Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
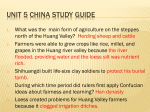
Cardiovascular Toxic Effects of Ma Huang 12 Mayo Clin Proc, January 2002, Vol 77 Original Article Adverse Cardiovascular Events Temporally Associated With Ma Huang, an Herbal Source of Ephedrine DAVID SAMENUK, MD; MARK S. LINK, MD; MUNTHER K. HOMOUD, MD; ROBERT CONTRERAS, BS; THEOHARIS C. THEOHARDES, MD; PAUL J. WANG, MD; AND N. A. MARK ESTES III, MD • Objective: To evaluate possible cardiovascular toxic effects associated with use of dietary supplements containing ma huang, an herbal source of ephedrine. • Methods: We reviewed the comprehensive database Adverse Reaction Monitoring System of the Food and Drug Administration, which included clinical records, investigative reports, and autopsy reports related to ma huang use. The main outcome measurements were stroke, myocardial infarction, and sudden death. • Results: From 1995 to 1997, 926 cases of possible ma huang toxicity were reported to the Food and Drug Administration. In 37 patients (23 women and 14 men with a mean ± SD age of 43±13 years), use of ma huang was temporally related to stroke (in 16), myocardial infarction (in 10), or sudden death (in 11). Autopsies performed in 7 of the 11 patients who experienced sudden death showed a normal heart in 1, coronary atherosclerosis in 3, and cardiomyopathies in 3. In 36 of the 37 patients, use of ma huang was reported to be within the manufacturers’ dosing guidelines. • Conclusions: Analysis of the 37 patients indicates the following findings: (1) ma huang use is temporally related to stroke, myocardial infarction, and sudden death; (2) underlying heart or vascular disease is not a prerequisite for ma huang–related adverse events; and (3) the cardiovascular toxic effects associated with ma huang were not limited to massive doses. Although the pathogenesis of the cardiac toxic effects of ma huang remains incompletely defined, available observational and circumstantial evidence indicates that use of the substance may be associated with serious medical complications. Mayo Clin Proc. 2002;77:12-16 ARMS = Adverse Reaction Monitoring System; FDA = Food and Drug Administration A t present, herbal medicines are the most common form of alternative therapy in health care.1 Retail sales of dietary supplements, including herbal products, were estimated at $3.6 billion in 1997.2 Ma huang, a popular herb derived from the genus Ephedra, is used in many of these nontraditional remedies. As a natural source of ephedrine, ma huang is taken most commonly for weight loss and energy enhancement. The increasingly widespread use of ma huang has been accompanied by the misconception that this substance has no associated serious medical consequences. However, the potential cardiovascular toxic effects of ma huang have not been evaluated systematically. According to the Dietary Supplement Health and Education Act of 1994, herbal remedies, including ma huang, must be proved “unsafe” before they can be withdrawn from the market. This law required that “the Food and Drug Administration (FDA) bear the burden of proof that a mar- keted dietary supplement presents a serious or unreasonable risk under the conditions of use on the label or as commonly consumed.”3 This approach contrasts with that for drugs in which rigorous standards of safety and efficacy must be met through appropriately designed clinical trials before the drug is available to the public. To monitor for potential toxic effects of dietary supplements, the FDA established an Adverse Reaction Monitoring System (ARMS), which collects and systematically investigates adverse and toxic effects reported with use of herbal medicines and dietary supplements. Because of the concerns regarding the safety of ma huang, we systematically examined this database to evaluate possible adverse cardiovascular effects of this substance. For editorial comment, see page 7. METHODS Via a Freedom of Information Act request, a copy of Docket No. 95N-0304 was obtained from the Dockets Management Branch of the FDA, US Department of Health and Human Services. This docket includes Adverse Event Reports associated with dietary supplements containing the ephedrine alkaloid ma huang. Adverse Event Reports enter the FDA’s passive