Drugs as Antiparasitic Agents
There remains an urgent need for new effective antiparasitic agents, an area of drug development
that has languished because of poor economic return. The spread of resistance to chloroquine (an
antimalaria treatment) is one reason for attention to be paid to this area, as well as the sheer
numbers of people affected. Antimony compounds (43) and (44) (Figure 20) are used to treat
O
OH
O
O
OH
HO
OH
OH
H4gal
H2sal
O
O
O
O
Bi
O
O
O
OH
OH
O
H4cit
H4tar
O
O
O
O O Bi
S
MeO
O
Bi
S
O
OMe
O
S
O
O
( 41) (basic skeleton only
shown for clarity)
Figure 19
O
OH
HO
O
OH
HO
HO
OH
O
OH
MeO
(42)
Bismuth antiulcer drugs—the sugars used to produce the usually polymeric structures are shown
in the top panel.
832
Metal Complexes as Drugs and Chemotherapeutic Agents
O
O
H
C
H
C
O
O
O
O
Sb
O
O
O
2–
O
Sb
C
H
O
C
H
(43)
O
5–
SO3–
SO3–
O
O
Sb
–
O3S
O
O
SO3–
(44 )
Figure 20 Antimony-based antiparasitic agents.
leishmaniasis (H. Sun, personal communication). Another approach is to complex metal ions to
known antiparasitic agents in attempts to gain selective uptake or selective action of the metal–
drug conjugate. Gold and ruthenium complexes of chloroquine and clotrimazole have been
described ((45) and (46), Figure 21).257–260 In favorable cases, some of these compounds show
good activity—the chloroquine complexes being useful even in chloroquine-resistant cases.
9.18.5
9.18.5.1
PHARMACODYNAMIC USES OF METAL COMPLEX DRUGS
Lithium Carbonate
The clinical value of lithium has been recognized since 1949. Lithium carbonate is used in manic
depressive psychoses for the treatment of recurrent mood changes.261,262 Mood stability may only
occur after months rather than weeks. The drug is administered orally in doses up to 2 g day1
(30 mmol day1). The serum Li concentration should be in the range of 0.4–0.8 mmol l1.
+
N(CH2CH3)2
HN
Et2N
Cl
Cl
Ru
N
Cl
NH
Cl
Cl
N
N
Ru
Au
PPh3
HN
(45)
Cl
Cl
NEt2
(46)
Figure 21 Gold and ruthenium complexes of antiparasitic agents.
833
Metal Complexes as Drugs and Chemotherapeutic Agents
The development of lithium-specific electrodes has assisted greatly in monitoring patient compliance. The toxicity profile of lithium carbonate is now well established and the drug is safely
administered and well tolerated. It is of limited use in other psychiatric disorders such as
pathological aggression, although additional benefit may also include a reduction in actual or
attempted suicide.
Newer uses have appeared in the treatment of viral diseases including AIDS, alteration of the
immune response, and cancer. The lithium salt of -linolenic acid (LiGLA) has a significant
anticancer effect against certain cancers. The neurochemical basis for lithium action is difficult to
define. Lithium carbonate induces a wide range of intra- and extracellular changes—most
emphasis has been naturally on the similarities with Na/K/Ca/Mg ions. Lithium selectively
interferes with the inositol lipid cycle, representing a unified hypothesis of action. The biochemistry, distribution, and cellular localization of lithium has been extensively documented.
9.18.5.2
Vanadium Complexes in Diabetes
The role of vanadium in biological systems in general is of increasing interest.263 The discovery of
the insulin-like properties of vanadate ions spurred research into the clinical use of vanadium
compounds as insulin mimics.264 Inadequate glucose metabolism, either through absence of
endogenously secreted insulin or insulin resistance, leads to diabetes mellitus. The potential of
insulin-mimetic compounds as drugs lies in their oral administration—insulin, as a small protein,
is not orally active. The vanadate (V) ion is effective upon oral administration, and an obvious
strategy to enhance the pharmacokinetic characteristics and the efficacy of the insulin-mimetic
response is complexation of vanadate with suitable biologically compatible ligands.265,266
Insulin binding to the extracellular side of cell membranes initiates the ‘‘insulin cascade’’, a
series of phosphorylation/dephosphorylation steps. A postulated mechanism for vanadium is
substitution of vanadate for phosphate in the transition state structure of protein tyrosine
phosphatases (PTP).267,268 In normal physiological conditions, the attainable oxidation states of
vanadium are VIII, VIV and VV. Relevant species in solution are vanadate, (a mixture of HVO42/
H2VO4) and vanadyl VO2þ. Vanadyl is not a strong inhibitor of PTPs, suggesting other
potential mechanisms for insulin mimesis for this cation.
Both VIV and VV coordination compounds have been tested as insulin mimics. The preponderance of VIV compounds contain the V¼O(L-L)2 motif (e.g., (47) and (48), Figure 22) and
complexes containing a variety of O,O; N,O; N,S; and S,S bidentate ligands L–L have been
synthesized and tested. Control of lability and ligand displacement are important criteria for drug
design in terms of delivery of the biologically active vanadate. Clinical trials have focused to date
on sodium orthovanadate and the bis(maltolato)oxovanadium(IV) compound (BMOV) (47). The
speciation and aqueous chemistry of BMOV have been described.266
9.18.5.3
Gold Compounds as Antiarthritic Agents
Gold salts have had a long history of use in rheumatoid arthritis.269,270 The development of orally
active auranofin (also known as Ridaura; (50), Figure 23) was a major improvement over the
early ‘‘injectable gold’’ preparations which were polymeric (e.g., (51)–(53)). However, use has
declined with the popularity of nonsteroidal antiinflammatory drugs (NSAIDS) such as indomethacin; a recent estimate of the commercial value for auranofin was $6 million. The mechanism
CH3
O
O
O
V
O
O
O
O
O
CH3
(47)
C8H17
N
H
H2 O H 2
N
N
V
S
S
(48 )
Figure 22 Vanadium compounds in treatment of diabetes.
O
N
H
C8H17
834
Metal Complexes as Drugs and Chemotherapeutic Agents
SO3
S
CH2OAc
O
3–
S
Au(PEt3)
OAc
Au S
AcO
O3S
( 50)
(49)
OAc
Polymeric [AuRS]n compounds:
(52) RS– =
( 51) RS– = CO2–
CH S–
–
( 53) RS– =
O
S–
O3S
CH2
CH2OH
S–
OH
HO
CO2–
OH
Figure 23
Au antiarthritis compounds.
of action is postulated to occur through thiolate exchange reactions.271 The structures of the
polymeric gold compounds have been described in detail. An interesting feature of gold metabolism is the production of [Au(CN)2]269 as a metabolite of the gold-thiol compounds.
9.18.5.4
Nitric Oxide in Physiology and Medicine
An intriguing aspect of the role of metal complexes in medicine is the role of NO.272,273 The
nitroprusside ion, [Fe(NO)(CN)5]2 is a vasodilator used in emergency situations to treat hypertensive patients in operating theaters.274,275 The complex is 30–100 times more potent than simple
nitrites. The mechanism is considered to be release of NO, an understanding prompted by the
emergence of NO as a prominent cell signaling molecule.273 Related to the biology of NO is
production of peroxynitrite ONOO through reaction of NO with O2. In this regard, production
of peroxynitrite may play a role in many pathological conditions.276,277 Water-soluble porphyrins
and texaphyrins may catalytically react with ONOO and may have clinical utility in peroxynitrite
scavenging.
