Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
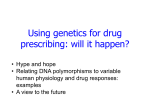
Pharmacological Reports Copyright © 2013 2013, 65, 187194 by Institute of Pharmacology ISSN 1734-1140 Polish Academy of Sciences Variability in CYP2C9 allele frequency: A pilot study of its predicted impact on warfarin response among healthy South and North Indians Risha Nahar1,2, Roumi Deb2, Renu Saxena1, Ratna Dua Puri1, Ishwar Chander Verma1 1 Centre of Medical Genetics, Sir Ganga Ram Hospital, Rajinder Nagar - 110060, New Delhi, India 2 Amity Institute of Biotechnology, Amity University, Sector-125, Noida - 201301, Uttar Pradesh, India Correspondence: Risha Nahar, e-mail: [email protected] Abstract: Background: Wide variability exists in the frequency of pharmacogenetic markers for anticoagulant response in different populations. There is insufficient data on the prevalence of these variant genotypes in the Indian population. This study aims to determine the frequency of various genotype combinations of CYP2C9*2, *3 and VKORC1-1639G>A polymorphisms in the South and North Indians. Methods: Genotyping was carried out by PCR-RFLP (polymerase chain reaction-restriction fragment length polymorphism) technique in 209 North Indians (NI) and 82 South Indians (SI). Warfarin maintenance dose was predicted for all subjects based on FDA approved genotype-based dose estimates from revised COUMADIN medication guide. Fisher exact test and c2 test were applied to compare categorical data among the SI and NI groups. Results: In SI and NI, the allele frequency of CYP2C9*2 was 0.006 and 0.05 (significant variation; p < 0.001); of CYP2C9*3 was 0.09 and 0.11; and of VKORC1-1639A was 0.14 and 0.19 (not significant), respectively. The variation in the frequency of combined CYP2C9/ VKORC1 genotypes revealed plausible difference in warfarin response among SI and NI. Based on the FDA approved revised dosing guidelines, significantly higher percentage of NI were likely to require intermediate dose (3–4 mg/day; p = 0.015, RR = 2.16) and were also predicted to have an increased risk of bleeding episodes and over anticoagulation (p = 0.012, RR = 1.93). Conclusions: Genotype frequency of CYP2C9 and VKORC1 SNPs is variable among the two ethno-geographically distinct Indian populations. This could translate into diverse warfarin response among the Indian population. Key words: warfarin, acenocoumarol, India, thrombosis, drug response, adverse effects, CYP2C9, VKORC1 Abbreviations: CYP2C9 – cytochrome P450 subfamily IIC polypeptide 9, NI – North Indians, SI – South Indians, SNP – single nucleotide polymorphism, VKORC1 – vitamin K epoxide reductase complex, subunit 1 Introduction Coumarin anticoagulant drugs are used in the treatment and prophylaxis of venous and arterial thromboembolic events; warfarin (Coumadin) being the most widely prescribed worldwide. Acenocoumarol and phenprocoumon are administered in Europe [3] while in India, acenocoumarol (Acitrom) and warfarin are the most commonly prescribed. The widespread use of these drugs is limited by the wide interindividual variability (20 fold) in the dose required to achieve therapeutic anticoagulation [24]. Current dosage protocols (based on demographic or clinical information) run the risk of severe bleeding and hemorrhage (when on higher dose) or slow and inadequate anticoagulation (when on lower dose). Pharmacological Reports, 2013, 65, 167194 187 Warfarin and acenocoumarol are metabolized primarily in the liver by cytochrome P-450 2C9 enzyme (encoded by CYP2C9), and exert their anticoagulant effect by inhibiting vitamin K epoxide reductase complex, subunit 1 protein (encoded by VKORC1). In western countries, pharmacogenomic studies on these two genes have clearly shown their value in individualizing treatment. These have helped the physicians to reduce the risk of bleeding and hemorrhage without compromising the effectiveness of therapy [26]. Indeed, in year 2007, the US Food and Drug