Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
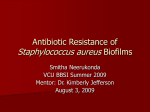
Journal of Medical Microbiology (2014), 63, 1509–1516 DOI 10.1099/jmm.0.075374-0 A combination of cis-2-decenoic acid and antibiotics eradicates pre-established catheter-associated biofilms Azadeh Rahmani-Badi,1 Shayesteh Sepehr,1 Parisa Mohammadi,1 Mohammad Reza Soudi,1 Hamta Babaie-Naiej1 and Hossein Fallahi2,3 Correspondence 1 Azadeh Rahmani-Badi 2 [email protected] Department of Biology, Alzahra University, Tehran, Iran Department of Biology, Razi University, Kermanshah, Iran 3 Medical Biology Research Center, Kermanshah University of Medical Sciences, Kermanshah, Iran Received 12 March 2014 Accepted 29 July 2014 The catheterized urinary tract provides ideal conditions for the development of biofilm populations. Catheter-associated urinary tract infections (CAUTIs) are recalcitrant to existing antimicrobial treatments; therefore, established biofilms are not eradicated completely after treatment and surviving biofilm cells will carry on the infection. Cis-2-decenoic acid (CDA), an unsaturated fatty acid, is capable of inhibiting biofilm formation by Pseudomonas aeruginosa and of inducing the dispersion of established biofilms by multiple types of micro-organisms. Here, the ability of CDA to induce dispersal in pre-established single- and dual-species biofilms formed by Escherichia coli and Klebsiella pneumoniae was measured by using both semi-batch and continuous cultures bioassays. Removal of the biofilms by combined CDA and antibiotics (ciprofloxacin or ampicillin) was evaluated using microtitre plate assays (crystal violet staining). The c.f.u. counts were determined to assess the potential of combined CDA treatments to kill and eradicate preestablished biofilms formed on catheters. The effects of combined CDA treatments on biofilm surface area and bacteria viability were evaluated using fluorescence microscopy, digital image analysis and live/dead staining. To investigate the ability of CDA to prevent biofilm formation, single and mixed cultures were grown in the presence and absence of CDA. Treatment of preestablished biofilms with only 310 nM CDA resulted in at least threefold increase in the number of planktonic cells in all cultures tested. Whilst none of the antibiotics alone exerted a significant effect on c.f.u. counts and percentage of surface area covered by the biofilms, combined CDA treatments led to at least a 78 % reduction in biofilm biomass in all cases. Moreover, most of the biofilm cells remaining on the surface were killed by antibiotics. The addition of 310 nM CDA significantly prevented biofilm formation by the tested micro-organisms, even within mixed cultures, indicating the ability of CDA to inhibit biofilm formation by other types of bacteria in addition to Pseudomonas aeruginosa. These findings suggested that the biofilm-preventive characteristics of CDA make it a noble candidate for inhibition of biofilm-associated infections such as CAUTIs, which paves the way toward developing new strategies to control biofilms in clinical as well as industrial settings. INTRODUCTION The biofilm mode of growth is a basic survival strategy deployed by bacteria in a wide range of environmental, industrial and clinical settings (Stoodley et al., 2002). The catheterized urinary tract provides ideal conditions for the development of enormous biofilm populations. Consequently, catheter-associated urinary tract infections (CAUTIs) are amongst the most common infectious Abbreviations: CAUTI, catheter-associated urinary tract infection; CDA, cis-2-decenoic acid; EPS, extracellular polymeric substance. 075374 G 2014 The Authors diseases of humans, and significantly burden the healthcare system by increasing both morbidity and treatment costs (Ulett et al., 2007). The initial infections are usually by single bacterial species, such as Escherichia coli, Staphylococcus epidermidis and Enterococcus faecalis (Stickler, 2008). However, over time, a variety of organisms, including Klebsiella pneumoniae, Pseudomonas aeruginosa, Proteus mirabilis and Morganella morganii, colonize the bladder urine and form poly-microbial communities that are embedded in protective self-produced extracellular polymeric substances (EPSs) (Stickler, 2008). In order to Downloaded from www.microbiologyresearch.org by IP: 88.99.165.207 On: Sun, 07 May 2017 07:25:12 Printed in Great Britain 1509 A. Rahmani-Badi and others inactivate these encased cells, antimicrobial molecules must diffuse through the biofilm EPSs and gain access to the microbial cells in sufficient concentrations (Walters et al., 2003). However, EPSs present a diffusional barrier for these molecules either by influencing the rate of transport of the molecule to the biofilm interior (e.g. ciprofloxacin and ampicillin) (Anderl et al., 2000) or by reaction of the antimicrobial material with the matrix material (Campanac et al., 2002). Thus, micro-organisms that are sensitive