Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
By: Roberta Boon
Facilitator: Professor Kolp
Indiana Wesleyan University
December, 2014
I have read and understand the plagiarism policy as outlined in
the syllabus and the sections in the Student bulletin relating to the
IWU Honesty/Cheating Policy. By affixing this statement to the title
page of my paper, I certify that I have not cheated or plagiarized in
the process of completing this assignment. If it is found that cheating
and/or plagiarism did take place in the writing of this paper, I
understand the possible consequences of the act/s, which could
include expulsion from Indiana Wesleyan University.
Birth to 1 month old (Neonate)
Neonates (0-4 weeks) are likely to lay flexed with head turned to a side with
the primitive reflexes. They can turn head when cheek is stroked (rooting reflex)
and have the basic innate reflexes. The reflex for sucking, palmar grasp, ankle
clonus with stepping reflex. The moro reflex or startle occurs with loud sounds or
with sudden change in movement of the infant and may last for about 6 months
(Burns, Dunn, Brady, Starr, & Blosser, 2013).
Patterns of Behavior:
In the prone position will have the head sag during ventral suspension.
The muscle tone is stiff and flexed.
Fixates on light and has a present red reflex.
Prefers to look at faces of people (Kliegman, Stanton, St. Geme, Schor, & Behrman,
2011).
Birth weight must be obtained at 2 week examination(Burns et al., 2013).
When approaching a month old will:
Keep legs more extended. Occasionally will lift head for a
moment. Has a tonic neck which is relaxed. Head lag present
with moving to sitting.
Follows movement with eyes (Kliegman et al., 2011).
1 month to 9 months old
At one month is beginning to have a social smile.
At two months is:
•
Raising head farther and can maintain head is plane with body.
•
Has head lag when moved to sitting position.
•
Follows moving object in 180 degrees fashion.
Has a social smile. Nearby voices are mimicked by coos (Kliegman et al., 2011).
At 4 months is:
•
Can lift head and chest. Can reach and grasp objects to bring to mouth.
•
Moro reflex is gone. When held upright will push with feet. May laugh out loud
•
(Fitzgerald, 2010; Kliegman et al., 2011).
At 6 months is:
•
Stranger and separation anxiety begin.
•
Starting to roll over and crawl. Solid food is best introduced at this time.
•
May sit briefly. With support will bounce actively (Fitzgerald, 2010;
Fitzgerald, 2010).
9 months to 12 months
At 9 months is:
•
Sits without support. Stands with support by use of furniture.
•
Cruises by moving around with support and pulls self to standing.
•
Starts to make repetitive sounds “Mama, Dada, and Bye-bye” with hand
gestures and plays peek-a-boo (Burns et al., 2013, Kliegman et al., 2011).
At 10 months:
•
•
Sits up alone and grasps at objects.
Picks up small objects with thumb and forefinger (Kliegman et al., 2011; Fitzgerald,
2010).
At 12 months:
•
•
•
•
•
Walks with one hand held. Rises from sitting independently. Can play simple ball
games (Kliegman et al., 2011).
Say at least 1 word.
Point to items they want that are out of reach or make sounds while
pointing.
Respond to their name most of the time when you call it.
Should be transitioning from breast or bottle feeding to sippy-cup
with iron fortified cereals (Burns et al., 2013).
15 months to 30 months
At 15 months:
Can point to and name body parts.
Walks alone, but crawls up stairs.
Can make a tower by 3 cubes, and can draw a line(Fitzgerald, 2010; Kliegman et al.,
2011).
At 18 months:
Throws a ball overhand. Runs some; walks up stairs.
Uses about 10 words and can feed self. May complain when wet or irritable
(Fitzgerald, 2010; Kliegman et al., 2011).
At 24 months:
Runs well, walks up and down steps.
Can kick a ball. Assists with putting on clothing and taking them off.
Can say about 300 words and is stringing together words to make simple sentences
(Fitzgerald, 2010; Kliegman et al., 2011).
At 30 months:
Goes up stairs with alternating feet; walks backwards.
Knows age and sex and can ride a tricycle. Can hop on one foot.
Copies circles and can stack a tower of 9 cubes (Fitzgerald, 2010; Kliegman et al.,
2011).
36 months to 60 months
At 36 months:
Speech is understandable by others outside of family.
Uses 3 word sentences and plays simple games with other children.
Knows age and sex and is able to wash hands.
Copies circles and dresses with supervision (Fitzgerald, 2010; Kliegman et al., 2011).
At 48 months:
Runs and turns while maintaining balance. Hops on one foot.
Can count 4 pennies and can tell a story. Can draw a stick figure man.
Can verbalize when hungry, tired or cold (Fitzgerald, 2010; Kliegman et al., 2011).
At 60 months:
Can skip; asks questions about the meaning of words. Can name 4 colors.
Can draw a triangle (Fitzgerald, 2010; Kliegman et al., 2011).