surveillance ARMS through several means, including Drug Quality Reporting From the Cardiac Arrhythmia Service, Division of Cardiology (D.S., M.S.L., M.K.H., R.C., P.J.W., N.A.M.E.), and Department of Pharmacology and Experimental Therapeutics (T.C.T.), New England Medical Center, Boston, Mass. Address reprint requests and correspondence to N. A. Mark Estes III, MD, Cardiac Arrhythmia Service, New England Medical Center, 750 Washington St, NEMCH Box 197, Boston, MA 02111 (e-mail: [email protected]). Mayo Clin Proc. 2002;77:12-16 12 © 2002 Mayo Foundation for Medical Education and Research For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings. Mayo Clin Proc, January 2002, Vol 77 System, MedWatch program, US Pharmacopeia, FDA’s field offices through the Office of Regulatory Affairs, Consumer Complaint System (FDA Form 2516), written and electronic correspondence, and written documentation of telephone conversations. Data were collected from January 1995 to January 1997. The clinical research and review staff in the Office of Special Nutritionals is responsible for the tracking and reviewing of Adverse Event Reports. Only Adverse Event Reports associated with an illness or injury are included. Reports of product quality or consumer dissatisfaction are not included. For the current study, detailed information relevant to each Adverse Event Report file was reviewed, including medical records, autopsy reports, affidavits from the Consumer/ Health Professional, Consumer Complaint Illness/Injury Report (FDA Form 2516), Complaint/Injury Follow-up (FDA Form 2516a), MedWatch report (FDA Form 3500), Investigative Memoranda, Collection Report (FDA Form 464), Adverse Reaction Information Form A or Adverse Reaction Questionnaire (Form A), Ephedrine Consumer Hotline Questionnaire, correspondence related to the Adverse Event Report, Sample Summary (FDA Form 465), and product labeling.4 Inclusion criteria for this study were adverse cardiovascular events defined as sudden death, myocardial infarction, or stroke in association with ma huang use reported to the FDA through ARMS. Sudden death was defined as death occurring within 1 hour of symptoms and/or unwitnessed death.5 The diagnosis of myocardial infarction was based on the World Health Organization definition and included the presence of at least 2 of the following 3 criteria: (1) a clinical history of ischemic-type chest discomfort, (2) changes on serially obtained electrocardiographic tracings, and (3) abnormal serum cardiac enzymes.6 Stroke was characterized by a history of rapid onset of localizing neurologic deficit and/or change in state of consciousness with documentation by computed tomography that showed no definite signs of any disease process or event causing focal brain deficit or coma other than cerebral infarction or hemorrhage.6 Suspected cases of ma huang toxicity with inadequate documentation were excluded as were cases in which the records indicated use of any illicit substance. RESULTS Of the 926 cases of possible ma huang toxicity reported to the FDA from 1995 to 1997, 37 involved serious cardiovascular events; 11 sudden deaths (1 resuscitation), 16 strokes (including 3 deaths), and 10 myocardial infarctions were temporally related to ma huang use (Table 1). The mean ± SD age of the 23 women and 14 men was 43±13 years (range, 20-69 years). Reasons for using ma huang were Cardiovascular Toxic Effects of Ma Huang 13 Table 1. Adverse Cardiovascular Events Temporally Related to Ma Huang Use Adverse events No. of patients Mean ± SD age (y) Sudden death Myocardial infarction Stroke 7 M, 4 F 3 M, 7 F 4 M, 12 F 40±14 44±14 44±13 weight loss, energy enhancement, bodybuilding, and recreational. Prior cardiovascular disease was reported in only 1 of the 37 patients. A review of clinical records and investigative interviews indicates that 36 of the patients used ma huang according to the manufacturers’ recommendations. A 20-year-old man died suddenly after ingesting 2 times the manufacturer’s recommended dosage. No patient had a clinical history or toxicologic data to indicate use of any other substance. Of the 37 patients, 33 (89%) used ma huang for more than 1 week, and 27 (73%) used it for more than 1 month. Of the 11 patients who experienced sudden death, 7 were men, and 