to antibiotics in their planktonic phenotype become resistant in their biofilm mode of growth (Stickler, 2008). This characteristic makes CAUTIs, like other biofilm-associated infections, recalcitrant to treatment by using existing antimicrobial treatments, and it is a common and frustrating experience that after treatment, established biofilms are not completely eradicated and surviving biofilm cells carry on the infection (Fux et al., 2005). To address the need for novel and improved measures against biofilms, especially preestablished biofilms, a clear strategy is to study the biofilm life cycle and identify key trigger points that regulate biofilm development. To control biofilm, the last stage of biofilm development presents several advantages, when a coordinated dispersal of biofilm cells is possible. Induction of biofilm dispersal can potentially use the micro-organisms’ own energy to remove EPSs and disrupt pre-established biofilms, which results in cells reverting to a planktonic phenotype and restores their susceptibility to antibiotics. It has been reported recently that Pseudomonas aeruginosa produces a diffusible signal factor family signal, cis-2decenoic acid (CDA), which is capable of inhibiting biofilm formation by Pseudomonas aeruginosa and of inducing the dispersion of established biofilms by multiple types of micro-organisms (bacteria as well as yeast) (Davies & Marques, 2009). In fact, CDA is involved in inter-species and inter-kingdom signalling where it can modulate the behaviour of other micro-organisms that do not produce the signal (Davies & Marques, 2009). Its broad spectrum of activity in addition to the fact that it has no cytotoxic effects on human cells at the nanomolar range (Jennings et al., 2012) makes CDA a promising candidate for the control of biofilms. However, there is limited information on the potential of CDA to boost the actions of antimicrobial agents. Therefore, in the current work the ability of CDA to induce dispersal in established single- and dual-species biofilms formed by E. coli and K. pneumoniae, and to eradicate their biofilms when combined with antibiotics, was studied. In addition, the ability of CDA to prevent biofilm formation by these pathogens and to increase the inhibitory effects of antibiotics on the growth of bacterial planktonic cells was investigated. METHODS Bacterial strains, media and growth conditions. The micro- organisms used in the present study included E. coli (ATCC 25922) and K. pneumoniae (ATCC 700603). All cultivations were performed 1510 in artificial urine adopted by Griffith et al. (1976) containing calcium chloride (0.49 g l21), magnesium chloride hexahydrate (0.65 g l21), sodium chloride (4.6 g l21), disodium sulphate (2.3 g l21), trisodium citrate dihydrate (0.65 g l21), disodium oxalate (0.02 g l21), potassium dihydrogen phosphate (2.8 g l21), potassium chloride (1.6 g l21), ammonium chloride (1.0 g l21), urea (25 g l21) and gelatine (5.0 g l21). The pH of the medium was adjusted to 6.1 and then the medium was sterilized by membrane filtration. Tryptone soya broth (Merck) was prepared separately, autoclaved and added to the sterile basal medium to a final concentration of 1.0 g l21. Medium was supplemented (as required) with antibiotic (chloramphenicol at a final concentration of 20 mg ml21). Chemicals and antimicrobial compounds. Three different con- centrations of CDA (U-Chemo; 100, 310 or 620 nM) were used. These concentrations were observed previously to have the most effect on inducing the dispersion of pre-established biofilms and on inhibiting biofilm development (Davies & Marques, 2009) with no cytotoxic effects on human cells (Jennings et al., 2012). Ethanol (10 %) (Merck) was used as a carrier for CDA. This study also examined the effects of two antibiotics, ciprofloxacin (Sigma) and ampicillin (Sigma), which are used widely in treatment of urinary tract infections. Ciprofloxacin was used at a final concentration of 1 mg ml21 and ampicillin was used at a final concentration of 256 mg ml21. The concentration of the selected antibiotics was established in our laboratory to be effective against planktonic cells, but have no inhibitory effect on the biofilm cells of the test micro-organisms. Single-and dual-species biofilm dispersal bioassays in Petri dishes. Single-species biofilms of E. coli and K. pneumoniae as well as their dual-species biofilms were cultivated on the inside surface of sterile Petri dishes (Barraud et al., 2006). Plates were incubated for 5 days at 37 uC with shaking at 30 r.p.m., in triplicate. Medium in the plates was replaced every 24 h to reduce the accumulation of native dispersion-inducing factors and to allow mature biofilms to form. After the final exchange of medium, the cells were allowed to grow for ~1 h and then dispersion induction was tested by replacing the growth medium with fresh medium containing one of the indicated concentrations of CDA (100, 310 or 620 nM) or just the carrier