Between the ages of 5-6 years:
Likes teacher and knows right and left hand. Identifies best friend.
Can complete simple chores (Fitzgerald, 2010; Kliegman et al., 2011).
6 years to 12 years
At 6- 7 years old:
•
•
Can tie shoe laces, prints name. Is able to read multiple single-syllable words.
Plays well with others and can count to around 30(Fitzgerald, 2010).
At 7-8 years old:
•
Reads simple sentences. Knows the day of the week. Copies shape of diamond
(Fitzgerald, 2010).
At 8-9 years old:
•
•
Can answer simple questions. Able to add and subtract.
Understands team work and participations (Fitzgerald, 2010).
At 9-10 years old:
•
•
Know the month, date, and year.
Able to multiply and do more complex subtraction. Can read fluently (Fitzgerald, 2010).
At 10-12 years old:
•
•
•
Tanner stage 1 for girls occurs in many young girls.
Complex reading skills are attained.
Can perform simple division (Fitzgerald, 2010). Early adolescence is difficult for many due to
rapid physical growth and emotional lability (Burns et al., 2013).
13 years to 18 years- Adolescence
At 13 – 18 years old:
•
•
•
•
•
This is a time of many changes with hormonal influences. Usually stage 1 of Tanners
stages is occurring.
The psychosexual stage according to Freud is the Genital stage.
Erikson’s psychosocial stage of identity vs. role diffusion.
Piaget’s cognitive theory states that adolescents are at formal operations level with
complex reasoning skills.
Kohlberg’s moral theory is that the adolescent is in post-conventional stage with moral
principles (Burns et al., 2013; Kliegman et al., 2011).
This is a time of rapid growth:
Boys Growth {Stages Coincide with Tanner’s Growth}
· Stage 1: 5-6cm/year
· Stage 2: 5-6cm/year
· Stage 3: 7-8cm/year
· Stage 4: 10cm/year – At 13-14 years old
· Stage 5: No further height increase after 17 years
Girls Growth
Stage 1: 5-6 cm/year
Stage 2:6-7 cm/ year
Stage3:8 cm/ year – 11-12 yrs. old
Stage4: 7 cm / year
Stage 5: No further height increase
after 16 years.
(Seidel, Ball, Dains,
Flynn, Solomon, &
Sewart, 2011).
Stage 1:Prepubertal
Stage 2:Enlargement of scrotum
and testes; scrotum skin reddens
and changes in texture. Sparse
growth of long, slightly pigmented
hair
Stage 3:Enlargement of penis
(length at first); further growth of
testes. Darker, coarser and more
curled hair, spreading
Stage 4:Increased size of penis
with growth in breadth and
development of glans; testes and
scrotum larger, scrotum skin
darker. Hair adult in type, but
covering smaller area than in adult
Stage 5:Adult genitalia and hair.
Boys
Stage 1:Prepubertal
Stage 2:Breast bud stage with
elevation of breast and papilla;
enlargement of areola. Sparse
growth of long, slightly pigmented
hair
Stage 3:Further enlargement of
breast and areola; no separation of
their contour. Darker, coarser and
more curled hair that is spreading.
Stage 4:Areola and papilla form a
secondary mound above level of
breast. Hair adult in type, but
covering smaller area than in
adult.
Stage 5:Mature stage: projection of
papilla only, related to recession of
areola with adult hair pattern.
Girls
(Burns et al., 2013)
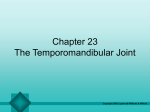
A common contagious bacterial
infection with honey colored cysts.
It requires treatment with topical
antibiotics if only superficial.
Topical treatment is usually with
polymyxin B or Mupirocin. But, with
the number of lesions that are seen
here it will require oral antibiotics
to treat the likely culprit of
Staphylococcus aureaus with
Amoxicillin/clavulate 90mg/kg/day
for 10 days or Cephalexin
40mg/kg/day for 10 days.
For the first 24 hours of treatment
it is important to keep from daycare
or other children due to being
contagious (Burns et al., 2013).
Acute Diarrhea
Discern the pattern of the diarrhea with onset, duration and
amount:
• Wet diapers in the last 24 hrs and urine vs. stool; Is dehydration present?
• Appearance with note to mucus or blood
• Other symptoms –nausea, vomiting, or abdominal pain
• Intake history of bottles and water; Eating shellfish or unpasteurized products
• Patterns of socialization; daycare, travel
• Any noted illnesses in environment
Diagnostic tests:
• Dependent on history and symptoms.
• Dependent on appearance and smell you will order
• Stool cultures x3 with pH, leukocytes, toxins (Shiga and C. Diff), Ova & Parasites.
Differential:
• Consider all systemic infections and viral and bacterial agents. Are there any
food-borne outbreaks for E. coli? Campylobacter jejuni? Listeria? Adenovirus?