9.18.5.5
Lanthanum Carbonate
Patients with end-stage renal disease hyperphosphatemia ineffectively filter excess phosphate that
enters the body in the normal diet.278 Elevated phosphate produces the bone disorder renal
osteodystrophy. Skeletal deformity may occur, possibly associated with cardiovascular disease.
Calcium deposits may further build up around the body and in blood vessels creating further
health risks. The use of lanthanum carbonate is being promoted as an alternative to aluminumbased therapies.279,280 Systemic absorption, and cost have produced a clinical candidate, Fosrenol
(AnorMED), an intriguing use of a lanthanide compound in therapy.
9.18.6
REFERENCES
1. Farrell, N. P. Transition Metal Complexes as Drugs and Chemotherapeutic Agents; James, B. R.; Ugo, R., Ed.; ReidelKluwer Academic Press: Dordrecht, 1989; Vol. 11.
2. Farrell, N. P. The Uses of Inorganic Chemistry in Medicine; The Royal Society of Chemistry: Cambridge, 1999.
3. Orvig, C.; Abrams, M. J. Chem. Rev. 1999, 99, 2201–2204.
4. Guo, Z.; Sadler, P. J. Angew Chem., Int. Ed. Engl. 1999, 38, 1512–1531.
Metal Complexes as Drugs and Chemotherapeutic Agents
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
835
Keppler, B. Metal Complexes in Cancer Chemotherapy; VCH: Basel, 1993.
Clarke, M. J. Progress in Clinical Biochemistry and Medicine, 1989; Vol. 10.
Fricker, S. P., Ed.; Metal Complexes in Cancer Therapy. Chapman and Hall: London, 1994; Vol. 1, p 215.
Berthon, G. Handbook of Metal–ligand Interactions in Biological Fluids; Marcel-Dekker Inc.: New York, 1995; Vol. 1
and 2.
Clarke, M. J.; Sadler, P. J., Eds.; Metallopharmaceuticals I: DNA Interactions; Springer-Verlag: Berlin 1999; Vol. 1,
p 199.
Sadler, P. J. Adv. Inorg. Chem. 1999, 49, 183–306.
Roat, R. M. Bioinorganic Chemistry: A Short Course, Wiley Interscience, Hoboken, New Jersey, 2002.
Sigel, H.; Sigel, A., Eds., Metal Ions in Biological Systems; Marcel Dekker: New York 1995; Vol. 31.
Lever, A. B. P. Ed., Coord. Chem. Rev. 2003, Vol. 232 Aspects of Biomedical Inorganic Chemistry. Elsevier Press.
Reynolds, J. E. F. Ed., Martindale The Extra Pharmacopoeia, 31sted.; The Royal Pharmaceutical Society; London,
1996. Martindales Pharmacopeia.
Andersen, O. Chem. Rev. 1999, 99, 2683–2710.
Liu, Z. D.; Hider, R.C. Coord. Chem. Rev. 2002, 232, 151–172.
Sarkar, B. Chem. Rev. 1999, 99, 2535–2544.
Whittaker, M.; Floyd, C. D.; Brown, P.; Gearing, A. J. Chem. Rev. 1999, 99, 2735–2776.
Parks, W. C.; Mecham, R.; Mecham, R. P. Matrix Metalloproteinases; Academic Press, 1998.
Vallee, B. L.; Auld, D. S.; Acc. Chem. Res. 1993, 26, 543–551. Jolles, P.; Jornvall, H., Eds.; Verlag: Basel, 1995, p 259.
Rein, A.; Henderson, L. E.; Levin, J. G. Trends Biochem. Sci. 1998, 23, 297–301.
Albert, A. Selective Toxicity, 6th ed.; Wiley: New York, 1979.
Food and Drug Administration: http://www.fda.gov United States Food and Drug Administration; Vol. 2002.
National Cancer Institute: http://nci.nih.gov/dtp.cfm NCI-DTP; Vol. 2002.
Bertucci, C.; Domenici, E. Curr. Med. Chem. 2002, 9, 1463–1481.
He, X. M.; Carter, D. C. Nature 1992, 358, 209–215.
Chan, J.; Huang, Z.; Merrifield, M. E.; Salgado, M. T.; Stillman, M. J. Studies of metal binding reactions in
metallothioneins by spectroscopic, molecular biology, and molecular modeling techniques. Coord. Chem. Rev. 2002,
233, 319–339.
Sun, H.; Li, H.; Sadler, P. J. Chem. Rev. 1999, 99, 2817–2842.
Petering, D.; Xiao, J.; Nyayapati, S.; Fulmer, P.; Antholine, W. Oxidation Damage by Bleomycin, Adriamycin and
Other Cytotoxic Agents that Require Iron or Copper; Farrell, N., Ed.; The Royal Society of Chemistry: Cambridge,
1999, pp 135–157.
Claussen, C. A.; Long, E. C. Chem. Rev. 1999, 99, 2797–2816.
Weinstein, J. N.; Myers, T. G.; O’Connor, P. M.; Friend, S. H.; Fornace, A. J., Jr.; Kohn, K. W.; Fojo, T.; Bates, S. E.;
Rubinstein, L. V.; Anderson, N. L.; Buolamwini, J. K.; van Osdol, W. W.; Monks, A. P.; Scudiero, D. A.; Sausville, E. A.;
Zaharevitz, D. W.; Bunow, B.; Viswanadhan, V. N.; Johnson, G. S.; Wittes, R. E.; Paull, K. D. Science 1997, 275,
343–349.
Boyle, F. T.; Costello, G. F. Chem. Soc. Rev. 1998, 27, 251–261.
Rosenberg, B. Platinum Complexes for the Treatment of Cancer. Why the Search goes on. In Cisplatin: Chemistry and
Biochemistry of a Leading Anticancer Drug; Lippert, B., Ed.; Wiley-VCH: New York, 1999 pp 3–30.
Lippert, B., Ed. Cisplatin: Chemistry and Biochemistry of a Leading Anticancer Drug; Wiley-VCH: New York, 1999.
Kelland, L. R.; Farrell, N. P. Platinum-based Drugs in Cancer Therapy; Humana Press, Totawa, New Jersey. 2000.
Wong, E.; Giandomenico, C. M. Chem. Rev. 1999, 99, 2451–2466.
Weiss, R. B.; Christian, M. C. Drugs 1993, 46, 360–377.
Lebwohl, D.; Canetta, R. Eur. J. Cancer 1998, 34, 1522–1534.
O’Dwyer, P. J.; Johnson, S. W.; Hamilton, T. C. Cisplatin and Its Analogues. In Cancer Principles and Practice of
Oncology 5th ed.; DeVita, V. T., Hellman, S.; Rosenberg, S. A., Eds.; Lippincott-Raven: Philadelphia, 1997; Vol. 2,
pp 418–431.
O’Dwyer, P. J.; Stevenson, J. P.; Johnson, S. W. Clinical Status of Cisplatin, Carboplatin, and Other Platinum-based
Antitumor Drugs. In Cisplatin: Chemistry and Biochemistry of a Leading Anticancer Drug; Lippert, B., Ed.; WileyVCH: New York 1999, pp 31–72.