as a control and the cells were incubated for a further 1 h. Medium containing dispersed cells was then homogenized for 30 s at 5000 r.p.m. and cell density was determined based on the OD600. Dispersion bioassays in biofilm tube reactors. Single- and dual- species biofilms were also grown on the interior surfaces of tubing of a once-through continuous-flow reactor system at 37 uC. The silicone tubes were inoculated by syringe injection through a septum 1 cm upstream from each reactor tube with 3 ml of overnight cultures of each micro-organism to cultivate single-species biofilms. To grow dualspecies biofilms, 1.5 ml overnight cultures of E. coli and K. pneumoniae were mixed well and then used as inoculum. Cells were allowed to attach (static incubation) to the tubing for 1 h, after which the flow was started at an elution rate of 280 ml min21. After 5 days of biofilm culture, the influent medium was switched from fresh medium in the test lines to one of the three indicated concentrations of CDA. Control lines were switched to new lines containing just the carrier. Samples were collected in test tubes on ice and were subsequently homogenized, and cell density was determined as described above. Combined CDA and antibiotic biofilm microtitre plate assays. To assess the effect of antibiotics alone or in combination with CDA, biofilms were grown on the inside surface of sterile polystyrene 96well plates. To cultivate biofilms, plates were inoculated with either 150 ml per well of overnight culture of each test micro-organism (to grow single-species biofilms) or mixtures of two bacteria overnight cultures (to cultivate dual-species biofilms) and then were incubated at 37 uC with shaking at 120 r.p.m. Medium within each well was Downloaded from www.microbiologyresearch.org by IP: 88.99.165.207 On: Sun, 07 May 2017 07:25:12 Journal of Medical Microbiology 63 Eradication of catheter-associated biofilms replaced every 24 h for 5 days. The biofilms were then treated for 1 h with the indicated concentrations of antibiotics alone or combined with 310 nM CDA and biofilms were monitored by crystal violet staining as described by Musk & Hergenrother (2008). All experiments were repeated at least four times. (100, 310 or 620 nM) on the growth of planktonic cells of the test micro-organisms. The MICs were determined in triplicate in Mueller–Hinton broth by using a microdilution assay with bacteria at a density of 105 c.f.u. ml21. Plates were incubated for 24 h at 37 uC. The lowest concentration of antibiotics where there was no growth after 24 h was taken as the MIC (CLSI, 2006). Biofilm formation on catheters. Biofilm formation was also assayed under hydrodynamic conditions in silicone catheters. Pieces of catheter (100 % silicon) with a length of 3.0 cm were cut, sterilized in 0.5 % sodium hypochlorite for 1 h and then washed extensively with sterile water. Each piece of catheter was put into a glass tube with 5.0 ml growth medium. The tubes were then inoculated with 50 ml of a culture of each test micro-organism freshly grown overnight (to cultivate single-species biofilms) or their mixtures (to grow dualspecies biofilms). The tubes were left at 37 uC in a water bath with shaking at 110 r.p.m. for 5 days. Medium in each tube was replaced every 24 h for 5 days. The biofilms were then treated for 1 h with the indicated concentrations of antibiotics alone or combined with 310 nM CDA. The amount of adhered bacteria on the catheters was examined by viable counts. The catheter pieces were first washed in 50 ml PBS three times and excess liquid was removed by capillarity on adsorbent paper to reduce the influence of non-attached or loosely attached bacteria. The catheter pieces were then placed into plastic tubes containing 5.0 ml PBS. Adhered bacteria were detached by sonication for 4 min at 42 Hz at room temperature, followed by vortexing at maximum velocity for 15 s, and then serial dilution and plating onto LB agar plates. The sonication procedure did not adversely affect bacterial viability (this was confirmed by plating samples of bacterial liquid cultures before and after sonication). Flow cell (continuous culture) biofilm experiments, antibiotics sensitivity assays and surface area coverage. To observe the effect of combined CDA and antibiotic treatments on biofilm surface area and bacteria viability, single- and dual-species biofilms of GFPexpressing E. coli and K. pneumoniae carrying plasmid pAmr93 (generously provided by E. Peter Greenberg, Department of Microbiology, University of Washington, School of Medicine, Seattle WA, USA) were also grown in synthetic urine, supplemented with chloramphenicol at 37 uC in continuous culture flow cells (channel dimensions, 164640 mm). After 48 h of biofilm culture, the influent medium was switched from fresh medium in the test lines to the antibiotics alone or in combination with 310 nM CDA. After 1 h treatment, biofilms were stained with 30 mM propidium iodide, which labels