Norovirus? Rotavirus? Salmonella? Shigella? And Yersina? Overfeeding in infants is
worth considering. The rarer cases involve syndromes and enzyme deficiencies or
Hirschsprung toxic colits. In adolescents, it is worth considering hyperthyroidism.
(Burns et al., 2013).
Acute Diarrhea Management
Treat according to degree of dehydration:
Minimal
• If less than 10 kg give 60-120ml of oral rehydration solution (ORS) for each
diarrheal stool or vomiting.
• More than 10 kg give 120-240ml of ORS for each stool or emesis.
Moderate
• ORS of 50-100 ml/kg over 3-4 hrs. or 10-20ml/kg/hr.
Severe
• Needs admission to hospital for IV fluids of Ringers Lactate or Normal Saline.
You want to start feedings as soon as possible to promote intestinal repair.
Prescribe antibiotics according to causative organism if bacterial systemic infection;
• C. Diff- oral metronidazole
• E. Coli (differentiate type)
• Enterohemorrhagic E. Coli- then provide supportive care.
• E. coli - TMP-SMS and quinolones
• Listeria - admit to the hospital for IV antibiotics
• Campylobacter - Erythromycin or azithromycin
Viruses need supportive care
Probiotics may be useful – Lactobacillus casei or S. boulardii decreases duration
(Burns et al., 2013).
Streptococcal Pharyngitis VS.
Other Acute Pharyngitis
Streptococcus occurs most typically in the fall, winter, and cooler part of Spring.
Incubation of the gram positive cocci is usually 7 to 10 days. It occurs less
frequently than viral pharyngitis. The most likely causative organism are
Adenoviruses, rhinoviruses, or the occasional enterovirus. However, the most common
Bacterial cause of pharyngitis is group A beta-hemolytic streptococcus (Burns et
al.,2013)
Assess for pain, fever, and associated symptoms like dysphagia.
Does any other family members have any illnesses? Duration? What has been taken?
Anything working to alleviate symptoms?
Diagnostic Test:
• A rapid strept test is very specific but has less sensitivity. Therefore, there can
Be false positives and it is important to also obtain a throat culture (Burns et al., 2013).
Treatment:
The mainstay are penicillins such as penicillin V potassium and for children less than
60 lbs. are to take 250mg 2-3x/day for 10 days with strict adherence.
Amoxicillin 50mg/kg for 10 days is an alternative, but for allergy to beta lactams
give azithromycin 12mg/kg daily to max dose of 500mg/day (Burns et al., 2013).
Bronchiolitis
It is an acute inflammation of the lower airways with edema in
infants and young children. This usually presents itself during the
months of November – April with the most prevalent organism
being respiratory syncytial virus (RSV), but other viruses are also
attributable. M. pneumoniae may be present which is bacterial.
In mild cases the symptoms may last for 1-3 days, but the course
of the virus is usually 2-3 weeks (Burns et al., 2013; Fitzgerald, 2010).
Assess: Initial presentation and onset of upper respiratory symptoms
such as cough, and coryza. Are there any adventitious lung sounds? Is
there a fever? Decreased appetitie? Did the child stop breathing? Is
there any grunting or retractions? What is the respiratory rate? Is
there any conjunctivitis? Any pharyngitis? Any other symptoms like
abdominal distention or palpable liver and spleen(Burns et al., 2013)?
Risk Factors may indicate the need for more aggressive care and
hospitalization such as; smoking in the home, low birth weight,
immunodeficiency, and daycare environments. If the child has heart
issues and is premature it is beneficial to administer Synagis or
Palivizumab before they are 24 months old. Synagis is administered
monthly from November – March at 15mg/ kg by intramuscular
injection (Lippincott Williams & Wilkins, 2014; Burns et al., 2014).
Bronchiolitis
Diagnostic tests: Pulse oximetry is the only real
recommendation (Lippincott Williams & Wilkins, 2014).
Viral culture with nasal washings and CXR maybe
warranted for the more severe cases (Burns et al.,
2013).
Treatment: The milder cases supportive care is the
most therapeutic approach such as encouraging fluids
and antipyretic therapy. The use of normal saline
drops for the nares with bulb suction are strongly
recommended as is smaller more frequent feedings.
Hospitalization is warranted if dehydration or more
severe illness is suspected (Burns et al., 2013).
Asthma
Affects 5-10% of the population and is one of the most
prevalent chronic diseases of children. It appears to be more
common in boys than girls and that reverses in adulthood.
The symptoms appear to be worse at night with bronchospasm
(Fitzgerald, 2010; Lippincott Williams & Wilkins,2014).
Assess: History of symptoms, emergency room visits and past intubations.
Such when are symptoms worse. Respiratory rate with noting the inspiration to
expiration and accessory muscle usage (Lippincott Williams & Wilkins, 2014).
Diagnostic tests: Use a peak flow meter or spirometry readings to evaluate
current status and keep record (Lippincott Williams & Wilkins, 2014).