Administration (FDA) considered evidence of the benefits of genotyping to be sufficiently strong for it to revise warfarin label in year 2007, recommending lowering of initial doses in patients having the CYP2C9 *2 or *3 or VKORC1-1639G>A alleles [8]. In 2010, the Coumadin® label was revised again with specific pharmacogenetic guided dosing ranges derived from multiple published clinical studies [6]. In 2006, Takahashi et al. [22] showed that the dosing requirement for a similar intensity of anticoagulation varies across different populations. Asians (Chinese, Japanese, Malays) were reported to require lower maintenance dose than Caucasians and Indians, while African Americans require higher dose [22]. Before introducing pharmacogenetic-based dosing of coumarin anticoagulants in Indians, it would be useful to determine the prevalence of the different genotype combinations of CYP2C9 (*2, *3) and VKORC1 (-1639G>A) in the South and North Indian population. The people of Northern India are known to be descendents of Aryans (Indo-European-speaking group) while the South Indian population are considered to be the Dravidian ethnic group [2]. Dermatoglyphic and genomic marker studies have confirmed the diversity between these two ethnogeographical Indian ethnic populations [2, 17]. This study was aimed to identify and compare the proportion of South and North Indians who are carriers of variant CYP2C9 and VKORC1 polymorphisms. As this is a pilot study in health subjects, a more systematic prospective study including larger cohort of patients with well defined clinical and extended candidate gene-SNP panel are needed to get a finer picture of variability in warfarin response among South and North Indians. Materials and Methods The study was carried out at the Centre of Medical Genetics, Sir Ganga Ram Hospital, New Delhi, India. 188 Pharmacological Reports, 2013, 65, 187194 The study protocol was approved by the hospital’s Ethics Review Board and is in accordance with the ethical guidelines for biomedical research on human participants (Indian Council of Medical Research). Study population Healthy volunteers (n = 291) were recruited from a period of February to November 2011. The ‘healthy’ status was based on the information they had provided themselves during their visit to the genetic clinic for routine antenatal screening. Prospective organ donors who visited the clinic for HLA matching tests were assumed to be healthy. Of these, 209 (102 males; 107 females) belonged to the Northern states of India [Punjab (n = 65), Haryana (n = 38), Uttar Pradesh (n = 35), New Delhi (n = 40), Uttarakhand (n = 31) – IndoAryan ethnic group] and 82 (40 males; 42 females) were from Southern India [Tamil Nadu (n = 25), Andhra Pradesh (n = 32), Kerala (n = 25) – Dravidian ethnic group]. The study was planned with a 5% precision level (95% confidence interval) and sample sizes were calculated accordingly. Ethnicity was established by inquiring about the individuals’ maternal and paternal grand-parental place of origin and language. Informed consent was obtained from all subjects prior to their inclusion in the study. DNA extraction DNA was isolated from two ml of whole blood (with EDTA as anticoagulant) using standard salt-extraction method [14] and stored at 4°C prior to genotyping analysis. The DNA purity and quantity was measured using UV visible spectrophotometer (NanoDrop 2000, Thermo Scientific, USA). Genotyping of CYP2C9*2 (430C>T); *3 (1075A>C) and VKORC1-1639G>A polymorphisms Polymerase chain reaction (PCR) followed by restriction fragment length polymorphism (RFLP) was used for genotyping VKORC1–1639G>A, CYP2C9*2 and CYP2C9*3 as described previously [7, 21]. Amplification of DNA samples was carried out by three separate PCR reactions, each with 20 picomoles of the specific primer pair, 0.1 mM dNTP, 100 to 200 ng genomic DNA, 0.6 U of Taq DNA polymerase (Genei) in 10 mM Tris–HCl (pH 9.0), 1.5 mM MgCl2, 50 µM KCl. PCR amplification