4 were women. The mean ± SD age of this group was 40.4±14.4 years (range, 20-63 years). In these 11 patients, 7 autopsies demonstrated a normal heart in 1, atherosclerosis (defined as ≥70% luminal stenosis) of a major epicardial coronary artery in 3, and cardiomyopathies in 3 (Table 2). Of the 10 patients with myocardial infarction, 7 (70%) were women, and 3 (30%) were men; the mean ± SD age was 44.2±13.8 years (range, 23-67 years). Of these patients, 8 used ma huang for weight loss. Of the 10 patients with myocardial infarctions, 8 underwent cardiac catheterization, with normal findings in 3, obstructive coronary artery disease in 4, and a dissection of the circumflex artery in 1. The mean ± SD creatine kinase level was 1509±914 U/L, and mean ± SD creatine kinase–MB fraction was 85.6±40.6 U/L. Of the 16 patients who suffered a stroke, 12 (75%) were women, and 4 (25%) were men; the mean ± SD age was 43.6±13.0 years (range, 24-69 years). Eleven (69%) of these patients used ma huang for weight loss. Of these 16 patients, 12 (75%) had an ischemic stroke, and 4 (25%) had a hemorrhagic stroke. DISCUSSION Our study findings provide evidence that ma huang may precipitate life-threatening cardiovascular events, and they expand on observations from other reports.8-11 Because of the absence of appropriately designed toxicity trials and absence of rechallenges in any of the surviving patients, the cases presented in this report must be interpreted as demonstrating only a temporal, not causal, relationship between ma huang and adverse cardiovascular events. For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings. 14 Cardiovascular Toxic Effects of Ma Huang Table 2. Autopsy Findings in 7 Patients Who Experienced Sudden Death* Age (y)/ sex Cardiac pathology 20/M Normal 23/M Multifocal and confluent myocyte necrosis with healing of approximately 1 to 2 weeks; mild perivascular, focal endocardial, and local epicardial fibrosis; and moderate myocyte hypertrophy and vascular congestion. No evidence of myocarditis. Myocyte necrosis findings are nonspecific and could be due to primary myocyte toxicity or secondary to ischemia. The peculiar distribution of the necrosis as a band in the subepicardial one third of the myocardium contrasts with the typical subendocardial distribution of myocardial damage associated with large coronary vascular obstructions. This finding, the myocardial hemorrhage, and the observed single, few cell necrotic areas certainly are consistent with effects of factors that collectively could be responsible for vascular damage, vasoconstriction of small arterial vessels, and myocyte toxicity. Variable duration of lesions suggests multiple/ongoing insults. These pathologic features are reminiscent of experimental and clinical aspects of adrenergic/sympathomimetic agents† 29/F Greater than or equal to 90% stenosis of left main, left circumflex, left anterior descending, and right coronary arteries 32/M Mild chronic inflammation and focal fibrosis of the epicardium. Widespread, focally severe necrotizing interstitial myocarditis involving the intraventricular septum and all sections of the left ventricle, sparing the right ventricle. Infiltration of these areas is composed of neutrophils and macrophages, with rare eosinophils. Monocytes and nuclei show moderate hypertrophy, and intramural arteries show moderate and focally severe thickening of the walls. Heart weight, 600 g 37/M Myocardial hypertrophy, focal interstitial fibrosis, mild focal disarray of myocardial fibers, and mild medial hypertrophy of the intramyocardial small arteries 38/M Greater than 75% stenosis of the obtuse marginal, 50% of the left anterior descending, 75% of the proximal right coronary artery, and 75% of the proximal left circumflex coronary artery. Cardiomegaly (heart weight, 490 g) 45/M Approximately 50% stenosis of the proximal left anterior descending coronary artery with acute intracoronary thrombus *Data from Adverse Reaction Monitoring System database. †Autopsy report from Backer et al.7 Mayo Clin Proc, January 2002, Vol 77 Another analysis of FDA adverse events during a different period (June 1997-March 1999)10 similarly concluded that dietary supplements containing ephedra alkaloids may pose a health risk.8 Among 140 reported adverse effects