Treatment: Is dependent on the exacerbation. Initially in an outpatient
setting, it is important to provide short-acting β-agonist (SABA) for quick relief
of acute exacerbations. Nebulizers are beneficial in the young and those with
poor technique. If the exacerbation is moderate to severe with persistence it
is important to give systemic steroids and inhaled corticosteroid therapy (ICS)
which requires consistent use (Lippincott Williams & Wilkins, 2014). There is a
stepwise management plan that varies slightly for children that are 0-4 years
old and then children from 5-11 years of age based on the National Asthma
Education and Prevention Program Expert Panel Report 3. The main
differences in treatment according to age is the use of montelukast for 0-4
year olds and the use of long acting β- agonists or leukotiene receptor agonist
for the older children (Fitzgerald,2010).
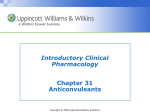
This highly contagious virus has decreased in
frequency due to vaccination, but it tends to
peak in the ages of 10-14 year olds. The
incubation period is 10-21 days and the
communicability is a couple of days before
the rash appears.
The disease can still occur after vaccination,
but the severity is greatly reduced. A mild
infection occurs in 1 out of 5 vaccinated .
Aspirin is contraindicated and the treatment
is supportive. Use oatmeal baths, calamine
lotion topical (not to be applied to children
less than 6 months) and antihistamines for
itching. For the immune compromised
intravenous acyclovir is beneficial.
(Burns et al., 2013).
Acute Otitis Media (AOM)
Inflammation of the middle ear with fluid is often
related to an upper respiratory infection. However, some children
have a greater tendency in contracting these infections. There are risk
factors associated with acute otitis media; such as genetics, premature
birth, bottle feeding while supine, daycare, smoking in home, and
being male. Having AOM before 1 year old is a risk factor for
reoccurrence (Lippincott Williams & Wilkins, 2014).
Assess: Has the child had a fever? Otorrhea? Disrupted sleep and
inability to sleep? Are there any craniofacial abnormalities? Any
diarrhea or vomiting? Any sudden hearing loss? Are there any changes in
the gait? Is there any drainage coming from the ear (Burns et al.,
2013)?
Diagnostic tests: Exam by pneumatic otoscope is the best way of
determining AOM. Tympanometry is good for assessing effusion and
typanocentesis can assist in organism identification (Burns et al.,
2013).
Antibiotics for Acute Otitis
Media(AOM)
Treatment: Pain management is the first treatment that needs to be
completed such as with benzocaine topically applied to the tympanic membrane.
For children less than 6-months-old antibacterial therapy is always given. In a
child that is older than 6 months, but less than 2-years-old is to receive antibiotic
therapy if the diagnosis is certain. If questionable watchful waiting for 48-72 hours
prior to prescribing antibiotics is a cost-effective strategy which can minimize
resistance patterns (Burns et al., 2013).
There has been much debate over the administration of antibiotics for AOM.
The antibiotic treatment is for temperature of < 102.2º with
• amoxicillin 80-90mg /kg/day for 10 days divided for every 12 hour
administration.
• Cefdinir if recommended if penicillin allergy or azithromycin
If treatment failure or fever >102.2º
• Amoxicillin-clavulante 90mg/6.4mg/ kg/ day
• Ceftriaxone intramuscularly 50 mg /kg once or in 3 consecutive doses
(Burns et al., 2013).
Attention Deficit Hyperactivity Disorder (ADHD)
This disorder consists of several subtypes:
• Hyperactive/ impulsive
• Inattentive
• Combined
The DSM-IV criteria states there must be 6-9 behaviors in inattention
and/or hyperactivity with impulsivity that persists for more than 6
months. This must also be proved to be maladaptive. An individual
education plan (IEP) must be obtained following the parental request of
the from the school.
Assess: Need to use a standardized screening form such as the Connor (Only
screens for ADHD), Vanderbilt and Child Behaviors Checklist (possible comorbidities
are assessed). Need a detailed parental, academic and developmental history of
the child. Sleep history is also important in assessment. Family history with
learning disabilities are something to consider. Was the child premature, have any
(Acute life threatening events) ALTES, or lead exposure?
• Diagnostic tests:
•
•
•
CBC for anemia
Thyroid function tests (TSH, FT4 – or "free thyroxine" – levels)
Blood lead level
(Lippincott Williams & Wilkins, 2014).
First line treatment consists of stimulants:
Methylphenidate, dextroamphetamine,and amphetamine.
Second line is Atomoxetine and other psychotropic
medications
Follow-up is important and the use of a multidisciplinary
team of developmental pediatrics, psychologists, neurologists
and psychiatrists for assessment and treatment.
Monitor height, weight, B/P,and heart rate.
Monitor performances at school, with peers and at home.
Resources for parents are at www.chadd.org
and www.add.about.com
(Lippincott Williams & Wilkins, 2014).