was accomplished with Predicted coumarin response in healthy Indians Risha Nahar et al. Fig. 1. (i) Agarose gel band pattern for VKORC1-1639A: The variant abolishes Mspl restriction site. Lane 1 is the undigested PCR product. Lanes 3 and 7 show heterozygosity (AG) while lanes 2, 4, 5 and 6 show pattern of the wild type genotype (GG). (ii) Agarose gel band pattern for CYP2C9*2 (430T): The variant abolishes AvaII restriction site. Lane 1 is the undigested PCR product. Lanes 2, 3, 4 and 6 show homozygosity for the wild type genotype (CC) while lanes 5, 7 and 8 are heterozygous for the polymorphism (CT). (iii) Polyacrylamide gel band pattern for CYP2C9*3 (1075C): The variant abolishes NsiI restriction site: Lane 1 is the undigested PCR product. Lanes 3, 4 and 13 show heterozygosity (AC) while the rest show the wild type genotype (AA) 4 min of initial denaturation at 94°C; followed by 30 cycles of 94°C, 60°C, and 72°C for 1 min each and a final extension at 72°C for 7 min. Controls of known genotype as well as no template controls were included in each batch of PCR. Restriction fragment size analysis was performed. The Nsi1 digested products were then separated on 10% polyacrylamide gel followed by silver staining while the AvaII and MspI digested products were separated on 2% agarose and visualized by ethidium bromide staining. The resulting band patterns for the restriction fragment analysis for the three SNPs are illustrated in Figure 1. The genotyping results were validated by gene resequencing. Since the cleavage recognition site for NsiI restriction enzyme used for detection of CYP2C9*3 (1075A>C) may be affected by the presence of CYP2C9*4 (1076T>C), 50 samples observed to be heterozygous or homozygous for the *3 variant were resequenced to detect *4 variant in these samples. Although other variants of VKORC1 and CYP2C9 may be present, the alleles tested in the current study are the most important for determining dose requirement and are the only valid biomarkers for warfarin sensitivity and dosing considered by the FDA. Prediction of warfarin response based on FDA approved dose estimates and recommendations Based on the 2010 revised Coumadin dosing recommendations with pharmacogenetic data [6], the expected warfarin maintenance dose range was esti- mated independently in the two ethno-geographic groups in the present study. The FDA approved classification of genotype-guided warfarin dose estimates have been “derived from multiple published clinical studies” and are as given below; s with *1/*1, AA; *1/*3, GG; *1/*3, AG; *1/*2, AG; *1/*2, AA; *2/*2, GG; *2/*2, AG and *2/*3, GG are recommended 3.0 to 4.0 mg/day and those with genotypes *1/*1, GG; *1/*1, AG and *1/*2, GG have been suggested a higher dose range of 5.0 to 7.0 mg/day. The revised dosing recommendations also highlight the prolonged time to achieve therapeutic INR effect for a given dosage regimen in carriers of CYP2C9 *1/*3, *2/*2, *2/*3, and *3/*3 as compared to non-carriers of the above CYP2C9 genotypes (*1/*1; *1/*2). The guidelines, based on several published studies, also emphasize the increased risk of over anticoagulation (INR>3) or bleeding in CYP2C9 *2 and *3 carriers [6]. Statistical analysis Genotype frequencies were checked for HardyWeinberg equilibrium using c2 test. Fisher exact probability test and c2 test (with Yates correction) were applied to compare categorical data among the SI and NI groups. Relative risks were calculated where applicable. All statistical analysis was done using the SPSS package (version 15.0). A p value < 0.05 was considered to be statistically significant. Pharmacological Reports, 2013, 65, 167194 189 Results Tab. 1. Comparison of CYP2C9 and VKORC1 genotype and allele frequencies in the study cohorts South Indians (SI, n = 82) The subjects were of the age range 19 to 43 years (mean age = 28 ± 8.8 years). The genotype and allele frequencies of CYP2C9 (*1, *2, *3) and VKORC11639G>A in the South and