dead cells red. Using epifluorescence microscopy (CETI), 15 selected fields of view per flow cell were imaged in the xy plane, at regular intervals and across the entire channels. Image analysis (ImageJ software; http://imagej.nih.gov/ij/) was performed, and results were presented as the percentage of total biofilm surface reduction in cultures subjected to combined CDA and antibiotic treatments relative to the total biofilm surface in control cultures that were not exposed to CDA. Statistical comparison of the percentage of surface covered by biofilms in the different treatments was performed using ANOVA. Three replicates per experiment were used and at least two independent repetition experiments were performed. Inhibition of biofilm formation on catheters by CDA. Biofilm formation was assayed in silicone catheters. Each piece of catheter was put into a glass tube with 5.0 ml growth medium (as described above) with or without 310 nM CDA. The tubes were then inoculated with 50 ml overnight culture of each test micro-organism (to cultivate singlespecies biofilms) or their mixtures (to grow dual-species biofilms). The tubes were then left at 37 uC in a water bath with shaking at 110 r.p.m. for 24 h before analysis. After plating onto LB agar, c.f.u. were counted. Combined CDA and antibiotic treatment of planktonic cells. We have also evaluated the probable inhibitory effects of antibiotics alone or in combination with three different concentrations of CDA http://jmm.sgmjournals.org RESULTS Very low concentrations of CDA induce biofilm dispersal We investigated the effect of exposure to nanomolar concentrations of CDA on pre-established single- and dualspecies biofilms in Petri dish cultures. CDA treatments resulted in a significant increase in the populations of planktonic cells released into the bulk liquid compared with untreated control samples. The greatest effect was observed repeatedly with 310 nM CDA with at least a threefold increase in the number of planktonic cells. At this concentration, the largest increase in the planktonic population was observed in the case of single-species biofilms of K. pneumoniae and also dual-species biofilms (OD600 0.92±0.01, P¡0.05 and 1.10±0.01, P¡0.05, respectively) versus untreated controls (OD60050.62±0.01, P¡0.05 and 0.78±0.02, P¡0.05, respectively). The results from these experiments are summarized in Table 1. We also examined the effect of exposure to very low concentrations of CDA on preestablished biofilms grown in continuous cultures on the inner surface of silicone tubing. We again observed an increase in the population of planktonic cells after treatment with CDA, indicating the release of biofilm bacteria into the effluent of cultures treated with CDA. As for semi-batch biofilm cultures, a threefold increase in the number of planktonic cells in the effluent runoffs was observed in cultures treated with 310 nM CDA (Table 2), which was the largest increase in all cases. At this concentration, CDA caused a significant increase in the population of planktonic cells especially in dual-species biofilms (OD600 0.51±0.03, P¡0.05) compared with the results for untreated controls (OD600 0.18±0.01, P¡0.05). Therefore, 310 nM CDA was used for further studies. The results from these two different dispersal bioassays demonstrated the ability of CDA to stimulate the release of cells from established biofilms, formed by catheterassociated bacteria, even within mixed cultures. Combined CDA and antibiotic treatment killed and removed pre-established biofilms formed on different surfaces We tested the effectiveness of combined CDA treatments on the removal of pre-established single- and dual-species biofilms formed on the inside surface of polystyrene 96-well plates. After 120 h growth, biofilms were treated with two antibiotics (ampicillin or ciprofloxacin) at the indicated concentrations, alone or in combination with 310 nM CDA. The remaining biofilms were then stained Downloaded from www.microbiologyresearch.org by IP: 88.99.165.207 On: Sun, 07 May 2017 07:25:12 1511 A. Rahmani-Badi and others Table 1. Activity of CDA as an inducer of biofilm dispersion using Petri dish bioassays Cell density of medium containing dispersed cells was determined by measuring the OD600; values represent the mean±SD calculated from three replicate experiments (P¡0.05). Micro-organism K. pneumoniae E. coli E. coli+K. pneumoniae CDA concentration Control 100 nM 310 nM 620 nM 0.62±0.01 0.66±0.02 0.78±0.02 0.80±0.02 0.78±0.02 0.86±0.05 0.92±0.01 0.9±0.05 1.10±0.01 0.89±0.02 0.82±0.01 1.00±0.01 with 0.1 % crystal violet. We observed that combined treatments with both CDA and antibiotics had a significant effect on removing pre-established biofilms (e.g. in the absence of CDA, ampicillin caused only 21 % reduction in dual-species biofilms, whereas addition of 310 nM CDA resulted in 78 % biofilm removal) (Fig. 1a). However, the largest biofilm removal was observed when both types of biofilms were