Highley, M. S.; Calvert, A. H. Clinical Experience with Cisplatin and Carboplatin; Kelland, L. R.; Farrell, N. P., Eds.;
Humana Press: Totowa NJ, 2000, pp 89–113.
Christian, M. C. Semin. Oncol. 1992, 19, 720.
Lokich, J.; Anderson, N. Ann. Oncol. 1998, 9, 13–21.
Burcheranal, J. H.; Kalaher, K.; Dew, K. Biochemie 1978, 60, 961.
Macdonald, J. S.; Astrow, A. B. Semin. Oncol. 2001, 28, 30–40.
Pelley, R. J. Curr. Oncol. Rep. 2001, 3, 147–155.
Ruley, H. E. Important Adv. Oncol. 1996, 10, 37–56.
Eastman, A. The Mechanism of Action of Cisplatin: From Adducts to Apoptosis. In Cisplatin: Chemistry and
Biochemistry of a Leading Anticancer Drug; Lippert, B., Ed.; Wiley-VCH: Weinheim, 1999, pp , 111–134.
Gonzalez, V. M.; Fuertes, M. A.; Alonso, C.; Perez, J. M. Mol. Pharmacol. 2001, 59, 657–663.
Kartalou, M.; Essigmann, J. M. Mutat. Res. 2001, 478, 23–43.
Perez, R. P. Eur. J. Cancer 1998, 34, 1535–1542.
Kartalou, M.; Essigmann, J. M. Mutat. Res. 2001, 478, 1–21.
Harrap, K. R.; Jones, M.; Siracky, J.; Pollard, L. A.; Kelland, L. R. Ann. Oncol. 1990, 1, 65–76.
Loh, S. Y.; Mistry, P.; Kelland, L. R.; Abel, G.; Harrap, K. R. Br. J. Cancer 1992, 66, 1109–1115.
Berners-Price, S. J.; Appleton, T. G. The Chemistry of Cisplatin in Aqueous Solution; In Platinum-Based
Drugs in Cancer Therapy. Kelland, L. R.; Farrell, N., Eds.; Humana Press: Totowa, NJ, 2000.
Miller, S. E.; House, D. A. Inorg. Chim. Acta 1991, 187, 125–132.
Berners-Price, S. J.; Sadler, P. J. Coord. Chem. Rev. 1996, 151, 1–40.
Appleton, T. G.; Hall, J. R.; Ralph, S. F. Inorg. Chem. 1985, 24, 4685–4693.
Kozelka, J.; Legendre, F.; Reeder, F.; Chottard, J. Coord. Chem. Rev. 1999, 190–192, 61–82.
836
Metal Complexes as Drugs and Chemotherapeutic Agents
60. Canovese, L.; Cattalini, L.; Chessa, G.; Tobe, M. L. J. Chem. Soc. Dalton Trans. 1988, 2135–2140.
61. Esposito, B. P.; Najjar, R. Coord. Chem. Rev. 2002, 232, 137–150.
62. Ivanov, A. I.; Christodoulou, J.; Parkinson, J. A.; Barnham, K. J.; Tucker, A.; Woodrow, J.; Sadler, P. J. J. Biol.
Chem. 1998, 273, 14721–14730.
63. Reedijk, J. Chem. Rev. 1999, 99, 2499–2510.
64. Djuran, M. I.; Lempers, E. L. M.; Reedijk, J. Inorg. Chem. 1991, 30, 2648–2652.
65. Appleton, T. G.; Connor, J. W.; Hall, J. R.; Prenzler, P. D. Inorg. Chem. 1989, 28, 2030–2037.
66. Murdoch, P. d. S.; Kratochwil, N. A.; Parkinson, J. A.; Patriarca, M.; Sadler, P. J. Angew Chem., Int. Ed. Engl. 1999,
38, 1949–2951.
67. Lempers, E. L. M.; Inagaki, K.; Reedijk, J. Inorg. Chim. Acta 1988, 152, 201–207.
68. Mitchell, K. A.; Streveler, K. C.; Jensen, C. M. Inorg. Chem. 1993, 32, 2608–2609.
69. Alden, W. W.; Repta, A. J. Chem. Biol. Interact. 1984, 48, 121–124.
70. Murdoch, P. d. S.; Ranford, J. D.; Sadler, P. J.; Berners-Price, S. J. Inorg. Chem. 1993, 32, 2249–2255.
71. Barnham, K. J.; Djuran, M. I.; Murdoch, P. d. S.; Ranford, J. D.; Sadler, P. J. Inorg. Chem. 1996, 35, 1065–1072.
72. Hambley, T. W. J. Chem. Soc., Dalton Trans. 2001, 2711–2718.
73. Cohen, S. M.; Lippard, S. J. Prog. Nucleic Acid Res. Mol. Biol. 2001, 67, 93–130.
74. Brabec, V. DNA Modifications by Antitumor Platinum and Ruthenium Compounds: Their Recognition and Repair;
Academic Press: Amsterdam, 2002; Vol. 71 pp 2–45.
75. Takahara, P. M.; Rosenzweig, A. C.; Frederick, C. A.; Lippard, S. J. Nature 1995, 377, 649–652.
76. Gelasco, A.; Lippard, S. J. Biochemistry 1998, 37, 9230–9239.
77. Schwartz, A.; Marrot, L.; Leng, M. Biochemistry 1989, 28, 7975–7979.
78. Gelasco, A.; Lippard, S. J. Anticancer Activity of Cisplatin and Related Complexes; In Metallopharmaceuticals l:
DNA Interactions. Clarke, M. J.; Sadler, P. J., Eds.; Springer-Verlag: Berlin, 1999; Vol. 1, pp 1–44.
79. Marzilli, L. G.; Saad, J. S.; Kuklenyik, Z.; Keating, K. A.; Xu, Y. J. Am. Chem. Soc. 2001, 123, 2764–2770.
80. Spingler, B.; Whittington, D. A.; Lippard, S. J. Inorg. Chem. 2001, 40, 5596–5602.
81. Mani, S.; Graham, M. A.; Bregman, D. B.; Ivy, P.; Chaney, S. G. Cancer Invest. 2002, 20, 246–263.
82. Woynarowski, J. M.; Faivre, S.; Herzig, M. C.; Arnett, B.; Chapman, W. G.; Trevino, A. V.; Raymond, E.; Chaney,
S. G.; Vaisman, A.; Varchenko, M.; Juniewicz, P. E. Mol. Pharmacol. 2000, 58, 920–927.
83. Coste, F.; Malinge, J. M.; Serre, L.; Shepard, W.; Roth, M.; Leng, M.; Zelwer, C. Nucleic Acids Res. 1999, 27,
1837–1846.