North Indian population are shown in Table 1. The genotypic frequencies were found to be in Hardy-Weinberg equilibrium (p = 0.1). The allele and genotype frequency did not differ significantly within subjects of different states within North India or South India and hence these are represented as two groups; the North Indians and South Indians, respectively. Genotype$ frequencies n (%) CYP2C9 (430C>T, 1075A>C) *1/*1 69 (84.1) P *1/*2 1 (1.2) *1/*3 9 (11) *2/*3 0 *3/*3 3 (3.7) Among the SI and NI, no significant difference was observed in the VKORC1-1639 A minor allele frequency (Tab. 1) and neither in the percent of carriers of the polymorphism (AA and GA; 28.1% vs. 35.9% in SI and NI, respectively). Predicted warfarin response based on combined CYP2C9 and VKORC1 genotypes The majority of both North and South Indians were envisaged to require higher (5–7 mg/day) warfarin maintenance dose to achieve therapeutic anticoagulation [74.6% (156), 85.4% (70), respectively] due to the overall high prevalence of CYP2C9 *1/*1 and 190 Pharmacological Reports, 2013, 65, 187194 145 (69.4) 20 (9.6) 42 (20) 2 (1) P 0 GG 59 (71.9) 134 (64.1) GA 23 (28.1) 72 (34.4) 0 3 (1.4) AA VKORC1 allele and genotypes P VKORC1-1639G>A CYP2C9 allele and genotypes The CYP2C9*2 allele frequency showed highly significant variation in the SI and NI (p = 0.007). Five CYP2C9 genotypes were detected in these two cohorts (*1/*1, *1/*2, *1/*3, *2/*3, *3/*3). Of these, genotypes *1/*1 and *3/*3 were observed to be in significantly higher frequency in the SI (n = 82) as compared to NI (n = 209; p = 0.01 and 0.02, respectively). Conversely, the SI had a much lower frequency of *1/*2 genotype as compared to the NI (p = 0.01). A total of 26.5% were carriers of the *2 and/or *3 variant alleles with significant deviation in frequency observed between the SI and NI groups (15.9 vs. 30.6%, respectively; p = 0.01). Resequencing of the 50 DNA samples with observed *3 variant (genotyped using NsiI digestion) did not reveal presence of *4 allele in any sample. North Indians (NI, n = 209) $$ Allele frequencies CYP2C9*1 0.9 0.84 CYP2C9*2 0.006 P 0.05 CYP2C9*3 0.09 0.11 VKORC1-1639G 0.86 0.81 VKORC1-1639A 0.14 0.19 $ Genotype *1/*1 = 430CC/1075AA; *1/*2 = 430CT/1075AA; *1/*3 = 430CC/1075AC; *2/*2 = 430TT/1075AA; *2/*3 = 430CT/1075AC; *3/*3 = 430CC/1075CC, CYP2C9 *1 is the wild type allele and refers to CYP2C9 alleles other than *2 and *3. P Statistically significant (p value < 0.05) variation in frequency between SI and NI, $$ Allele *1 = 430C/1075A; *2 = 430T; *3 = 1075C VKORC1 GG wild-type genotypes. The percentage of NI likely to require intermediate (3–4 mg/day) dose was significantly greater than that of SI [24.4% (51) vs. 11% (9), respectively; p = 0.015, relative risk (RR) = 2.16; 95% confidence interval (CI) = 1.12–4.18]. The subjects who were likely to require low dose (0.5–2.0 mg/day) formed the minority group [0.9% (2) NI and 3.6% (3) SI] showing no significant variation. Also, considerably larger proportion of NI were genetically predisposed to warfarin-induced bleeding episodes or over anticoagulation (INR > 3) due to increased frequency of CYP2C9*2 and *3 variants as compared to SI [30.6% (64) vs. 15.9% (13), respectively; p = 0.012; RR = 1.93; 95% CI = 1.13–3.31]. Prolonged time to achieve stable therapeutic INRs was expected in 14.6% (12) of South Indians and 21% (44) of North Indians with no significant deviation (p = 0.249). Predicted coumarin response in healthy Indians Risha Nahar et al. Tab. 2. Allele frequency of the three SNPs in different world-wide populations Ethnic Population Reference study Caucasian Takahashi et al. 2006 Swedish Yasar et al. 1999 (i); Wadelius et al. 2007 (ii) French Yang et al. 2003 (i); Bodin et al. 2005 (ii) Netherlands Schalekamp et al. 2004 (i); 2006 (ii) n CYP2C9*2 (%) CYP2C9*3 (%) VKORC1-1639A (%) 115 14.3 10.9 42.2 430 (i), 181 (ii) 10.7 7.4 39 151 (i); 222 (ii) 15 8.0 42 231 (i & ii) 16.5 19.9 64.9 Greek Markatos