Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
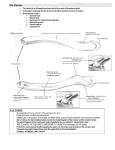
Clavicle Distinguish the motion of the clavicle from the glenohumeral & scapular motion - - Sternoclavicular joint: o The only true joint that attaches the UE to the thoracic cage o Complex synovial joint with cartilaginous meniscus o 3 pairs of motion of clavicle= abduction(elevation)/adduction(depression), horizontal flexion/extension & internal/external rotation Acromioclavicular joint: o Planar joint with rudimentary crescent-shaped incomplete meniscus o Clavicle motion here is just a small amount of glide (superior/inferior, anterior/posterior & rotational) o Clavicle SD usually has TTP at AC joint Characterize the reciprocal motion between distal & proximal ends of the clavicle - Reciprocal superior/inferior & anterior/posterior motion between ends (fulcrum= costoclavicular ligament) Non-reciprocal rotation along long axis (fulcrum= sternoclavicular joint) Must remain mobile to allow for optimal motion of shoulder/upper extremity & upper rib cage More motion available at distal end than proximal end, but more motion at SC joint than at AC joint In general, when discussing motion at a joint in the appendicular skeleton, we are referring to how the distal bone moves in relation to the more proximal bone Yet, somatic dysfunction at an appendicular joint can be due to restriction of either the distal end of the proximal bone or the proximal end of the distal bone Diagnose dysfunctions of the AC & SC joints - - Somatic dysfunction: o Altered mechanics causes increased wear & tear on associated joints & ultimately results in osteoarthritis o Altered mechanics also causes increased susceptibility of the joint & surrounding structures to injury (sprains, strains & fracture) o Fascial pull due to the dysfunction causes distortion of the fascial coverings resulting in mechanical impediments to the flow of liquids & causes buildup of waste products & decreased ability to deliver nutrients & O2. This in turn, increases the physiological stress in the area, which can result in more dysfunction of the soma… cycle of worsening dysfunction. o Patient activity may be limited due to mechanical inability or due to pain causing psychological discouragement from engaging in the activity Decreased activity can have a myriad of physical, mental & social effects “Clavicle” can be involved in dysfunction of the Thoracic Outlet & Inlet o Thoracic outlet- subclavian artery & vein, lymphatic vessels & brachial plexus pass through o Thoracic Inlet- important structures pass through near SC joint o We can use a bone that does not move the way it should (ie. restricted or having SD) as a sign that something connected to it is causing inappropriate tension to be applied to that bone - - - - o AC separation o Sprain (with or without tear) of the acromioclavicular ligament o Is it somatic dysfunction? YES, but OMT doesn’t have any direct effect on correcting anatomical barriers But how could OMT be useful in someone with an AC separation (ie. help enhance the patient’s natural healing abilities)? OMT could benefit a patient with an AC separation by removing impediments to the motion & enhance the patient’s ability to heal up the injury/avoid further injury o Look for Sulcus sign & step off deformity o Bilateral shoulder XR w/& w/o weight bearing Local somatic dysfunction that tends to affect clavicular motion: o Bones that articulate with the clavicle (scapula, manubrium, rib 1) o Muscles that attach to the clavicle (trapezius, deltoid, pectoralis major, subclavius, sternocleidomastoid & sternohyoid) o Fascial restrictions from other nearby soft tissue structures When describing clavicular SD, you can speak in terms of the ends of the clavicle or the whole clavicle: o Proximal end- superior/inferior or anterior/posterior SD o Distal end- superior/inferior or anterior/posterior SD o Whole clavicle- internal/external rotation SD Some DOs do talk about AC joint motion dysfunction without specifying whether it is the A (acromion of the scapula) or C (clavicle) that has the restriction. This is likely due to them employing the same technique regardless of which has the restriction (for example, muscle energy OMT). Yet, some other types of OMT would require a more precise diagnosis. Explain how to set up & perform osteopathic techniques for the AC & SC joints - Muscle Energy o Indication: Somatic dysfunction o Contraindications: Absolute Lack of patient consent and/or cooperation Relative Infection, hematoma, or tear in involved muscle Fracture or dislocation of involved joint Rheumatologic conditions causing instability of the cervical spine Undiagnosed joint swelling of involved joint Positioning that compromises vasculature - - - - Soft Tissue (ST) o A direct technique that usually involves lateral stretching, linear stretching, deep pressure, traction and/or separation of muscle origin and insertion while monitoring tissue response and motion changes by palpation Also called (direct) myofascial treatment o Indication: Presence of a CS point o Contraindications: Absolute Lack of patient consent and/or cooperation Relative contraindications for local application Skin: Disorders which would preclude skin contact, e.g., contagious skin diseases, acute burns, painful rashes, abscesses, skin cancers, etc. Fascia: Acute fasciitis (infectious or autoimmune), acute fascial tears Muscle: Acute muscular strains, acute myositis, muscle neoplasms. Ligament: Acute ligamentous sprain, acute ligamentous inflammatory disorders, septic arthritis, primary or secondary joint neoplasms. Bone: Acute fracture, osteomyelitis, primary or secondary bone tumors, osteoporosis Joint: Septic joint, joint instability/collagen disorders Viscera: Infection, neoplasm, or organomegaly i.e. the liver /spleen. Gastric or bowel obstruction or distention. Acute or undiagnosed abdominal or pelvic pain Vascular: Hematoma, deep venous thrombosis, coagulopathy Trigger Point o A small hypersensitive site that, when stimulated, consistently produces a reflex mechanism that gives rise to referred pain and/or other manifestations in a consistent reference zone that is consistent from person to person. o Located in consistent, specific spots o Locally tender o Characteristic radiating pain pattern o Located in muscle tissue o Patient may or may not be aware of pain at the