84. Coste, F.; Shepard, W.; Zelwer, C. Acta Crystallogr. D 2002, 58, 431–440.
85. Huang, H.; Zhu, L.; Reid, B. R.; Drobny, G. P.; Hopkins, P. B. Science 1995, 270, 1842–1845.
86. Paquet, F.; Perez, C.; Leng, M.; Lancelot, G.; Malinge, J. M. J. Biomol. Struct. Dyn. 1996, 14, 67–77.
87. Brabec, V.; Leng, M. Proc. Natl. Acad. Sci. USA 1993, 90, 5345–5349.
88. Chu, G. J. Biol. Chem. 1994, 269, 787–790.
89. Zlatanova, J.; Yaneva, J.; Leuba, S. H. Faseb J. 1998, 12, 791–799.
90. Patrick, S. M.; Turchi, J. J. Biochemistry 1998, 37, 8808–8815.
91. Thomas, J. O. Biochem. Soc. Trans. 2001, 29, 395–401.
92. Ohndorf, U. M.; Rould, M. A.; He, Q.; Pabo, C. O.; Lippard, S. J. Nature 1999, 399, 708–712.
93. He, Q.; Ohndorf, U. M.; Lippard, S. J. Biochemistry 2000, 39, 14426–14435.
94. Holford, J.; Sharp, S. Y.; Murrer, B. A.; Abrams, M.; Kelland, L. R. Br. J. Cancer 1998, 77, 366–373.
95. Raynaud, F. I.; Boxall, F. E.; Goddard, P. M.; Valenti, M.; Jones, M.; Murrer, B. A.; Abrams, M.; Kelland, L. R.
Clin. Cancer Res. 1997, 3, 2063–2074.
96. Holford, J.; Raynaud, F.; Murrer, B. A.; Grimaldi, K.; Hartley, J. A.; Abrams, M.; Kelland, L. R., Anticancer Drug
Des. 1998, 13, 1–18.
97. Chen, Y.; Guo, Z.; Parsons, S.; Sadler, P. J. Chem. Eur. J. 1998, 4, 672–676.
98. Chen, Y.; Parkinson, J. A.; Guo, Z.; Brown, T.; Sadler, P. J. Angew Chem., Int. Ed. 1999, 38, 2060–2063.
99. Trigo, J. M.; Beale, P.; Judson, I. R.; Raynaud, F.; Rees, C.; Milan, D.; Wolf, L.; Walker, R.; Hanwell, J.;
Giandomenico, C. ASCO 1999, 648.
100. Mellish, K. J.; Barnard, C. F.; Murrer, B. A.; Kelland, L. R. Int. J. Cancer 1995, 62, 717–723.
101. Hall, M. D.; Hambley, T. W. Coord. Chem. Rev. 2002, 232, 49–67.
102. Lemma, K.; Sargeson, A. M.; Elding, L. I. J. Chem. Soc., Dalton Trans. 2000, 1167–1172.
103. Lemma, K.; Berglund, J.; Farrell, N.; Elding, L. I. J. Biol. Inorg. Chem. 2000, 5, 300–306.
104. Giandomenico, C. M.; Abrams, M. J.; Murrer, B. A.; Vollano, J. F.; Rheinheimer, M. I.; Wyer, S. B.; Bossard, G. E.;
Higgins, III, J. D. Inorg. Chem. 1998, 34, 1015–1021.
105. Carr, J. L.; Tingle, M. D.; McKeage, M. J. Cancer Chemother. Pharmacol. 2002, 50, 9–15.
106. Raynaud, F. I.; Mistry, P.; Donaghue, A.; Poon, G. K.; Kelland, L. R.; Barnard, C. F.; Murrer, B. A.; Harrap, K. R.
Cancer Chemother. Pharmacol. 1996, 38, 155–162.
107. Hartwig, J. F.; Lippard, S. J. J. Am. Chem. Soc. 1992, 114, 5646–5654.
108. Kurata, T.; Tamura, T.; Sasaki, Y.; Fujii, H.; Negoro, S.; Fukuoka, M.; Saijo, N. Jpn J. Clin. Oncol. 2000, 30, 377–384.
109. Kelland, L. R. Exp. Opin. Invest. Drugs 2000, 9, 1373–1382.
110. Farrell, N.; Qu, Y.; Hacker, M. P. J. Med. Chem. 1990, 33, 2179–2184.
111. Farrell, N. Comm. Inorg. Chem. 1995, 16, 373–389.
112. Farrell, N. DNA Binding of Dinuclear Platinum Complexes; In Advances in DNA Sequence Specific Agents. Vol. 2
Hurley, L. H.; Chaires, J. B., Eds.; JAI Press, 1996, pp 187–216.
113. Farrell, N. Cancer Invest. 1993, 11, 578–589.
114. Qu, Y.; Rauter, H.; Soares Fontes, A. P.; Bandarage, R.; Kelland, L. R.; Farrell, N. J. Med. Chem. 2000, 43,
3189–3192.
115. Farrell, N. P.; Qu, Y.; Bierbach, U.; Valsecchi, M.; Menta, E. Structure–activity Relationships within Di- and
Trinuclear Platinum Phase I Clinical Agents; In Cisplatin: Chemistry and Biochemistry of a Leading Anticancer
Drug; Lippert, B., Ed.; Verlag, 1999, pp 479–496.
116. Farrell, N.; Spinelli, S. Dinuclear and Trinuclear Platinum Anticancer Agents; In Uses of Inorganic Chemistry in
Medicine, Farrell, N., Ed.; The Royal Society of Chemistry: Cambridge, 1999, pp 124–134.
Metal Complexes as Drugs and Chemotherapeutic Agents
837
117. Farrell, N. P. Polynuclear Charged Platinum Compounds as a New Class of Anticancer Agents: Toward a New
Paradigm; In Platinum-Based Drugs in Cancer Therapy, Kelland, L. R. and Farrell, N. P., Ed.; Humana Press, 2000,
pp 321–338.
118. Qu, Y.; Appleton, T. G.; Hoeschele, J. D.; Farrell, N. Inorg. Chem. 1993, 32, 2591.
119. Manzotti, C.; Pratesi, G.; Menta, E.; Di Domenico, R.; Cavalletti, E.; Fiebig, H. H.; Kelland, L. R.; Farrell, N.;
Polizzi, D.; Supino, R.; Pezzoni, G.; Zunino, F. Clin. Cancer Res. 2000, 6, 2626–2634.
120. Pratesi, G.; Perego, P.; Polizzi, D.; Righetti, S. C.; Supino, R.; Caserini, C.; Manzotti, C.; Giuliani, F. C.; Pezzoni,
G.; Tognella, S.; Spinelli, S.; Farrell, N.; Zunino, F. Br. J. Cancer 1999, 80, 1912–1919.
121. Perego, P.; Caserini, C.; Gatti, L.; Carenini, N.; Romanelli, S.; Supino, R.; Colangelo, D.; Viano, I.; Leone, R.;
Spinelli, S.; Pezzoni, G.; Manzotti, C.; Farrell, N.; Zunino, F. Mol. Pharmacol. 1999, 55, 528–534.
122. Orlandi, L.; Colella, G.; Bearzatto, A.; Abolafio, G.; Manzotti, C.; Daidone, M. G.; Zaffaroni, N., Eur. J. Cancer
2001, 37, 649–659.
123. Calvert, P. M.; Highley, M. S.; Hughes, A. N.; Plummer, E. R.; Azzabi, A. S. T.; Verrill, M. W.; Camboni, M. G.;
Verdi, E.; Bernareggi, A.; Zucchetti, M.; Robinson, A. M.; Carmichael, J.; Calvert, A. H. Clin. Cancer Res. 1999, 5,
3796s.