related to the use of dietary supplements containing ma huang, 47% involved the cardiovascular system and 18% the central nervous system.8 The pathogenesis of ma huang toxicity remains incompletely defined. Ma huang (Ephedra) has been used in traditional Chinese medicine for more than 5 millennia.12 The approximately 40 species of herbs in the genus Ephedra are divided into several geographic types and vary qualitatively and quantitatively in their alkaloid content.12 Commercially available ma huang varies considerably in ephedrine alkaloid content.12,13 Many products do not list ephedrine content on the label.13,14 A recent determination of the content of alkaloids in 20 herbal dietary supplements containing ma huang showed that alkaloid content often differed markedly from label claims and was inconsistent between 2 lots of the same products. Total alkaloid content ranged from 0.0 to 18.5 mg per dosage unit.13,14 Ranges for ephedrine and pseudoephedrine were 1.1 to 15.3 mg and 0.2 to 9.5 mg per unit dose, respectively. Norpseudoephedrine, a schedule 4 controlled substance, was often present.14 Substantial lot-to-lot variations in alkaloid content were observed for multiple products. This included lotto-lot variation of ephedrine, pseudoephedrine, and methylephedrine that exceeded 180%, 250%, and 100%, respectively. Analysis of 1 product showed no detectable ephedra alkaloid. Similar analysis of other nutraceuticals, including melatonin, dehydroepiandrosterone, ginseng, feverfew, and kava, documented substantial deviations in content from the product label.13,14 Botanical supplements have been contaminated with harmful herbs, undeclared conventional pharmaceuticals, or heavy metals.3,14 These observations raise questions regarding the adequacy of self-regulation for product quality, consistency, potency, and purity within the nutraceutical industry. Although the association of ma huang use and cardiovascular toxic effects in our study is circumstantial, a considerable body of knowledge is available on the potential and similar toxic effects of ephedrine, the active alkaloid in ma huang. Ma huang increases the availability of naturally released catecholamines at synaptic areas in the brain and in the heart and directly stimulates α- and β-adrenergic receptors.15 As a result, ma huang increases blood pressure secondary to elevations in heart rate, cardiac output, and peripheral resistance.16 Ephedrine is well absorbed after oral administration and is excreted primarily unchanged in the urine, with a serum half-life of 2.7 to 3.6 hours.17 The therapeutic index for ephedrine is low, with toxic effects reported with both short-term and long-term use.17 Ephed- For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings. Mayo Clin Proc, January 2002, Vol 77 rine has been previously reported to be associated with both ischemic and hemorrhagic stroke.18 In addition, combinations with other common stimulants, such as caffeine, have been associated with cardiac arrhythmias including ventricular tachycardia.19 Coronary artery vasospasm has been documented with ephedrine administration during spinal anesthesia.20,21 Intravenous ephedrine has been linked to acute myocardial infarction.22 Sudden death resulting from an ephedrine overdose has been reported.7 Long-term ephedrine use may lead to a cardiomyopathy typically seen with catecholamine excess.23,24 The serious adverse reactions associated with ma huang ingestion documented in the current study are consistent with those previously reported with ephedrine toxicity. Cases in which a reasonable alternative explanation was possible for the cardiovascular events were excluded from our study. The pathophysiology for such devastating complications may be related to intense vasoconstriction in both cerebral and coronary arteries, similar to that seen with ephedrine and also with cocaine.25 Toxic effects of ephedrine may be related to ischemia secondary to sudden increases in myocardial oxygen requirements. Long-term ephedrine use may lead to conditions seen with prolonged catecholamine excess resulting in fibrosis and even death.26 In the current study, ma huang was associated with sudden death even in the absence of structural heart disease. In addition, a substantial proportion of patients