Kawasaki Disease
It is a multisystem disease that presents usually with skin
eruptions initially in the genital area and a high fever.
It is referred to as an acute systemic vasculitis. Oral changes
occur and then desquamation of the areas most involved such as
perineum, hands, feet (Burns et al., 2013; Lippincott Williams &
Wilkins, 2014).
Edema and erythema of the feet is the most complained about issue
and without treatment coronary artery aneurysm may occur. There is
unilateral adenopathy, conjunctivitis and generalized inflammation
associated with the rash (Lippincott Williams & Wilkins, 2014).
Diagnostic tests: CBC with differential, ESR, Chest x-ray and
echocardiography are the most important tests. Serial EKGs are done
at first evaluation, then 2 weeks, 6 weeks and at 8 weeks.
Angiography, MRI, and cardiac stress testing may be considered (Burns
et al., 2013; Lippincott Williams & Wilkins, 2014).
Treatment: The main treatment is the administration of Intravenous
immunoglobulin G (IVIG) at 2 g/ kg along over 10- 12 hours with aspirin
in high doses (Burns et al., 2013; Lippincott Williams & Wilkins, 2014).
Autism Spectrum Disorders
It is a set of neurodevelopmental disorders that are characterized by impaired
social skills, impaired communications skills, and repetitive behaviors . There
also appears to be an interest in inanimate objects (Lippincott Williams &
Wilkins, 2014). It occurs more in males and in approximately in once out of
every 100-500 children (Lippincott Williams & Wilkins, 2014).
Assess: Social skills and activities for developmental screening by an (ages and
stages questionnaire) ASQ-3 at stages 9,18, and 24 months. The earlier the
better in Kentucky because the cut-off for getting the child in first steps is at 36
months. The modified checklist for autism in toddlers(MCHAT )may also be used
at 15 and 20 months. Developmental surveillance occurs at all visits and if
needed the child is referred for other intervention such as child specialists
(Myers, 2014). Red flags are not knowing name by 1 year old and avoiding eye
contact (Burns et al., 2013). Is there any macrocephaly in 25% range? Are there
any dysmorphic features? Is there any hypotonia (Lippincott, Williams & Wilkins,
2014).
Diagnostic tests: Lead screening at 12 months, PKU screening , Karyotype and
DNA analysis. Metabolic testing if lethargy, hypotonia, developmental regression
or unusual habits.
Autism Spectrum Disorders -Treatment
Treatment: It is important to have follow-up testing such as with the
Autism Behavior Checklist. Comprehensive speech and language
evaluation with a speech therapist. Having a multidisciplinary team
such as psychiatry, neurology, and other autism specialists
(Lippincott, Williams & Wilkins, 2014).
Early intervention is the best medication.
Then you might consider medications if needed. Stimulants, and SSRIs
Risperidone may be beneficial for irritability and social withdrawal for
a short period (Lippincott, Williams & Wilkins, 2014).
The Autism toolkit and patient handout “Understanding Autism Spectrum
Disorders (ASD)” available at www.aap.org
www.autismdigest.com
www.autism-society.org
www.cdc.gov/ncbddd/autism/index.html
www.cdc.gov/ncbddd/autism/hcp-recommendations.html
Conjunctivitis
There are multiple causes of conjunctivitis and a good examination
with follow-up is important in the proper care of conjunctivitis.
Noting the age of the child and the associated factors surrounding
the complaints are worthy of investigation.
Assess: Pain? Discharge? Photophobia? Matted eyelids? Petechiae or bulbar
conjuctiva? Wears contacts? Vision changes? Upper respiratory infection?
Fever? Headache? Allergies? Itching?
Diagnostic tests: If there are vision changes the child must be referred to an
opthalmologist for a slit lamp and further intensive examination.
If the infection is in a neonate you need to gram stain the discharge for
possible chlamydia (Lippincott, Williams & Wilkins, 2014).
Treatment: If bacterial treatment depends on the causative organism.
Gonococcus- Ceftriaxone by IV and 1% tetracycline ophthalmic
ointment QID for 14 days
Chlamydia- oral erythromycin syrup 12.5mg/kg/day QID for 14 days with
0.5% erythromycin or 1% tetracycline ophthalmic ointment
Other Bacteria- empiric therapy and polymyxin B ophthalmic solution QID or
levofloxacin 0.5% ophthalmic solution QID or even above therapies
for ointments(Lippincott, Williams & Wilkins, 2014).
Conjunctivitis - Treatment
Treatment:
depends on the causative organism
Gonococcus- Ceftriaxone by IV and 1% tetracycline ophthalmic
ointment QID for 14 days
Chlamydia- oral erythromycin syrup 12.5mg/kg/day QID for 14 days with
0.5% erythromycin or 1% tetracycline ophthalmic ointment
Other Bacteria- empiric therapy and polymyxin B ophthalmic solution QID
or levofloxacin 0.5% ophthalmic solution QID or even above
therapies for ointments(Lippincott, Williams & Wilkins, 2014).