124. Sessa, C.; Capri, G.; Gianni, L.; Peccatori, F.; Grasselli, G.; Bauer, J.; Zucchetti, M.; Vigano, L.; Gatti, A.; Minoia,
C.; Liati, P.; Van den Bosch, S.; Bernareggi, A.; Camboni, G.; Marsoni, S. Ann. Oncol. 2000, 11, 977–983.
125. Gourley, C.; Cassidy, J.; Bisset, D.; Camboni, G.; Boyle, D.; Joddrell, D. Proc. AACR 2002, 2760.
126. Calvert, A. H.; Thomas, H.; Colombo, N.; Gore, M.; Earl, H.; Sena, L.; Camboni, G.; Liati, P.; Sessa, C. European
Journal of Cancer 2001, 37 (supp6) Poster Discussion 965. Phase II Clinical Study of BBR3464, a Novel, Bifunctional
Platinum Analogue, in Patients with Advanced Ovarian Cancer, 2001.
127. Scagliotti, G.; Crino, L.; de Marinis, F.; Tonato, M.; Selvaggi, G.; Massoni, F.; Maestri, A.; Gatti, B.; Camboni, G.
European Journal of Cancer 2001, 37 (Supp6) Poster 182. Phase II Trial of BBR3464, a Novel, Bifunctional Platinum
Analogue, in Advanced but Favourable Out-come, Non Small Cell Lung Cancer Patients, 2001.
128. Roberts, J. D.; Peroutka, J.; Farrell, N. J. Inorg. Biochem. 1999, 77, 51–57.
129. Perego, P.; Gatti, L.; Caserini, C.; Supino, R.; Colangelo, D.; Leone, R.; Spinelli, S.; Farrell, N.; Zunino, F. J. Inorg.
Biochem. 1999, 77, 59–64.
130. Guo, Z.; Chen, Y.; Zang, E.; Sadler, P. J. J. Chem. Soc., Dalton Trans. 1997, 4107–4111.
131. Davies, M. S.; Cox, J.; Berners-Price, S.; Barklage, W.; Qu, Y.; Farrell, N. Inorg. Chem. 2000, 39, 1710–1715.
132. Davies, M. S.; Thomas, D. S.; Hegmans, A.; Berners-Price, S. J.; Farrell, N. Inorg. Chem. 2002, 41, 1101–1109.
133. McGregor, T. D.; Hegmans, A.; Kasparkova, J.; Neplechova, K.; Novakova, O.; Penazova, H.; Vrana, O.; Brabec, V.;
Farrell, N. J. Biol. Inorg. Chem. 2002, 7, 397–404.
134. Brabec, V.; Kasparkova, J.; Vrana, O.; Novakova, O.; Cox, J. W.; Qu, Y.; Farrell, N. Biochemistry 1999, 38,
6781–6790.
135. Johnson, A.; Qu, Y.; Van Houten, B.; Farrell, N. Nucleic Acids Res. 1992, 20, 1697–1703.
136. Wu, P. K.; Kharatishvili, M.; Qu, Y.; Farrell, N. J. Inorg. Biochem. 1996, 63, 9–18.
137. McGregor, T. D.; Balcarova, Z.; Qu, Y.; Tran, M. C.; Zaludova, R.; Brabec, V.; Farrell, N. J. Inorg. Biochem. 1999,
77, 43–46.
138. McGregor, T. D.; Bousfield, W.; Qu, Y.; Farrell, N. J. Inorg. Biochem. 2002, 91, 212–219.
139. Walker, G. T.; Stone, M. P.; Krugh, T. R. Biochemistry 1985, 24, 7462–7471.
140. Kim, Y.; Geiger, J. H.; Hahn, S.; Sigler, P. B. Nature 1993, 365, 512–520.
141. Herbert, A.; Rich, A. J. Biol. Chem. 1996, 271, 11595–11598.
142. Gohlke, C.; Murchie, A. I.; Lilley, D. M.; Clegg, R. M. Proc. Natl. Acad. Sci. USA 1994, 91, 11660–11664.
143. Kloster, M. B.; Hannis, J. C.; Muddiman, D. C.; Farrell, N. Biochemistry 1999, 38, 14731–14737.
144. Cox, J. W.; Berners-Price, S. J.; Davies, M. S.; Qu, Y.; Farrell, N. J. Am. Chem. Soc. 2001, 123, 1316–1326.
145. Davies, M. S.; Thomas, D. S.; Hegmans, A.; Berners-Price, S. J.; Qu,Y.; Farrell, N. A Comparison of the kinetics of
formation of 1,4-interstrand crosslinks by the trinuclear clinical agent BBR3464: Preassociation and evidence of
conformational flexibility J. Am. Chem. Soc. submitted for publication.
146. Wang, Y.; Farrell, N.; Burgess, J. D. J. Am. Chem. Soc. 2001, 123, 5576–5577.
147. Qu, Y.; Scarsdale, N. J.; Tran, M. C.; Farrell, N. Cooperative effects in long-range 1,4 DNA-DNA interstrand crosslinks formed by polynuclear platinum complexes: an unexpected syn-orientation of adenine bases outside the binding
sites. J Biol Inorg Chem 2003, 8, 19–28.
148. Rajski, S. R.; Williams, R. M. Chem. Rev. 1998, 98, 2723–2796.
149. Thompson, A. S.; Hurley, L. H. J. Mol. Biol. 1995, 252, 86–101.
150. Seaman, F. C.; Chu, J.; Hurley, L. J. Am. Chem. Soc. 1996, 118, 5383–5395.
151. Qu, Y.; Bloemink, M. J.; Reedijk, J.; Hambley, T. W.; Farrell, N. J. Am. Chem. Soc. 1996, 118, 9307.
152. Kasparkova, J.; Novakova, O.; Vrana, O.; Farrell, N.; Brabec, V. Biochemistry 1999, 38, 10997–11005.
153. Kasparkova, J.; Mellish, K. J.; Qu, Y.; Brabec, V.; Farrell, N. Biochemistry 1996, 35, 16705–16713.
154. Kasparkova, J.; Farrell, N.; Brabec, V. J. Biol. Chem. 2000, 275, 15789–15798.
155. Zehnulova, J.; Kasparkova, J.; Farrell, N.; Brabec, V. J. Biol. Chem. 2001, 276, 22191–22199.
156. Kasparkova, J.; Zehnulova, J.; Farrell, N.; Brabec, V. DNA interstrand crosslinks of novel antitumor trinuclear
platinum complex BBR. Conformation, recognition by HMG-domain proteins and nucleotide excision repair. J Biol
Chem 2002, 277, 48076–48086.
157. Sancar, A. Annu. Rev. Biochem. 1996, 65, 43–81.
158. Servidei, T.; Ferlini, C.; Riccardi, A.; Meco, D.; Scambia, G.; Segni, G.; Manzotti, C.; Riccardi, R. Eur. J. Cancer
2001, 37, 930–938.
159. Wheate, N. J.; Webster, L. K.; Brodie, C. R.; Collins, J. G. Anticancer Drug Des. 2000, 15, 313–322.
160. Komeda, S.; Lutz, M.; Spek, A. L.; Chikuma, M.; Reedijk, J. Inorg. Chem. 2000, 39, 4230–4236.
161. Komeda, S.; Lutz, M.; Spek, A. L.; Yamanaka, Y.; Sato, T.; Chikuma, M.; Reedijk, J. J. Am. Chem. Soc. 2002, 124,
4738–4746.