were young and had no other risk factors for cardiovascular disease, such as diabetes, hypertension, smoking, or family history of cardiovascular diseases. The mean age of patients who experienced these adverse events was young compared to those who typically experience stroke, myocardial infarction, or sudden death. This observation may be related to the greater proportion of younger people choosing alternative therapies27 and the marketing of these agents for younger people. Importantly, in 36 of the 37 patients in this report, use of ma huang was reported to be within the manufacturers’ recommended dosing. The exact number of people in the United States who use ma huang is unknown. An estimated 12 million persons in the United States consumed products containing ma huang in 1999.8 Adverse effects of drugs are underreported, with reporting rates lower than 15%.8 The reporting rate for adverse reactions to nutraceuticals is believed to be even lower.8 Accordingly, it is not possible to know precisely the proportion of people taking ma huang who are at risk. Despite this limitation, the adverse effects of ma huang documented in this report and others raise several issues regarding the risk of this agent, which has no scientifically proven benefit.8 The cases presented herein cannot be used to establish the frequency of adverse reactions because of almost certain underreporting of adverse events. However, Cardiovascular Toxic Effects of Ma Huang 15 these cases can serve as a reminder of the potential toxic effects of ma huang to both the medical community and to the people who consume ma huang. Our report has the limitation of being an observational study and as such does not definitively establish the relationship between ma huang use and the risk of adverse cardiovascular events. In August 1997, a small observational study reported on the association of fenfluramine and phentermine use and cardiac valvular regurgitation.28 That report had limitations similar to our observations regarding potential ma huang toxicity.28 In the year preceding the report on valvular abnormalities in association with anorectic agents, the number of prescriptions written for these agents in the United States exceeded 18 million. Although not approved by the FDA for combination use, these drugs were commonly used together. Within 3 weeks of the publication by Connolly et al28 before more definitive investigations were conducted, fenfluramine and dexfenfluramine were withdrawn from the market at the request of the FDA. Population-based follow-up studies, case-control investigations, and analyses of a double-blind, placebo-controlled study were performed to assess the incidence and prevalence of these cardiac valvular findings.29-31 The subsequent studies ultimately concluded that these anorectic agents are associated with an increased risk of newly diagnosed cardiac valve disorders.29-31 Neither the small observational study by Connolly et al28 nor our report on ma huang use definitively establishes a causal relationship between the respective agents and the observed adverse cardiovascular events. Additionally, these reports provide no insight on the potential biologic mechanisms of the adverse effects of ma huang or the combined anorectic agents. However, like the cases of fenfluraminephentermine, our observations raise important public health issues that warrant further research. Persons using or considering using ma huang should be informed of the possibility of associated serious adverse cardiovascular effects. REFERENCES 1. 2. 3. 4. 5. 6. Brody JE. Alternative medicine makes inroads, but watch out for curves. New York Times. April 28, 1998:F7. Canedy D. Real medicine or medicine show? growth of herbal remedy sales raises issues about value. New York Times. July 23, 1998:D1. Slifman NR, Obermeyer WR, Aloi BK, et al. Contamination of botanical dietary supplements by Digitalis lanata. N Engl J Med. 1998;339:806-811. Food and Drug Administration. Docket No. 95N-0304. Rockville, Md: Food and Drug Administration; 1995. Hinkle LE Jr, Thaler HT. Clinical classification of cardiac deaths. Circulation. 