et al. 2008 98 15.5 7.5 48.5 German Burian et al. 2002 (i); Geisen et al. 2005 (ii) 118 (i); 200 (ii) 14 5.0 42 Russian Gaikovitch et al. 2003 290 10.5 6.7 NA Japanese Takahashi et al. 2006 64 0 1.6 89.1 Chinese Yang et al. 2003 (i); Yuan et al. 2005 (ii) 394 (i); 104 (ii) 0.1 3.6 91 Korean Yoon et al. 2001 574 0 1.1 NA Takahashi et al. 2006 66 0 0.8 8.6 African-American $ Lee et al. 2006 43 4 18 NA South India$$ Jose et al. 2004 346 4 8 NA South India$$$ Adithan et al. 2003 135 2.6 6.7 NA Indians # Rathore et al. 2010 102 4.9 3.92 14.22 South Indians (SI) Present study 82 0.6 9 14 North Indians (NI) Present study 209 5 11 19 Total cohort (SI + NI) Present study 291 4 10 17 North India NA = Not available; CYP2C9*2 (430C>T; rs1799853); CYP2C9*3 (1075A>C; rs1057910); VKORC1 -1639G>A (G3673A; rs9923231); $ from Singapore); $$ from states of Andhra Pradesh, Karnataka or Kerala; $$$ only from Tamil Nadu state; # mainly from Uttar Pradesh state Discussion The present study has analyzed genotypes of three SNPs in a total of 582 chromosomes (n = 291) of which 164 chromosomes (n = 82) were of individuals of SI (Dravidian ethnic origin) and 418 of NI origin (n = 209). This study is the largest of its kind in the Indian subcontinent to compare the genotype-based predicted warfarin response in two ethno-geographically distinct groups in India. The current study, reports the allele and genotype frequency of VKORC1-1639G>A SNP in the SI population and reports no significant difference from that in NI. However, the VKORC11639 minor allele frequency in the current population was observed to be smaller in contrast to Caucasians [22], and other world populations [4, 10, 19, 20, 25, 27, 28] except the African Americans [22] (Tab. 2). The CYP2C9*2 allele frequency was observed to be significantly different between the SI and NI groups. More specifically, the relatively smaller *2 allele frequency in SI was similar to that reported in other Asian populations (Japanese [22], Chinese [27, 30] and Korean [29]) and African Americans [22], while the *2 allele frequency in NI is similar to the Caucasians [22] and Russians [9]. In two other studies in Southern India, the CYP2C9*2 allele occurred with a frequency of 2.6% (includes subjects originating from Tamil Nadu) [1] and 4% (includes subjects from Kerala, Andhra Pradesh and Karnataka) [11] while in the 82 SI analyzed in the present study, it was comparatively much lesser (0.6%). This discrepancy may Pharmacological Reports, 2013, 65, 167194 191 be due to the smaller sample size of SI in the present study and variation in the ethno-geographic origin of subjects in the above studies. The CYP2C9*3 allele frequency in the present Indian cohort corresponds to that observed in some Caucasian populations [4, 13, 22, 25, 27, 28], but comparatively lesser than that reported in the Netherlands [19, 20]. A recent study [16] which analyzed 102 NI reported smaller frequencies of CYP2C9*3 and VKORC1-1639A than that reported in the 209 NI in the current study. This discrepancy could be because most of the study cohort in the above study originated from the state of Uttar Pradesh while the present study included individuals originating from the states of Punjab, Haryana, New Delhi, Uttarakhand and Uttar Pradesh. There is strong evidence that patients who are homozygous or heterozygous for CYP2C9*2, *3 or/and VKORC1-1639G>A are sensitive to warfarin and acenocoumarol. They require low maintenance dose (CYP2C9*2, *3 carriers requiring reduction in dose by 16% and 41% for heterozygous and homozygous carriers, respectively), take a longer time to achieve stable dose with international normalized ratio (INR) values within the therapeutic range (2.0 to 3.0–3.5) [3, 5, 18, 22]. Multiple variants of CYP2C9 or VKORC1 increase the risk of over anticoagulation (INR ³ 4.0) and bleeding episodes [5]. Individuals heterozygous for the variants (CYP2C9*1/*2, *1/*3, VKORC1 AG) are partially sensitive to coumarin