point before pressure is applied Tender Point o Located in consistent, specific spots o Locally tender o No radiation of pain o Located in muscle, tendon, & ligament o Patient is most often unaware of pain at the point until pressure is applied (Jones) Strain-Counterstrain o A system of diagnosis and treatment that considers the dysfunction to be a continuing, inappropriate strain reflex, which is inhibited by applying a position of mild strain in the direction exactly opposite to that of the reflex; this is accomplished by specific directed positioning about the point of tenderness to achieve the desired therapeutic response o This is accomplished by specific directed positioning about the point of tenderness (aka tender point) to achieve the desired therapeutic response o An indirect technique in which the tissue being treated is positioned towards a point of balance, or ease, away from the restrictive barrier o Counterstrain is based on identifying counterstrain tender points o Physiologic mechanism: The exact physiologic mechanism of counterstrain is unknown. o o o o The most commonly accepted theory is that the mechanism of dysfunction is proprioceptive in origin and is due to aberrant neuromuscular activity mediated by muscle spindle fibers. The primary proprioceptor in the antagonist is suddenly changed from maximal shortening to panic lengthening so fast as to report strain before ever reaching its neutral length. From then on it reports strain where there is none Other possible contributors to the formation of or maintenance of counterstrain points: nociceptive reflexes, spinal fixation, neurovascular bundle impingement & centrallymediated causes Jones theory/commonly accepted theory: Strain= Rapid shortening in one muscle (the agonist) Counterstrain= this produces a rapid lengthening of the antagonist muscle Afferent feedback indicates possible myofascial damage in the antagonist muscle from the “strain” (stress) Body attempts to prevent damage by contracting the tissues that it believes are threatened by the rapid lengthening (ie. the antagonist) This produces an inappropriate reflex that manifests as a counterstrain tender point in the antagonist muscle Indication: Presence of a CS point Contraindications: Absolute (KNOW THESE) Lack of patient consent and/or cooperation Inability to tolerate the classic treatment position, meaning that the treatment position must be modified Manifestation of neurological symptoms brought on by the treatment position Exacerbation of potentially life-threatening symptomatology by treatment position (EKG changes, drop in O2 saturation, etc in a monitored patient) Relative Patient who cannot voluntarily relax Severely ill patient Upper cervical hyperrotation and hyperextension in patients with known vertebral artery disease or upper cervical ligamentous instability or dens malformation Severe osteoporosis Inability to tolerate the classic treatment position, meaning that the treatment position must be modified Inability to effectively communicate Patient with severe acute rheumatological flare Signs of apprehension while approaching the treatment position CLASSICAL STEPS OF TREATMENT FOR COUNTERSTRAIN: ***KNOW THIS*** 1. Identify a CS point Usually use tip of index finger to palpate for one It should be TTP at that point, but not so much in the surrounding tissues Should have tissue texture abnormality (TTA) different than the surrounding tissues Should not refer pain elsewhere If no contraindications, then you may treat 2. Stop pressing so hard! but keep your finger on the point so you can monitor the TTA 3. Establish a pain scale o o Tell the patient to think of the pain they felt when you were pushing on the point as 100% 4. Position the patient into the treatment position 5. Push on the CS point again briefly & ask patient how much the pain has improved (ie. what number would they give it now) [want pain reduced by at least 70% (ie. only hurts 30 or less)] 6. Hold position for 90 seconds (patient needs to be relaxed during steps 6 & 7) 7. Passively reposition the patient to neutral 8. Repeat step 5 Likely neurophysiolgic mechanism of CS positioning Shortening the muscle without it being actively contracted, reduces tension in the area & allows for increased microcirculation This alters neural afferent input Which alters neural efferent output Which allows normalization of neural signaling feedback loops Thus patient can tolerate more mechanical stress being applied to the point before it causes activation of pain signal or reflexes that would interfere with maximal lengthening of that muscle Counterstrain Considerations for Muscles Attached to Clavicle: Sternocleidomastoid (SCM): Origin: Anterior and superior manubrium and superior medial third of clavicle Insertion: Lateral aspect of mastoid process and lateral half of superior nuchal line Maximal shortened position: Neck sidebent to ipsilateral side & rotated opposite Upper trapezius Origin: Medial third superior nuchal line, ligament nuchae, spinous processes and supraspinous ligaments to C7 Insertion: Upper fibers to lateral third of posterior border of clavicle Maximal shortened position: Clavicle & scapula elevated. Neck extended and sidebent to ipsilateral side Anterior deltoid Origin: Lateral third of clavicle Insertion: Middle of lateral surface of humerus (deltoid tuberosity) Maximal shortened position: UE flexed, abducted, and internally rotated Pectoralis major Origin: Clavicular head= medial half of clavicle; Sternocostal head= lateral manubrium and sternum, six upper costal cartilages and external oblique aponeurosis Insertion: Lateral lip of bicipital groove of humerus and anterior lip of deltoid tuberosity Maximal shortened position: Clavicular head= UE flexed ~900 and adducted; Sternal head= UE flexed ~450, adducted and internally rotated Anatomy - - Clavicle o Double-curved long bone (S shape) o Serves as a strut suspending the scapula and limb to allow maximum, controlled freedom of motion o Sternal end articulates with manubrium of sternum Sternoclavicular (SC) joint o Acromial end articulates with acromion o Acromioclavicular (AC) joint Ligaments o Proximal End: Sternoclavicular ligament Costoclavicular ligament o - Interclavicular ligament Distal End: Coracoclavicular ligament Conoid ligament Trapezoid ligament Acromioclavicular ligament **usually 1st ligament torn when injured