treated with a combination of CDA and ciprofloxacin, which resulted in 90 % reduction in biofilm biomass in single-species biofilms and ~80 % biofilm removal in dual-species biofilms (Fig. 1a). We also examined the effect of combined CDA and antibiotic treatment on the killing and eradication of preestablished biofilms grown on urinary catheters. When 120 h biofilms were treated in the absence of CDA, both antibiotics caused a roughly twofold decrease in c.f.u. counts compared with untreated controls, whilst combined exposure of cultures to either 310 nM CDA and only 256 mg ampicillin ml21 or 310 nM CDA and 1 mg ciprofloxacin ml21 resulted in at least a fourfold decrease in c.f.u. counts (Fig. 1b). This demonstrated that CDA removed biofilms not only from the polystyrene surfaces, as shown in microtitre plates, but also from silicone surfaces of urinary catheters. continuous culture flow cells. When 48 h biofilms were treated in the absence of CDA, none of the antibiotics exerted a significant effect on the percentage of surface area covered by the biofilms (Fig. 2). In contrast, after combined treatment, the biofilm cells remaining on the surface were easily removed and killed by antibiotics when examined by using live/dead staining (Fig. 2). As for microtitre assays, the largest reduction in biofilm biomass was observed when pre-established single- and dual-species biofilms were treated with a combination of CDA and ciprofloxacin, giving ~90 and 80 % biofilm removal, respectively (Fig. 2a). Therefore, combined treatments with both CDA and antibiotics caused almost complete removal of preestablished single- and dual-species biofilms formed by catheter-associated micro-organisms. CDA prevented biofilm formation on urinary catheters Combined CDA and antibiotic treatment significantly reduced biofilm surface coverage Test micro-organisms were also used to investigate the inhibitory role of additional CDA in biofilm formation by both single- and mixed-cultures on silicone catheters. Determinations of c.f.u. (mm catheter)–1 revealed a twofold reduction in biofilms by only 310 nM CDA (Fig. 3), indicating the ability of CDA to inhibit biofilm formation by other types of bacteria in addition to Pseudomonas aeruginosa. To further examine the effect of CDA on biofilm eradication, we also tested combined CDA and antibiotic treatment against pre-established biofilms cultivated in To further investigate the effect of CDA on the sensitivity of test micro-organisms towards antibiotics, we also evaluated very low concentrations of CDA for inhibitory effects on the Table 2. Activity of CDA as an inducer of biofilm dispersal using tube reactor bioassays Cell density of medium containing dispersed cells was determined by measuring the OD600; values represent the mean±SD calculated from three replicate experiments (P¡0.05). Micro-organism K. pneumoniae E. coli E. coli+K. pneumoniae 1512 CDA concentration Control 100 nM 310 nM 620 nM 0.15±0.01 0.17±0.01 0.18±0.01 0.35±0.01 0.3±0.01 0.34±0.02 0.44±0.01 0.36±0.02 0.51±0.03 0.39±0.02 0.31±0.01 0.46±0.01 Downloaded from www.microbiologyresearch.org by IP: 88.99.165.207 On: Sun, 07 May 2017 07:25:12 Journal of Medical Microbiology 63 Eradication of catheter-associated biofilms –CDA (a) +CDA 100 60 E. coli 50 Biofilm remaining (% of control) Biofilm remaining (% of control) +CDA 40 30 20 10 0 –CDA E. coli+K. pneumoniae +CDA 80 K. pneumoniae 50 Biofilm remaining (% of control) –CDA 60 40 30 20 60 40 20 10 0 Amp 256 mg ml–1 Cip 1 mg ml–1 Amp 256 mg ml–1 Cip 1 mg ml–1 E. coli K. pneumoniae Dual-species biofilm (b) 3.0 Biofilm formation [c.f.u. (mm catheter)–1] (×106) 0 Amp 256 mg ml–1 Cip 1 mg ml–1 2.5 2.0 1.5 1.0 0.5 0 Amp (–CDA) Amp+CDA Cip (–CDA) Cip+CDA Control Fig. 1. Effect of CDA in combination with antibiotics on pre-established single- and dual-species biofilm removal. (a) The amount of biofilm remaining after treatment with the tested concentrations of antibiotics [ampicillin (Amp) and ciprofloxacin (Cip)] alone (–CDA) or in combination with 310 nM CDA (+CDA) for 1 h was determined by the measurement of A590 of crystal violet by staining the 120 h biofilms in a microtitre plate assay. All readings are corrected to reflect 0 and 100 % controls (blank well, 0 %; biofilms without any treatments, 100 %). Bar, SD (n54). (b) After treatment of the biofilms with antibiotics alone or combined with 310 nM CDA, c.f.u. plate counts were determined to assess the viability of the bacteria (n59). growth of planktonic cells. Compared with antibiotics alone, the combination of nanomolar concentrations of CDA with antibiotics had no additional inhibitory effects on the growth of planktonic cells (Table 3). DISCUSSION Microbial biofilms are an increasing concern in the medical field where the use of artificial medical devices for therapeutic and restorative purposes is on the rise. CAUTIs are notable examples of this, and illustrate the significant economic and medical problems associated with