162. Farrell, N.; Ha, T. T.; Souchard, J. P.; Wimmer, F. L.; Cros, S.; Johnson, N. P. J. Med. Chem. 1989, 32, 2240–2241.
163. Van Beusichem, M.; Farrell, N. Inorg. Chem. 1992, 31, 634.
164. Farrell, N.; Kelland, L. R.; Roberts, J. D.; Van Beusichem, M. Cancer Res. 1992, 52, 5065–5072.
838
Metal Complexes as Drugs and Chemotherapeutic Agents
165. Natile, G.; Coluccia, M. Trans-platinum Compounds in Cancer Therapy: A Largely Unexplored Strategy for
Identifying Novel Antitumor Platinum Drugs; In Metallopharmaceuticals l: DNA Interactions, Clarke, M. J.; Sadler,
P. J., Eds.; Springer-Verlag: Berlin, 1999; Vol. 1, pp 73–98.
166. Natile, G.; Coluccia, M. Coord Chem. Rev. 2001, 216, 383–410.
167. Perez, J. M.; Montero, E. I.; Gonzalez, A. M.; Solans, X.; Font-Bardia, M.; Fuertes, M. A.; Alonso, C.; NavarroRanninger, C. J. Med. Chem. 2000, 43, 2411–2418.
168. Montero, E. I.; Diaz, S.; Gonzalez-Vadillo, A. M.; Perez, J. M.; Alonso, C.; Navarro-Ranninger, C. J. Med. Chem.
1999, 42, 4264–4268.
169. Khazanov, E.; Barenholz, Y., Gibson, D., Najraeh, Y. Novel apoptosis-including trans-platinum piperidine and
piperazine derivatives: Synthesis and biological characterization. J. Med. Chem. 2002, 45, 5189–5195 .
170. Farrell, N. Met. Ions Biol. Sys. 1996, 32, 603–634.
171. Bierbach, U.; Sabat, M.; Farrell, N. Inorg. Chem. 2000, 39, 1882–1890.
172. Zou, Y.; Van Houten, B.; Farrell, N. Biochemistry 1993, 32, 9632–9638.
173. Brabec, V.; Neplechova, K.; Kasparkova, J.; Farrell, N. J. Biol. Inorg. Chem. 2000, 5, 364–368.
174. Bierbach, U.; Qu, Y.; Hambley, T. W.; Peroutka, J.; Nguyen, H. L.; Doedee, M.; Farrell, N. Inorg. Chem. 1999, 38,
3535–3542.
175. Bierbach, U.; Farrell, N. Inorg. Chem. 1997, 36, 3657–3665.
176. Bierbach, U.; Farrell, N. J. Biol. Inorg. Chem. 1998, 3, 570.
177. Zaludova, R.; Zakovska, A.; Kasparkova, J.; Balcarova, Z.; Vrana, O.; Coluccia, M.; Natile, G.; Brabec, V. Mol.
Pharmacol. 1997, 52, 354–361.
178. Clarke, M. J.; Zhu, F.; Frasca, D. R. Chem. Rev. 1999, 99, 2511–2534.
179. Clarke, M. J. Ruthenium Chemistry Pertaining to the Design of Anticancer Agents; Progress in Clinical Biochemistry
and Medicine; Springer-Verlag: Berlin, 1989; Vol. 10, pp 25–40.
180. Frasca, D. R.; Clarke, M. J. J. Am. Chem. Soc. 1999, 121, 8523–8532.
181. Zhao, M.; Clarke, M. J. J. Biol. Inorg. Chem. 1999, 4, 318–324.
182. LaChance-Galang, K.; Zhao, M.; Clarke, M. J. Inorg. Chem. 1996, 35, 6021–6026.
183. Keppler, B. K.; Friesen, C.; Moritz, H. G.; Vongerichten, H.; Vogel, E. Struct. Bonding 1991, 78, 97–127.
184. Pieper, T.; Borsky, K.; Keppler, B. K. Non-platinum Antitumor Compounds; In Metallopharmacecuticals l: DNA
Interactions, Clarke, M. J.; Sadler, P. J., Eds.; Springer-Verlag: Berlin, 1999; Vol.1, pp , 171–199.
185. Kratz, F.; Hartmann, M.; Keppler, B.; Messori, L. J. Biol. Chem. 1994, 269, 2581–2588.
186. Sava, G.; Alessio, E.; Bergamo, A.; Mestroni, G. Sulfoxide Ruthenium Complexes: Non Toxic Tools for the Selective
Treatment of Solid Tumor Metastases; In Metallopharmaceuticals l: DNA Interactions, Clarke, M. J. and Sadler, P. J.,
Ed.; Springer-Verlag: Berlin, 1999; Vol.1, pp 143–170.
187. Sanna, B.; Debidda, M.; Pintus, G.; Tadolini, B.; Posadino, A. M.; Bennardini, F.; Sava, G.; Ventura, C. Arch.
Biochem. Biophys. 2002, 403, 209–218.
188. Cherrington, J. M.; Strawn, L. M.; Shawver, L. K. Adv. Cancer Res. 2000, 79, 1–38.
189. Sava, G.; Clerici, K.; Capozzi, I.; Cocchietto, M.; Gagliardi, R.; Alessio, E.; Mestroni, G.; Perbellini, A. Anticancer
Drugs 1999, 10, 129–138.
190. Bergamo, A.; Gagliardi, R.; Scarcia, V.; Furlani, A.; Alessio, E.; Mestroni, G.; Sava, G. J. Pharmacol. Exp. Ther.
1999, 289, 559–564.
191. Zorzet, S.; Bergamo, A.; Cocchietto, M.; Sorc, A.; Gava, B.; Alessio, E.; Iengo, E.; Sava, G. J. Pharmacol. Exp. Ther.
2000, 295, 927–933.
192. Sava, G.; Bergamo, A.; Zorzet, S.; Gava, B.; Casarsa, C.; Cocchietto, M.; Furlani, A.; Scarcia, V.; Serli, B.; Iengo, E.;
Alessio, E.; Mestroni, G. Eur. J. Cancer 2002, 38, 427–435.
193. Gopal, Y. N.; Jayaraju, D.; Kondapi, A. K. Biochemistry 1999, 38, 4382–4388.
194. Chen, H.; Parkinson, J. A.; Parsons, S.; Coxall, R. A.; Gould, R. O.; Sadler, P. J. J. Am. Chem. Soc. 2002, 124,
3064–3082.
195. Morris, R. E.; Aird, R. E.; Murdoch Pdel, S.; Chen, H.; Cummings, J.; Hughes, N. D.; Parsons, S.; Parkin, A.; Boyd, G.;
Jodrell, D. I.; Sadler, P. J. J. Med. Chem. 2001, 44, 3616–3621.
196. Antman, K. H. Oncologist 2001, 6, 1–2.
197. Waxman, S.; Anderson, K. C. Oncologist 2001, 6, 3–10.
198. Shen, Z. X.; Chen, G. Q.; Ni, J. H.; Li, X. S.; Xiong, S. M.; Qiu, Q. Y.; Zhu, J.; Tang, W.; Sun, G. L.; Yang, K. Q.;
Chen, Y.; Zhou, L.; Fang, Z. W.; Wang, Y. T.; Ma, J.; Zhang, P.; Zhang, T. D.; Chen, S. J.; Chen, Z.; Wang, Z. Y.