derivatives requiring intermediate doses [5, 22]. Carriers of CYP2C9 variants also have delayed stabilization of anticoagulation with both drugs [3]. Individuals with CYP2C9 *1/*1, VKORC1 -1639GG genotype are known to require the highest amount of weekly dose and are sometimes known as extensive or ultra metabolizers [5, 18, 22]. In the present study, extrapolation of FDA approved genotype-guided warfarin dose estimates revealed that a minority of North and South Indians were predicted to require low (0.5–2 mg/day) dose to achieve therapeutic anticoagulation. Intra-ethnic variation in warfarin response was observed where in a significantly higher percentage of NI would require intermediate (3–4 mg/day) dose and would be at an increased risk of bleeding episodes and over anticoagulation (INR > 3) as compared to SI. This estimation is based on reports from multiple published studies [3, 5, 18, 22]. However, since the SI sample group is smaller than that of NI, extrapolation of these dose estimates in rest of the Indian population must be done 192 Pharmacological Reports, 2013, 65, 187194 with caution. Large prospective studies are warranted to extend our findings and truly explore the variation in coumarin response in the South and North Indians. Several studies [15, 23] have established that VKORC1 SNP (-1639 A allele) accounts for 19% to 30% of variance in the dose of warfarin, while CYP2C9 SNPs (*2, *3) have a contribution of 3.2 to 12%. Prediction of warfarin response solely dependent on genotype, as attempted in the current study, is limited in explaining only a part of the inter-individual variability. As the present study was carried out in a healthy population (who were not on anticoagulation therapy), it is limited in not taking into account the non-genetic and clinical factors such as age, sex, ethnicity, body weight, concomitant medications, comorbidities and dietary vitamin K intake that are responsible for more than 50% variability in oral anticoagulation therapy [6]. There is a lack of genome wide association studies of oral anticoagulant response in the South and North Indian populations. Hence, the plausible role of rare variations in CYP2C9 and VKORC1 genes and variation in other genes (APOE, CALU, EPHX1, ABCB1, GGCX, CYP4F2) reported to be associated with warfarin response in other ethnic groups [15, 23–25], remains uncertain in the Indian population, and hence were not included in the current pilot study. Clearly, this may result in reduced accuracy of predicting warfarin dose in clinical settings. Variation in coumarin response and its genetic contribution in different populations vary mostly due to differences in the frequencies of the common CYP2C9 and VKORC1 polymorphisms or prevalence of specific polymorphisms in certain populations. The present study demonstrated that the North and South Indian populations are predicted to require variable warfarin dose due to their varied genotype frequency and may necessitate different pharmacogenetic dosing algorithms for the two Indian populations. However, a more systematic study including larger cohorts with well defined demographic/ethnicity profiles, extended candidate gene and SNP panel and comparison of predictive algorithms are needed to get a finer picture of variability in warfarin response among Indians. The identification of coumarin-sensitive patients by pharmacogenetic testing, along with appropriate clinical evaluation will allow the informed patient and physician to work together for optimizing long term anticoagulant therapy while avoiding adverse effects of the drug. Predicted coumarin response in healthy Indians Risha Nahar et al. Conclusions Studies have proved that prospective pharmacogenetic-based dosing for oral anticoagulants can help better optimize the dose and reduce drug associated bleeding events in patients. Before pharmacogenetic testing can be introduced in the Indian population, knowledge about the frequency of