the use of such devices (Stamm, 1991; Tambyah et al., 2002). http://jmm.sgmjournals.org In the long quest aiming to prevent or reduce the accumulation of microbial biofilms, many different strategies have been proposed with different degrees of success (Yang et al., 2012). In various industrial settings, a range of biocides and toxic metals (e.g. tin and copper) have been used for antifouling coatings and sanitizing purposes (Cloete et al., 1998; Chambers et al., 2006). These substances are, however, not appropriate for use in medical implants and therefore other strategies have been sought. For example, in urology, a range of urinary catheters has been developed which incorporate and/or release antimicrobial compounds, e.g. metals (such as silver salts) and antibiotics (Darouiche et al., 1999; Johnson et al., 2006). Nevertheless, the general risk of antibiotic resistance development associated with these compounds has resulted Downloaded from www.microbiologyresearch.org by IP: 88.99.165.207 On: Sun, 07 May 2017 07:25:12 1513 A. Rahmani-Badi and others (a) K. pneumoniae E. coli Dual-species biofilm Untreated control Untreated control Untreated control Amp (–CDA) Amp+CDA Amp (–CDA) Amp+CDA Amp (–CDA) Amp+CDA Cip (–CDA) Cip+CDA Cip (–CDA) Cip+CDA Cip (–CDA) Cip+CDA 60 50 40 30 20 10 0 Control –CDA 80 Surface coverage (%) Surface coverage (%) +CDA E. coli Amp 256 µg ml–1 Cip 1 µg ml–1 +CDA 70 +CDA E. coli+K. pneumoniae 100 60 50 40 30 20 10 0 –CDA K. pneumoniae Surface coverage (%) –CDA (b) 80 70 Control Amp 256 µg ml–1 Cip 1 µg ml–1 80 60 40 20 0 Control Amp 256 µg ml–1 Cip 1 µg ml–1 Fig. 2. Biofilms were grown using GFP-labelled E. coli and K. pneumoniae for 48 h. Following dispersion of biofilms by CDA, cells remaining on the surface were easily removed by antibiotics [ampicillin (Amp) and ciprofloxacin (Cip)]. After treatments, biofilms were stained with 30 mM propidium iodide, which labels dead cells red, and quantified (per cent surface coverage) using digital image analysis. (a) Microscopic images of the biofilms on the surface of coverslips after combinatorial treatments. Images are top-down views (xy plane). Bars, 50 mm. (b) The columns show the levels of biofilm biomass after antimicrobial treatments when used alone (–CDA) or combined with CDA (+CDA). Bar, SD. Results are representative of three separate experiments. in limited use of such strategies (Ramos et al., 2011). Therefore, additional strategies are being developed in order to reduce catheter-associated biofilms. In a previous study, Cobrado et al. (2012) suggested that cerium nitrate, low-molecular-mass chitosan and hamamelitannin are biocompatible compounds that could be used to coat medical devices. However, their in vivo studies revealed that amongst these compounds, only hamamelitannin could inhibit biofilm formation by all the bacteria tested. According to Cobrado et al. (2013), a more durable coating strategy and further in vivo testing for these compounds are needed in order to develop a cost-effective and biocompatible indwelling catheter that could reduce medical deviceassociated biofilms more effectively than the present available options. The main feature of biofilms is the production of EPSs to build a matrix for embedding the cells, and protecting them from shearing forces and undesirable conditions, 1514 including the presence of most antimicrobial agents (Flemming & Wingender, 2010). In a previous study, Davies & Marques (2009) reported that CDA, a signalling molecule synthesized by Pseudomonas aeruginosa, induces dispersion of pre-established biofilms in this bacterium, as well as many other strains of micro-organisms. Induction of biofilm dispersal can potentially use the microorganisms’ own energy to remove EPSs and disrupt preestablished biofilms, revert cells to a planktonic phenotype, and restore their susceptibility to antimicrobial agents. Therefore, in this study, we first examined the impacts of nanomolar concentrations of CDA (as an inducer of biofilm dispersal) on dispersion of single- and mixedspecies biofilms formed by the top two species in CAUTIs, E. coli and K. pneumoniae, which are also excellent biofilm formers (Dalgaard, 1995; Hancock et al., 2010). Our data showed that treatment of pre-established biofilms with only 310 nM CDA resulted in at least a threefold increase in the number of planktonic cells in all the cultures tested. Downloaded from www.microbiologyresearch.org by IP: 88.99.165.207 On: Sun, 07 May 2017 07:25:12 Journal of Medical Microbiology 63 Eradication of catheter-associated biofilms Biofilm formation [c.f.u. (mm catheter)–1] 14000 Table 3. Susceptibility profiles (MIC; mg ml”1) of E. coli and K. pneumoniae to the examined antibiotics in the presence and absence of three different concentrations of CDA No CDA 12000 310 nM CDA 10000 Treatment 8000 6000 4000 2000 0 K. pneumoniae E. coli Dual-species biofilm Fig. 3. Addition of CDA inhibits biofilm formation of E. coli and K. pneumoniae on