Blood 1997, 89, 3354–3360.
199. Novick, S. C.; Warrell, R. P., Jr. Semin. Oncol. 2000, 27, 495–501.
200. Rust, D. M.; Soignet, S. L. Oncologist 2001, 6, 29–32.
201. Miller, W. H., Jr.; Schipper, H. M.; Lee, J. S.; Singer, J.; Waxman, S. Cancer Res. 2002, 62, 3893–3903.
202. Jing, Y.; Dai, J.; Chalmers-Redman, R. M.; Tatton, W. G.; Waxman, S. Blood 1999, 94, 2102–2111.
203. Dai, J.; Weinberg, R. S.; Waxman, S.; Jing, Y. Blood 1999, 93, 268–277.
204. Yang, C. H.; Kuo, M. L.; Chen, J. C.; Chen, Y. C. Br. J. Cancer 1999, 81, 796–799.
205. Zhang, T. D.; Chen, G. Q.; Wang, Z. G.; Wang, Z. Y.; Chen, S. J.; Chen, Z. Oncogene 2001, 20, 7146–7153.
206. Kroemer, G.; de The, H. J. Natl. Cancer Inst. 1999, 91, 743–745.
207. Preston, T. J.; Abadi, A.; Wilson, L.; Singh, G. Adv. Drug Deliv. Rev. 2001, 49, 45–61.
208. Costantini, P.; Jacotot, E.; Decaudin, D.; Kroemer, G. J. Natl. Cancer Inst. 2000, 92, 1042–1053.
209. Koya, K.; Li, Y.; Wang, H.; Ukai, T.; Tatsuta, N.; Kawakami, M.; Shishido; Chen, L. B. Cancer Res. 1996, 56,
538–543.
210. McKeage, M.J.; Maharaj, L.; Berners-Price, S. J. Coord. Chem. Rev. 2002, 232, 127–135.
211. Berners-Price, S. J.; Bowen, R. J.; Galettis, P.; Healy, P. C.; McKeage, M. J. Coord. Chem. Rev. 1999, 185–186,
823–836.
212. Berners-Price, S.; Jarrett, P.; Sadler, P. Inorg. Chem. 1987, 26, 3074–3077.
213. Shaw, C. F. Chem. Rev. 1999, 99, 2589–2600.
214. Berners-Price, S. J.; Girard, G. R.; Hill, D. T.; Sutton, B. M.; Jarrett, P. S.; Faucette, L. F.; Johnson, R. K.;
Mirabelli, C. K.; Sadler, P. J. J. Med. Chem. 1990, 33, 1386–1392.
Metal Complexes as Drugs and Chemotherapeutic Agents
839
215. McKeage, M. J.; Berners-Price, S. J.; Galettis, P.; Bowen, R. J.; Brouwer, W.; Ding, L.; Zhuang, L.; Baguley, B. C.
Cancer Chemother. Pharmacol. 2000, 46, 343–350.
216. Berners-Price, S.; Bowen, R.; Hambley, T.; Healy, P. J. Chem. Soc., Dalton Trans. 1999, 8, 1337–1346.
217. Riley, D. P. Chem. Rev. 1999, 99, 2573–2588.
218. McCord, J. M.; Fridovich, I. J. Biol. Chem. 1969, 244, 6049–6055.
219. Kramer, R. Angew Chem., Int. Ed. 2000, 39, 4469–4470.
220. Weiss, R.; Riley, D. Therapeutic Aspects of Manganese(II)-based Superoxide Dismutase Mimics; In Uses of Inorganic
Chemistry in Medicine, Farrell, N., Ed.; The Royal Society of Chemistry: Cambridge, 1999, pp 77–92.
221. Doctrow, S. R.; Huffman, K.; Marcus, C. B.; Musleh, W.; Bruce, A.; Baudry, M.; Malfroy, B. Adv. Pharmacol. 1997,
38, 247–269.
222. Melov, S.; Ravenscroft, J.; Malik, S.; Gill, M. S.; Walker, D. W.; Clayton, P. E.; Wallace, D. C.; Malfroy, B.;
Doctrow, S. R.; Lithgow, G. J. Science 2000, 289, 1567–1569.
223. Salvemini, D.; Wang, Z. Q.; Zweier, J. L.; Samouilov, A.; Macarthur, H.; Misko, T. P.; Currie, M. G.; Cuzzocrea, S.;
Sikorski, J. A.; Riley, D. P. Science 1999, 286, 304–306.
224. Aston, K.; Rath, N.; Naik, A.; Slomczynska, U.; Schall, O. F.; Riley, D. P. Inorg. Chem. 2001, 40, 1779–1789.
225. Melendez, E. Crit. Rev. Oncol. Hematol. 2002, 42, 309–315.
226. Comba, P.; Jakob, H.; Nuber, B.; Keppler, B. K. Inorg. Chem. 1994, 33, 3396–3400.
227. Schilling, T.; Keppler, K. B.; Heim, M. E.; Niebch, G.; Dietzfelbinger, H.; Rastetter, J.; Hanauske, A. R. Invest.
New Drugs 1996, 13, 327–332.
228. Christodoulou, C. V.; Ferry, D. R.; Fyfe, D. W.; Young, A.; Doran, J.; Sheehan, T. M.; Eliopoulos, A.; Hale, K.;
Baumgart, J.; Sass, G.; Kerr, D. J. J. Clin. Oncol. 1998, 16, 2761–2769.
229. Korfel, A.; Scheulen, M. E.; Schmoll, H. J.; Grundel, O.; Harstrick, A.; Knoche, M.; Fels, L. M.; Skorzec, M.; Bach, F.;
Baumgart, J.; Sass, G.; Seeber, S.; Thiel, E.; Berdel, W. E. Clin. Cancer Res. 1998, 4, 2701–2708.
230. Lummen, G.; Sperling, H.; Luboldt, H.; Otto, T.; Rubben, H. Cancer Chemother. Pharmacol. 1998, 42, 415–417.
231. Harding, M. M.; Mokdsi, G. Curr. Med. Chem. 2000, 7, 1289–1303.
232. Kuo, L. Y.; Liu, A. H.; Marks, T. J. Met. Ions Biol. Syst. 1996, 33, 53–85.
233. Harding, M. M.; Mokdsi, G.; Lucas, W. Inorg. Chem. 1998, 37, 2432–2437.
234. Sun, H.; Li, H.; Weir, R. A.; Sadler, P. J. Angew Chem., Int. Ed. Engl. 1998, 37, 1577–1579.
235. Apseloff, G. Am. J. Ther. 1999, 6, 327–339.
236. Webster, L. K.; Olver, I. N.; Stokes, K. H.; Sephton, R. G.; Hillcoat, B. L.; Bishop, J. F. Cancer Chemother.
Pharmacol. 2000, 45, 55–58.
237. Senderowicz, A. M.; Reid, R.; Headlee, D.; Abornathy, T.; Horti, J.; Lush, R. M.; Reed, E.; Figg, W. D.; Sausville,
E. A. Urol. Int. 1999, 63, 120–125.
238. Collery, P.; Lechenault, F.; Cazabat, A.; Juvin, E.; Khassanova, L.; Evangelou, A.; Keppler, B. Anticancer Res. 2000,
20, 955–958.