1982;65:457-464. Gillum RF, Fortmann SP, Prineas RJ, Kottke TE. International diagnostic criteria for acute myocardial infarction and acute stroke. Am Heart J. 1984;108:150-158. For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings. 16 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. Cardiovascular Toxic Effects of Ma Huang Backer R, Tautman D, Lowry S, Harvey CM, Poklis A. Fatal ephedrine intoxication. J Forensic Sci. 1997;42:157-159. Haller CA, Benowitz NL. Adverse cardiovascular and central nervous system events associated with dietary supplements containing ephedra alkaloids. N Engl J Med. 2000;343:1833-1838. Zahn KA, Li RL, Purssell RA. Cardiovascular toxicity after ingestion of “herbal ecstacy.” J Emerg Med. 1999;17:289-291. Zaacks SM, Klein L, Tan CD, Rodriguez ER, Leikin JB. Hypersensitivity myocarditis associated with ephedra use. J Toxicol Clin Toxiol. 1999;37:485-489. Theoharides TC. Sudden death of a healthy college student related to ephedrine toxicity from a ma huang-containing drink [letter]. J Clin Psychopharmacol. 1997;17:437-439. Tyler VE. The Honest Herbal: A Sensible Guide to the Use of Herbs and Related Remedies. 3rd ed. New York, NY: Pharmaceutical Products Press; 1993:119-120. Gurley BJ, Wang P, Gardner SF. Ephedrine-type alkaloid content of nutritional supplements containing Ephedra sinica (ma-huang) as determined by high performance liquid chromatography. J Pharm Sci. 1998;87:1547-1553. Gurley BJ, Gardner SF, Hubbard MA. Content versus label claims in ephedra-containing dietary supplements. Am J Health Syst Pharm. 2000;57:963-969. Sapru HN, Theoharides TC. Autonomic nervous system. In: Theoharides TC, ed. Essentials of Pharmacology. 2nd ed. Boston, Mass: Little, Brown; 1996:58. Hoffman BB, Lefkowitz RJ. Catecholamines, sympathomimetic drugs, and adrenergic receptor antagonists. In: Hardman JG, Limbird LE, Molinoff PB, Ruddon RW, Gilman AG, eds. Goodman & Gilman’s The Pharmacological Basis of Therapeutics. 9th ed. New York, NY: McGraw-Hill; 1996:221. Pentel P. Toxicity of over-the-counter stimulants. JAMA. 1984; 252:1898-1903. Bruno A, Nolte KB, Chapin J. Stroke associated with ephedrine use. Neurology. 1993;43:1313-1316. Weesner KM, Denison M, Roberts RJ. Cardiac arrhythmias in an adolescent following ingestion of an over-the-counter stimulant. Clin Pediatr (Phila). 1982;21:700-701. Mayo Clin Proc, January 2002, Vol 77 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. Hirabayashi Y, Saitoh K, Fukuda H, Mitsuhata H, Shimizu R. Coronary artery spasm after ephedrine in a patient with high spinal anesthesia. Anesthesiology. 1996;84:221-224. Lustik SJ, Chhibber AK, van Vliet M, Pomerantz RM. Ephedrineinduced coronary artery vasospasm in a patient with prior cocaine use. Anesth Analg. 1997;84:931-933. Cockings JG, Brown M. Ephedrine abuse causing acute myocardial infarction. Med J Aust. 1997;167:199-200. Van Mieghem W, Stevens E, Cosemans J. Ephedrine-induced cardiopathy [letter]. BMJ. 1978;1:816. To LB, Sangster JF, Rampling D, Cammens I. Ephedrine-induced cardiomyopathy. Med J Aust. 1980;2:35-36. Isner JM, Estes NA III, Thompson PD, et al. Acute cardiac events temporally related to cocaine abuse. N Engl J Med. 1986;315:14381443. Reichenbach DD, Benditt EP. Catecholamines and cardiomyopathy: the pathogenesis and potential importance of myofibrillar degeneration. Hum Pathol. 1970;1:125-150. Eisenberg DM, Kessler RC, Foster C, Norlock FE, Calkins DR, Delbanco TL. Unconventional medicine in the United States: prevalence, costs, and patterns of use. N Engl J Med. 1993;328: 246-252. Connolly HM, Crary JL, McGoon MD, et al. Valvular heart disease associated with fenfluramine-phentermine. N Engl J Med. 1997; 337:581-588. Weissman NJ, Tighe JF Jr, Gottdiener JS, Gwynne JT, SustainedRelease Dexfenfluramine Study Group. An assessment of heartvalve abnormalities in obese patients taking dexfenfluramine, sustained-release dexfenfluramine, or placebo. N Engl J Med. 1998; 339:725-732. Jick H, Vasilakis C, Weinrauch LA, Meier CR, Jick SS, Derby LE. A population-based study of appetite-suppressant drugs and the risk of cardiac-valve regurgitation. N Engl J Med. 1998;339:719724. Khan MA, Herzog CA, St. Peter JV, et al. The prevalence of cardiac valvular insufficiency assessed by transthoracic echocardiography in obese patients treated with appetite-suppressant drugs. N Engl J Med. 1998;339:713-718. For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.