urinary catheters. Biofilm formation by test bacteria in synthetic urine in the presence and absence of 310 nM CDA was examined on urinary catheters (100 % silicone) by viable counts. Catheters were incubated for 24 h, washed and sonicated, and serial dilutions were plated for determination of c.f.u. Results displayed are mean±SD of three replicates. Bacteria formed significantly less biofilm on catheters in medium with CDA (‘310 nM CDA’) than in medium without additional CDA (‘No CDA’) (P,0.01 by t-test). Then, we successfully removed both types of biofilm culture by using a combination of CDA and common antibiotics at concentrations that had not been significantly effective against biofilms in previous studies (Barraud et al., 2006). The results presented here demonstrated that following exposure to low concentrations of CDA, cells remaining on the surface were easily killed by antibiotics even within mixed cultures. We confirmed that the combination of 310 nM CDA with ciprofloxacin and ampicillin, which are used widely in the treatment of CAUTIs, resulted in up to 90 % reduction in biofilm biomass in all cases. Moreover, live/dead staining experiments showed that most of the biofilm cells remaining on the surface were killed by antibiotics. We also showed that, in addition to dispersal of pre-established biofilms, CDA inhibited biofilm formation by bacterial species other than Pseudomonas aeruginosa. This anti-biofilm activity could be useful in prophylactic measures for preventing biofilmassociated infections such as CAUTIs. CDA-based strategies to induce biofilm dispersal or to prevent biofilm formation contain very low concentrations of CDA, only in the nanomolar range, which should be safe to humans and to the environment. Moreover, in a previous study, Jennings et al. (2012) have shown that CDA has no cytotoxic or stimulatory effect on human cells even at high concentrations (up to 250 mg ml21). Some free fatty acids have been reported to have antimicrobial properties (Desbois et al., 2008; Desbois & Smith, 2010) and play an important role in maintaining the microbial flora of the http://jmm.sgmjournals.org Ampicillin (2 CDA) Ampicillin+100 nM CDA Ampicillin+310 nM CDA Ampicillin+620 nM CDA Ciprofloxacin (2 CDA) Ciprofloxacin+100 nM CDA Ciprofloxacin+310 nM CDA Ciprofloxacin+620 nM CDA Micro-organism E. coli K. pneumoniae 128 128 128 128 0.06 0.06 0.06 0.06 128 128 128 128 0.125 0.125 0.125 0.125 skin (Kenny et al., 2009; Takigawa et al., 2005). However, we demonstrated that CDA did not inhibit bacterial growth at the nanomolar range that induces biofilm dispersal. These results were highly consistent with results obtained from Jennings et al. (2012) showing that CDA inhibited bacterial growth only at micro- to millimolar concentrations. This lack of growth inhibition at lower concentrations was not surprising as bacteria produce this fatty acid and use it as a signalling molecule (Davies & Marques, 2009). CDA mediates the transition from a biofilm to a planktonic phenotype via a signalling mechanism (because it acts at nanomolar concentrations, consistent with all known cell–cell signalling molecules) rather than a toxic effect. Therefore, CDA-based biofilm control strategies would not be expected to select for resistant strains, as seen with antibiotics. The application of a dispersion inducer prior to, or in combination with, treatment by antimicrobial agents provides a promising mechanism for enhancing the activity of these treatments through the disruption of existing biofilms. ACKNOWLEDGEMENTS We sincerely thank Dr David G. Davies (Department of Biological Sciences, State University of New York, Binghamton, USA) for valuable information about CDA and also for providing protocols for biofilm dispersal bioassays. REFERENCES Anderl, J. N., Franklin, M. J. & Stewart, P. S. (2000). Role of antibiotic penetration limitation in Klebsiella pneumoniae biofilm resistance to ampicillin and ciprofloxacin. Antimicrob Agents Chemother 44, 1818– 1824. Barraud, N., Hassett, D. J., Hwang, S. H., Rice, S. A., Kjelleberg, S. & Webb, J. S. (2006). Involvement of nitric oxide in biofilm dispersal of Pseudomonas aeruginosa. J Bacteriol 188, 7344–7353. Campanac, C., Pineau, L., Payard, A., Baziard-Mouysset, G. & Roques, C. (2002). Interactions between biocide cationic agents and bacterial biofilms. Antimicrob Agents Chemother 46, 1469–1474. Downloaded from www.microbiologyresearch.org by IP: 88.99.165.207 On: Sun, 07 May 2017 07:25:12 1515 A. Rahmani-Badi and others Chambers, L. D., Stokes, K. R., Walsh, F. C. & Wood, R. J. K. (2006). Johnson, J. R., Kuskowski, M. A. & Wilt, T. J. (2006). Systematic Modern approaches to marine antifouling coatings. Surf Coat Technol 201, 3642–3652. review: antimicrobial urinary catheters to prevent catheter-associated urinary tract infection in hospitalized patients. Ann Intern Med 144, 116–126. Cloete, T. E., Jacobs, L. & Brözel, V. S. (1998). The chemical control of biofouling in industrial water systems. Biodegradation 9, 23–37. CLSI (2006). Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically, Approved Standard, 7th edn, M7-A7. Wayne, PA: Clinical and Laboratory Standards Institute. Cobrado, L., Azevedo, M. M., Silva-Dias, A., Ramos, J. P., Pina-Vaz, C. & Rodrigues, A. G. (2012). Cerium, chitosan and hamamelitannin as novel biofilm inhibitors? J Antimicrob Chemother 67, 1159–1162. Cobrado, L., Silva-Dias, A., Azevedo, M. M., Pina-Vaz, C. & Rodrigues, A. G. (2013). In vivo antibiofilm effect of cerium, chitosan and hamamelitannin against usual agents of catheter-related bloodstream infections. J Antimicrob Chemother 68, 126–130. Dalgaard, P. (1995). Qualitative and quantitative characterization of spoilage bacteria from packed fish. Int J Food Microbiol 26, 319–333. Darouiche, R. O., Smith, J. A., Jr, Hanna, H., Dhabuwala, C. B., Steiner, M. S., Babaian, R. J., Boone, T. B., Scardino, P. T., Thornby, J. I. & Raad, I. I. (1999). Efficacy of antimicrobial-impregnated bladder Kenny, J. G., Ward, D., Josefsson, E., Jonsson, I. M., Hinds, J., Rees, H. H., Lindsay, J. A., Tarkowski, A. & Horsburgh, M. J. (2009). The Staphylococcus aureus response to unsaturated long chain free fatty acids: survival mechanisms and virulence implications. PLoS ONE 4, e4344. Musk, D. J., Jr & Hergenrother, P. J. (2008). Chelated iron sources are inhibitors of Pseudomonas aeruginosa biofilms and distribute efficiently in an in vitro model of drug delivery to the human lung. J Appl Microbiol 105, 380–388. Ramos, E. R., Reitzel, R., Jiang, Y., Hachem, R. Y., Chaftari, A. M., Chemaly, R. F., Hackett, B., Pravinkumar, S. E., Nates, J. & other authors (2011). Clinical effectiveness and risk of emerging resistance associated with prolonged use of antibiotic-impregnated catheters: more than 0.5 million catheter days and 7 years of clinical experience. Crit Care Med 39, 245–251. catheters in reducing catheter-associated bacteriuria: a prospective, randomized, multicenter clinical trial. Urology 54, 976–981. Stamm, W. E. (1991). Catheter-associated urinary tract infections: epidemiology, pathogenesis, and prevention. Am J Med 91 (3B), 65S– 71S. Davies, D. G. & Marques, C. N. (2009). A fatty acid messenger is Stickler, D. J. (2008). Bacterial biofilms in patients with indwelling responsible for inducing dispersion in microbial biofilms. J Bacteriol 191, 1393–1403. Stoodley, P., Sauer, K., Davies, D. G. & Costerton, J. W. (2002). Desbois, A. P. & Smith, V. J. (2010). Antibacterial free fatty acids: activities, mechanisms of action and biotechnological potential. Appl Microbiol Biotechnol 85, 1629–1642. Desbois, A. P., Lebl, T., Yan, L. & Smith, V. J. (2008). Isolation and structural characterisation of two antibacterial free fatty acids from the marine diatom, Phaeodactylum tricornutum. Appl Microbiol Biotechnol 81, 755–764. Flemming, H. C. & Wingender, J. (2010). The biofilm matrix. Nat Rev Microbiol 8, 623–633. Fux, C. A., Costerton, J. W., Stewart, P. S. & Stoodley, P. (2005). urinary catheters. Nat Clin Pract Urol 5, 598–608. Biofilms as complex differentiated communities. Annu Rev Microbiol 56, 187–209. Takigawa, H., Nakagawa, H., Kuzukawa, M., Mori, H. & Imokawa, G. (2005). Deficient production of hexadecenoic acid in the skin is associated in part with the vulnerability of atopic dermatitis patients to colonization by Staphylococcus aureus. Dermatology 211, 240–248. Tambyah, P. A., Knasinski, V. & Maki, D. G. (2002). The direct costs of nosocomial catheter-associated urinary tract infection in the era of managed care. Infect Control Hosp Epidemiol 23, 27–31. Survival strategies of infectious biofilms. Trends Microbiol 13, 34–40. Ulett, G. C., Mabbett, A. N., Fung, K. C., Webb, R. I. & Schembri, M. A. (2007). The role of F9 fimbriae of uropathogenic Escherichia coli in Griffith, D. P., Musher, D. M. & Itin, C. (1976). Urease. The primary biofilm formation. Microbiology 153, 2321–2331. cause of infection-induced urinary stones. Invest Urol 13, 346–350. Hancock, V., Dahl, M. & Klemm, P. (2010). Abolition of biofilm Walters, M. C., III, Roe, F., Bugnicourt, A., Franklin, M. J. & Stewart, P. S. (2003). Contributions of antibiotic penetration, oxygen formation in urinary tract Escherichia coli and Klebsiella isolates by metal interference through competition for Fur. Appl Environ Microbiol 76, 3836–3841. limitation, and low metabolic activity to tolerance of Pseudomonas aeruginosa biofilms to ciprofloxacin and tobramycin. Antimicrob Agents Chemother 47, 317–323. Jennings, J. A., Courtney, H. S. & Haggard, W. O. (2012). Cis-2- Yang, L., Liu, Y., Wu, H., Song, Z., Høiby, N., Molin, S. & Givskov, M. (2012). Combating biofilms. FEMS Immunol Med Microbiol 65, 146– decenoic acid inhibits S. aureus growth and biofilm in vitro: a pilot study. Clin Orthop Relat Res 470, 2663–2670. 1516 157. Downloaded from www.microbiologyresearch.org by IP: 88.99.165.207 On: Sun, 07 May 2017 07:25:12 Journal of Medical Microbiology 63