Herpes Simplex- Topical trifluorothymidine (viroptic) 9 times daily for at
least 14 days with or without systemic acyclovir.
Follow- up cannot be stressed enough and daily monitoring with Gonoccus,
Chlamydia, and herpes simplex.
If the causative organism is not know it is important for the patient to
follow-up with an ophthalmologist if any vision changes occur (Lippincott,
Williams, & Wilkins, 2014).
If concerned for infection such as “pink eye” then restrict daycare and
socialization for 48 hours (Burns et al., 2013).
Enuresis
The peak incidence is 5-10 years old and the percentages of
male and females decrease with age generally. Approximately
75% of children had a first degree relative with this issue and it
is almost twice as common in monozygotic twins (Ferri, 2014).
Assess: When does it occur? Is it only at night? Is there a
particular time in the night? Are there any other physical issues?
Any constipation issues? What does the diet consist of? Does
diabetes run in the family? What medications does the child
take? What is the night time routine?
Perform a careful physical exam for possible infection or
stricture. Look and palpate for masses. A neurological exam to
determine if any neurological issues and funduscopic exam for
evaluating for increased intracranial pressure. Any spinal
defects? (Lippincott, Williams, & Wilkins, 2014).
Diagnostic tests: Urinalysis is the most important
test (preferably first morning void) with
evaluation for specific gravity, glucose, protein,
blood. If there is concern for anatomic function
problem then a renal ultrasound could be
performed with referral to urologist (Lippincott,
Williams, & Wilkins, 2014).
Treatment: Cognitive behavioral rewards and positive
reinforcement for dry nights if primary nocturnal
enuresis. Bell and pad alarm systems are useful as an
intervention. Mostly watchful waiting until the child
is older. If the child is around 6-8 years old and
the issue continues may reassess the situation
and see if desmopressin is needed (Ferri,2014;
Lippincott, Williams, & Wilkins, 2014).
Common sleep disorders
Children need to learn how to sleep and at about 6 months you can start
applying the conditioning training that Dr. T. Wolynn recommends at
www.kidspluspgh.com where you can obtain a great handout.
Assess: Are there any physical problems such as: ear infections
• Neurological disorders
*Hypothyroidism
• Obesity
* Pain
• Tonsil and adenoid hypertrophy *Blindness
• Orofacial anomalies
*Asthma
• Genetic disorders
*Chronic diseases
• Stress
*Autism
• ADHD
* Developmental stage (Burns et al., 2013).
Is the child in daycare? Medications? Sleep regimen? What time does sleep
occur? Is there consistency? The assessment should be varied as with the
age of the child and their problems. The tables on pages
264-265 (Burns et al, 2013).
Treatment:
The interventions are on page
265, but referral to a sleep neurologist
maybe necessary with obstructive sleep
apnea or parasomnias. If bruxism,
recommend a bite block from the sports
section of a store and dental referral
(Burns et al., 2013).
Diabetes Mellitus Type I and Type II
Type 1 is caused by an autoimmune destruction of the islets of
Langerhans
In the pancreas. Type II is related to impaired glucose tolerance and
insulin
resistance. Both diseases create a state of hyperglycemia. DM type II
is most
associated with African Americans, Latinos, and Native Americans
with a family history. The incidence of DM type II is increasing
rapidly in teenagers
(Lippincott, Williams, & Wilkins, 2014).
Assess: Polyuria, nocturia, and enuresis are issues that are common.
• Polyphagia
*Weight loss
• *Dehydration
* Fatigue
• Nausea and vomiting *Lethargy due to ketosis/ acidosis
• Candidal vaginitis
* In Ketosis –hyperventilation, and
dehydration
• Obesity for type II
* Acanthosis nigricans for type II
Diabetes Mellitus Type I and
Type II
Diagnostics:
• Blood glucose (BG) level that is greater than 126 as a fasting level or
2 hour BG > 200mg/dL
• Glucosuria or ketonuria *TSH and Free T4
Treatment: diet with a restriction in carbohydrates 55% with dietician
• Fats 30%
* Proteins 15% with insulin regimens spaced
carefully
• Weight loss for type II DM and metformin are the primary treatment
measures
• Routine doctor visits with urinalysis, Hgb A1C measure for
evaluation
• Annual ophthalmologist appointment
(Burns et al, 2013; Lippincott, Williams, & Wilkins, 2014).
Acquired Hypothyroidism in children
The most common cause of acquired hypothyroidism is Hashimoto thyroiditis
(Burns et al., 2013). Some genetic syndromes are associated such as Down and
Turner syndrome.