239. Arion, V. B.; Jakupec, M. A.; Galanski, M.; Unfried, P.; Keppler, B. K. J. Inorg. Biochem. 2002, 91, 298–305.
240. Knorr, G. M.; Chitambar, C. R. Anticancer Res. 1998, 18, 1733–1737.
241. Grier, N. Mercurials—Inorganic and Organic. In Mercurials—Inorganic and Organics (Disinfection, Sterilization and
Preservation.), Block, S. S., Ed.; Lea and Fabringer, 1983, pp 346–374.
242. Grier, N. Silver and Its Compounds. In Mercurials—Inorganic and Organics (Disinfection, Sterilization and Preservation.), Block, S. S., Ed.; Lea and Fabringer, 1983, pp 375–389.
243. Gupta, A.; Matsui, K.; Lo, J. F.; Silver, S. Nat. Med. 1999, 5, 183–188.
244. Clement, J. L.; Jarrett, P. S. Met. Based Drugs 1994, 1, 467–782.
245. Briand, G. G.; Burford, N. Chem. Rev. 1999, 99, 2601–2658.
246. Reglinski, J. Chemistry of Arsenic, Antimony, and Bismuth; Blackie Academic & Professional: London 1998.
247. Briand; Burford, N. Adv. Inorg. Chem. 2002, 50, 285–357.
248. Asato, E.; Driessen, W. L.; de Graaff, R. A. G.; Hulsbergen, F. B.; Reedijk, J. Inorg. Chem. 1991, 30, 4210–4218.
249. Asato, E.; Katsura, K.; Mikuriya, M.; Fujii, T.; Reedijk, J. Inorg. Chem. 1993, 32, 5322–5329.
250. Asato, E.; Katsura, K.; Mikuriya, M.; Turpeinen, U.; Mutikainen, I.; Reedijk, J. Inorg. Chem. 1995, 34, 2447–2454.
251. Sadler, P. J.; Li, H.; Sun, H. Coord. Chem. Rev. 1999, 185-186, 689–709.
252. Sadler, P. J.; Sun, H. J. Chem. Soc., Dalton Trans. 1995, 1395–1401.
253. Burford, N.; Eelman, M. D.; Cameron, T. S. Chem. Commun. (Camb) 2002, 1402–1403.
254. Whitmire, K. J. Chem. Soc. Chem. Commun. 2002, 2834–2835..
255. Sadler, P. J.; Sun, H. Z.; Li, H. Y. Chem. Eur. J. 1996, 2, 701–708.
256. Sun, H.; Li, H.; Mason, A. B.; Woodworth, R. C.; Sadler, P. J. Biochem. J. 1999, 337, 105–111.
257. Navarro, M.; Perez, H.; Sanchez-Delgado, R. A. J. Med. Chem. 1997, 40, 1937–1939.
258. Navarro, M.; Cisneros-Fajardo, E. J.; Lehmann, T.; Sanchez-Delgado, R. A.; Atencio, R.; Silva, P.; Lira, R.; Urbina,
J. A. Inorg. Chem. 2001, 40, 6879–6884.
259. Sanchez-Delgado, R. A.; Lazardi, K.; Rincon, L.; Urbina, J. A. J. Med. Chem. 1993, 36, 2041–2043.
260. Sanchez-Delgado, R. A.; Navarro, M.; Perez, H.; Urbina, J. A. J. Med. Chem. 1996, 39, 1095–1099.
261. Birch, N. Biomedical Uses of Lithium; Farrell, N., Ed.; The Royal Society of Chemistry: Cambridge, 1999, pp 11–21.
262. Birch, N. J. Chem. Rev. 1999, 99, 2659–2682.
263. Orvig, C.; Thompson, K. H.; Battell, M.; McNeill, J. H. Metal Ions in Biological Systems: Vanadium and its Role in
Life; In Metal Ions in Biological Systems, Sigel, H.; Sigel, A.; Eds.; Marcel Dekker: New York, 1995; Vol. 31, p 575.
264. Blondel, O.; Simon, J.; Chevalier, B.; Portha, B. Am. J. Physiol. 1990, 258, E459–E467.
265. Thompson, K. H.; McNeill, J. H.; Orvig, C. Chem. Rev. 1999, 99, 2561–2572.
266. Orvig, C.; Thompson, K.; Cam, M.; McNeil, J. Vanadium Compounds as Possible Insulin Modifiers; In Uses of
Inorganic Chemistry in Medicine, Farrell, N. Ed.; The Royal Society of Chemistry: Cambridge, 1999, pp 93–108.
267. Huyer, G.; Liu, S.; Kelly, J.; Moffat, J.; Payette, P.; Kennedy, B.; Tsaprailis, G.; Gresser, M. J.; Ramachandran, C.
J. Biol. Chem. 1997, 272, 843–851.
268. Elberg, G.; He, Z.; Li, J.; Sekar, N.; Shechter, Y. Diabetes 1997, 46, 1684–1690.
269. Shaw, C. Gold Complexes with Anti-arthritic, Anti-tumour and Anti-HIV Activity; In Uses of Inorganic Chemistry in
Medicine, Farrell, N., Ed.; The Royal Society of Chemistry: Cambridge, 1999, pp 26–57.
840
Metal Complexes as Drugs and Chemotherapeutic Agents
270. Snyder, R. M.; Mirabelli, C. K.; Crooke, S. T. Semin. Arthritis Rheum. 1987, 17, 71–80.
271. Rudkowski, R.; Graham, G. G.; Champion, G. D.; Ziegler, J. B. Biochem. Pharmacol. 1990, 39, 1687–1695.
272. Butler, A.; Rhodes, P. Nitric Oxide in Physiology and Medicine; In Uses of Inorganic Chemistry in Medicine, Farrell, N.,
Ed.; The Royal Society of Chemistry: Cambridge, 1999, pp 58–76.
273. Clarke, M. J.; Gaul, J. B. Struct. Bonding 1993, 81, 147–181.
274. Butler, A. R.; Williams, D. L. H. Chem. Soc. Rev. 1993, 22, 233–241.
275. Groves, J. T. Curr. Opin. Chem. Biol. 1999, 3, 226–235.
276. Shimanovich, R.; Groves, J. T. Arch. Biochem. Biophys. 2001, 387, 307–317.
277. Shimanovich, R.; Hannah, S.; Lynch, V.; Gerasimchuk, N.; Mody, T. D.; Magda, D.; Sessler, J.; Groves, J. T. J. Am.
Chem. Soc. 2001, 123, 3613–3614.
278. Hergesell, O.; Ritz, E. Kidney Int. 1999, 73, S42–S45.
279. Hutchison, A. J. Perit. Dial. Int. 1999, 19, S408–S412.
280. Hergesell, O.; Ritz, E., Phosphate binders on iron basis: a new perspective? Kidney Int. Suppl. 1999, 73, S42–45.
# 2003, Elsevier Ltd. All Rights Reserved
No part of this publication may be reproduced, stored in any retrieval system or
transmitted in any form or by any means electronic, electrostatic, magnetic tape,
mechanical, photocopying, recording or otherwise, without permission in writing
from the publishers
Comprehensive Coordination Chemistry II
ISBN (set): 0-08-0437486
Volume 9, (ISBN 0-08-0443311); pp 809–840