the variant genotypes is important to predict its usefulness and general applicability. The two ethno-geographically distinct populations, the South and North Indians, are observed to be diverse with respect to frequency of CYP2C9 *2 allele and *1/*1, *1/*2 and *3/*3 genotypes. The CYP2C9*3 allele frequency (10%) was similar to the Caucasians but higher than other Asian populations. The VKORC1-1639A allele frequency (17%) was observed to be much lower than the Caucasian and Asian populations. Prediction of warfarin dose requirement revealed variability among SI and NI. Significantly higher percentage of NI were estimated to require intermediate dose (3–4 mg/day) and were also predicted to have an increased risk of bleeding episodes and over anticoagulation as compared to SI. Conflict of interest statement: All authors declare: no financial relationships with any organizations that might have an interest in the submitted work in the previous three years, no other relationships or activities that could appear to have influenced the submitted work. Acknowledgments: We would like to thank Sir Ganga Ram Hospital for the research grant to conduct the study and acknowledge Ms. Parul Takkar for her help with statistical analyses. References: 1. Adithan C, Gerard N, Vasu S, Balakrishnan R, Shashindran CH, Krishnamoorthy R: Allele and genotype frequency of CYP2C9 in Tamilnadu population. Eur J Clin Pharmacol, 2003, 59, 707–709. 2. Basu A, Mukherjee N, Roy S, Sengupta S, Banerjee S, Chakraborty M, Dey B et al.: Ethnic India: A genomic view with special reference to peopling and structure. Genome Res, 2003, 13, 2277–2290. 3. Beinema M, Brouwers JRBJ, Schalekamp T, Wilffert B: Pharmacogenetic differences between warfarin, acencoumarol and phenprocoumon. Thromb Haemost, 2008, 100, 1052–1057. 4. Bodin L, Verstuyft C, Tregouet DA, Robert A, Dubert L, Funck-Brentano C, Jaillon P et al.: Cytochrome P450 2C9 (CYP2C9) and vitamin K epoxide reductase (VKORC1) genotypes as determinants of acenocoumarol sensitivity. Blood, 2005, 106, 135–140. 5. Carlquist JF, Horne BD, Muhlestein JB, Lappé DL, Whiting BM, Kolek MJ, Clarke JL et al.: Genotypes of the cytochrome p450 isoform, CYP2C9, and the vitamin K epoxide reductase complex subunit 1 conjointly determine stable warfarin dose: a perspective study. J Thromb Thrombolysis, 2006, 22, 191–197. 6. Coumadin Tablets (Warfarin Sodium) drug label and medication guide (revised 2010). Approved by US Food and Drug Administration: Bristol Myers Squibb Company, Princeton, New Jersey, USA, 1–33. 7. Daly AK, King BP, Leathart JBS: Genotyping for cytochrome P450 polymorphisms. Methods in Molecular Biology. CYP450- Protocols. 2nd edn., Humana Press, Totowa, NJ, 2006, 320, 193–207. 8. FDA News Release: FDA Approves Updated Warfarin (Coumadin) Prescribing Information New Genetic Information May Help Providers Improve Initial Dosing Estimates of the Anticoagulant for Individual Patients. Available from: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/2007/ucm108967.htm, 2007. 9. Gaikovitch EA, Cascorbi I, Mrozikiewicz PM, Brockmöller J, Frötschl R, Köpke K, Gerloff T et al.: Polymorphisms of drug-metabolizing enzymes CYP2C9, CYP2C19, CYP2D6, CYP1A1, NAT2 and of P-glycoprotein in a Russian population. Eur J Clin Pharmacol, 2003, 59, 303–312. 10. Geisen C, Watzka M, Sittinger K, Steffens M, Daugela L, Seifried E, Müller CR et al.: VKORC1 haplotypes and their impact on the inter-individual and inter-ethnical variability of oral anticoagulation. Thromb Haemost, 2005, 94, 773–779. 11. Jose R, Chandrasekaran A, Sam SS, Gerard N, Chanolean S, Abraham BK, Satyanarayanamoorthy K et al.: CYP2C9 and CYP2C19 genetic polymorphisms: frequencies in the south Indian population. Fund Clin Pharmacol, 2004, 19, 101–105. 12. Lee SC, Ng SS, Oldenburg J, Chong PY, Rost S, Guo JY, Yap HL et al.: Interethnic variability of warfarin maintenance requirement is explained by VKORC1 genotype in an Asian population. Clin Pharmacol Ther, 2006, 79, 197–205. 