Assess:
• Goiter
• Pernicious Anemia
• Growth (shortened stature)
• Diabetes history
• Myxedema
• Delayed puberty
* Vitiligo
*Bradycardia and thyroid bruit
* Decreased school performance
* Radiation exposure
* Muscle hypertrophy
* Precocious puberty and galactorrhea
Diagnostics:
T4 (low) and elevated TSH If the TSH is elevated and the T4 is normal the thyroid
Is compensating
• Antithyroglobulin and antimicrosomal antibodies
• Serum creatinine (elevated)
• LDL cholesterol (elevated)
• Creatinine kinase (elevated)
• MRI for evaluation of secondary cause such as pituitary tumor
Treatment:
• Primary treatment is with various forms of synthetic thyroid
hormone at 2-5 mcg/Kg/day for lifetime treatment (Burns
et al., 2013; Lippincott, Williams, & Wilkins, 2014).
Interpreters for foreign languages and communication
with families
Make
a complete statement for the
interpreter to interpret. Do not make too
many statements or things are lost in
translation. A translator is imperative with
working with multiple nationalities. There
are many lawsuits related to this and missed
issues such as in my case study. If you feel
the translator is not translating correctly, you
can and need to obtain another translator.
http://www.pacificinterpreters.com/docs/resources/high-costs-of-language-barriers-inmalpractice_nhelp.pdf
This PDF presents 32 cases of litigation that were due to lack of the
use of interpreters. You risk litigation without interpreters.
Assessment of 1-2 year olds
Demonstrate
on yourself, then
parent, and finally the patient all
methods of assessment. Make the
assessment like play and smile and
giggle at child to calm the child.
Children can tell by tone what is
going on. Keep things light and keep
a quiet hushed tone so that children
will be more intent on what is said
than what is being done.
Assessment of Toddlers to Preschoolers (2-5 years old)
Play
with the child. Make the
assessment a play experience. “Can
I see whether you have a puppy in
your ear?” The musculoskeletal
assessment can be done by using
Simon Says or an imitation game and
this should be done last due to the
fact that laughter can get loud.
Assessment of school age children 5-11 year olds
When
the child is younger play, but
if the child’s affect is very stiff or
appears ill be quiet and allow for a
more gentle approach.
Always show care and affection by
expression and occasional hugs.
Reward good behavior in younger
children by stickers or applause.
Assessment of Teenagers
Make
sure that you approach the teenager
as a person that wants the best for them.
Make sure that confidentiality is foremost
in their care. Make sure that you assess
some knowledge about sexuality and
mental health without the parent present.
Ask about everything such as friends,
relationships, and concerns at home. If you
do not ask, the teenager will not tell.
Sometimes, they still will not tell about
their concerns.
Assessment of Hispanics
It
is important be polite and
appreciative of their beliefs and
expect that they will use alternative
medicines.
Nodding of the head does not
necessarily mean understanding and
that it could signify respect.
Having interpreters from Cuba for
Cubans is better since the cultural
variations can be significant in regards
to healthcare.
Assessment of Nepali and other refugees
There
is a large population of Nepali
refugees in Louisville. These refugees
use many home remedies before seeing
a physician.
The refugees from all countries go to
various clinics, but there is no
communication between clinics and
you must ask about the TB clinic and
follow up appointments when you
have the assistance of the Nepali
interpreter.
Assessment of Somali children
All
Somali’s are Muslim and practice halal
dietary restrictions and may prefer to take
Soy formulas. This is the reason why they
will not take any other formula if they are
not breast feeding.
Halal is a strict form of dietary restriction,
but it is not as strict as a Jewish Kosher
diet. However, there are some concerns for
commercialism and preparations that are
not according to the Muslim lifestyle.
Assessment with Down’s Syndrome and Noonan’s
Syndrome
They
have a separate growth chart and
their expected growth is to have a
shorter stature.
Noonan Syndrome also has a different
growth chart for short growth stature
expectations.
These syndromes require a
multidisciplinary care approach and
you need to make sure that the
appointments with the other practices
are being kept.
Assessment of ears in a young child
Play
with the otoscope with the
young child by showing them that
the light shines on your hand and
then take the light and shine it on
the parent. Take the light and shine
it on the child and explain to parent
and child that it is important to be
still while I look for a culturally
appropriate cartoon or toy.
How to get a toddler to open their mouth
You
can play a little game of Simon
says or you can have the parent pinch
the child’s nose and release. If that
does not work then you can see if the
child will mimic you or you can get the
“popsickle stick” tongue blade and use
it for holding the mouth open. If they
do then you can play another game and
the musculoskeletal movement game is
something that you can do.
How to get a older toddler to take a deep breath
You
can take a glove and have the child try
to blow it up while you auscultate (best for 4
years old and up).
Another method is the taking a pen light and
have them blow it out (best for over 15
months).
Also you can the younger child be
held by the parent and if the parents
hair is long enough have the child blow
the hair out of their face (can be used
at any age).
The Harriet Lane handbook
has sections that discuss
genetic abnormalities, and
shows radiologic images along
with dermatology images
in the pediatric client. It
can help in differentiating the
diagnosis. Available in iOS and
Android.
http://www.unboundmedicine.com/products/harriet_lane_handbook
The application is available for
android and iOS. It lists
professional local lactation
consultants and pediatricians that
can help with breast feeding issues.
The application is free, but if you
use the
latchCHAT you will have to pay a
small fee. This can be real
beneficial so that you know who you
are talking to and helps find support
fast.
https://itunes.apple.com/us/app/latchme-breastfeeding.../id813106754?mt;
https://play.google.com/store/apps/details?id=com.latchme.app&hl=e
This helps in making sure that the child
that is new to eating is getting a
diversified diet and if the child is
suffering from neophobia it really can be
beneficial. The application is available
on iOS. The application developers also
have an application for healthy kids
exercises.
http://www.apppicker.com/apps/421514147/a-parents-app-for-healthykids--ifeed-lite
In the latest issue is the
“Best practices in developmental
Screening and referral for young
children”, by L. Myers.
This application can help you
access many online articles that
will help your practice. The
articles do not necessarily
pertain to children, but several
often do. This application is on iOS.
It specifically tells what
formulas to use to supplement
breastfeeding if needed and the
amount. It also specifies the
amount of growth and the
caloric content of many of the
commercial formulas for
infants. It is an online kit and
information.
https://www.preemietoolkit.com/pdfs/E_PhysicalExaminationAssessment/Recom
mendations-for-Postdischarge.pdf
https://www.preemietoolkit.com/images/outpatient_roll.jpg
The Newborn screening guide is
available for the state of Kentucky,
but every state has their own
practice. The screening guide
presents who to report to and what
the necessary information for
diseases and codes.
Kentucky: Cabinet for Health and Family
Services - Newborn Screeningchfs.ky.gov
Healthy Children application is
available for android and iOS.
You can customize the top row
with preferences, but this app
contains many subjects on
healthy ages and stages,
nutrition, fitness, and family
life.
Healthychildren.org
This application is developed by
the Northern California Training
academy it is by andromo and is
available on android developed
on 2013.
Child Development Milestones - Android Apps on Google
Playplay.google.com
Percentiles
Body Mass Index for Child and Teen
These are two applications that I
will resort to if Epocrates does not
work for evaluating BMI. I prefer
the online format because you can
list specialty calculators and use
the pediatrics section easily.
Precentiles is available on Google
Play for android by R. R. R.
Fernandez M. D.
The CDC app is available in iOS and
android versions by visiting the
CDC website at
http:nccd.cdc.gov/dnpabmi/Calculator.aspx
Percentiles App for Androidwww.appszoom.com ;
www.epocrates.com ;
http://nccd.cdc.gov/dnpabmi/Calculator.aspx
Baby center has the My Baby
Today app. This application
is sponsored by Johnsons and
Johnson with videos and all
kinds of information that is
important and relevant to
the child/parent at the time.
It is available for android or
iOS.
www.babycenter.com/my-baby-today-app
This application is the
vaccination schedules and all
of the information on catch
up schedules and various
issues that can occur with
catching up. All of the
information on the various
resources on the
administration of
vaccinations.
http://www.cdc.gov/vaccines/schedules/hcp/schedule-app.html
References
Burns, C. E., Dunn, A. M., Brady, M. A., Starr, N. B., & Blosser, C. G. (2013).
Pediatric primary care (5th ed.). Philadelphia, PA: Elsevier – Saunders.
Centers for Disease Control (2014). 2014 Recommended immunization schedule
for persons aged 0 through 18 years. Retrieved at
http://www.cdc.gov/vaccines/scheduels/dowloads/child/0-18yrs-schedule.pdf
Centers for Disease (2014). 2014 Catch-up immunization schedule. Retrieved at
http://www.cdc.gov/vaccines/schedules/downloads/child/catchup-schedulepr.pdf
Ferri, F.F. (2014). Ferri's clinical advisor 2014: 5 books in 1. Philadelphia, PA:
Mosby Elsevier.
Fitzgerald, M. (2010). Nurse practitioner certification examination and practice
preparation. Philadelphia, PA: F. A. Davis Company.
References
Kliegman, R. M., Stanton, B. F., St. Geme, J.W., Schor, N. F., & Behrman, R. E.
(2011). Nelson Textbook of Pediatrics (19th Ed.). Philadelphia, PA: Elsevier –
Saunders.
Lippincott Williams & Wilkins. (2014). Five-minute pediatric clinical consult.
Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins.
Myers, L. (2014). Best practices in developmental screening and referral for young
children. The Nurse Practitioner Journal, 39(12). Retrieved from
www.tnpj.com
Seidel, H. M., Ball, J. W., Dains, J. E., Flynn, J.A., Solomon, B.S., & Stewart,
R. W. (2011). Mosby's Guide to Physical Examination. St. Louis,
MO: Mosby Elsevier.