13. Markatos CN, Grouzi E, Politou M, Gialeraki A, Merkouri E, Panagou I, Spiliotopoulou I, Travlou A: VKORC1 and CYP2C9 allelic variants influence acenocoumarol dose requirements in Greek patients. Pharmacogenomics, 2008, 9, 1631–1638. 14. Miller SA, Dykes DD, Polesky HF: A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res, 1988, 16, 1215. 15. Pautas E, Moreau C, Gouin-Thibault I, Golmard JL, Mahé I, Legendre C, Taillandier-Hériche E et al.: Genetic factors (VKORC1, CYP2C9, EPHX1, and CYP4F2) are predictor variables for warfarin response in very elderly, frail inpatients. Clin Pharmacol Ther, 2010, 87, 57–64. 16. Rathore SS, Agarwal SK, Pande S, Mittal T, Mittal B: Frequencies of VKORC1-1639G>A, CYP2C9*2 and Pharmacological Reports, 2013, 65, 167194 193 17. 18. 19. 20. 21. 22. 23. 194 CYP2C9*3 genetic variants in the north Indian population. BioScience Trends, 2010, 4, 333–337. Reich D, Thangaraj K, Patterson N, Price AL, Singh L: Reconstructing Indian population history. Nature, 2009, 461, 489–494. Rieder MJ, Reiner AP, Gage BF, Nickerson DA, Eby CS, McLeod HL, Blough DK et al.: Effect of VKORC1 haplotypes on transcriptional regulation and warfarin dose. N Engl J Med, 2005, 352, 2285–2293. Schalekamp T, Brassé BP, Roijers JF, Chahid Y, van Geest-Daalderop JH, de Vries-Goldschmeding H, van Wijk EM et al.: VKORC1 and CYP2C9 genotypes and acenocoumarol anticoagulation status: Interaction between both genotypes affects overanticoagulation. Clin Pharmacol Ther, 2006, 80, 13–22. Schalekamp T, Geest-Daalderop JV, Goldchmeding HDV, Conemans J, Bernsen MJ, Boer AD: Acenocoumarol stabilization is delayed in CYP2C9*3 carriers. Clin Pharmacol Ther, 2004, 75, 394–402. Sconce EA, Khan TI, Wynne HA, Avery P, Monkhouse L, King BP, Wood P et al.: The impact of CYP2C9 and VKORC1 genetic polymorphism and patient characteristics upon warfarin dose requirements: proposal for a new dosing regimen. Blood, 2005, 106, 2329–2333. Takahashi H, Wilkinson GR, Nutescu EA, Morita T, Ritchie MD, Scordo MG, Pengo V et al.: Different contributions of polymorphisms in VKORC1 and CYP2C9 to intra- and inter-population differences in maintenance dose of warfarin in Japanese, Caucasians and AfricanAmericans. Pharmacogenet Genomics, 2006,16, 101–110. Takeuchi F, McGinnis R, Bourgeois S, Barnes C, Eriksson N, Soranzo N, Whittaker P et al.: A genomewide association study confirms VKORC1, CYP2C9, Pharmacological Reports, 2013, 65, 187194 24. 25. 26. 27. 28. 29. 30. and CYP4F2 as principal genetic determinants of warfarin dose. PLoS Genet, 2009, 5, e1000433. Voora D, McLeod HL, Eby C, Gage BF: The pharmacogenetics of coumarin therapy. Pharmacogenomics, 2005, 6, 503–513. Wadelius M, Chen LY, Eriksson N, Bumpstead S, Ghori J, Wadelius C, Bentley D et al.: Association of warfarin dose with genes involved in its action and metabolism. Hum Genet, 2007, 121, 23–34. Wadelius M, Pirmohamed M: Pharmacogenetics of warfarin: current status and future challenges. Pharmacogenomics J, 2007, 7, 99–111. Yang JQ, Morin S, Verstuyft C, Fan LA, Zhang Y, Xu CD, Barbu V et al.: Frequency of cytochrome P450 2C9 allelic variants in the Chinese and French populations. Fundam Clin Pharmacol, 2003, 17, 373–376. Yasar U, Eliasson E, Dahl ML, Johansson I, IngelmanSundberg M, Sjoqvist F: Validation of methods for CYP2C9 genotyping: Frequencies of mutant alleles in a Swedish population. Biochem Biophys Res Commun, 1999, 254, 628–631. Yoon YR, Shon JH, Kim MK, Lim YC, Lee HR, Park JY, Cha IJ, Shin JG: Frequency of cytochrome P450 2C9 mutant alleles in a Korean population. Br J Clin Pharmacol, 2001, 51, 277–280. Yuan HY, Chen JJ, Lee MT, Wung JC, Chen YF, Charng MJ, Lu MJ et al.: A novel functional VKORC1 promoter polymorphism is associated with inter-individual and inter-ethnic differences in warfarin sensitivity. Hum Mol Genet, 2005, 14, 1745–1751. Received: September 2, 2011; in the revised form: August 8, 2012; accepted: October 8, 2012.