Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
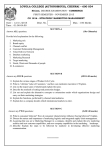
2003.1 VAQ 2 Radiology 021 CJJ-02 Scenario A head CT scan of an 83 year old woman has been performed, who has presented with a 3 day history of increasing confusion and unsteady gait following a fall. Her GCS is 12 (M5, V3, E4). 1. Mention 3 salient features of this CT scan 2. Describe 5 different factors you will consider while managing the case 2003.1 VAQ 2 Radiology 021 CJJ-02 Scenario A head CT scan of an 83 year old woman has been performed, who has presented with a 3 day history of increasing confusion and unsteady gait following a fall. Her GCS is 12 (M5, V3, E4). 1. Mention 3 salient features of this CT scan a. Presence of old and new bleed in the sub dural space and intraventricular bleed b. Significant midline shift with effacement of the ventricle c. Signs of the raised intracranial pressure 2. Describe 5 different factors you will consider while managing the case a. Age (83 female) and premorbid functional state b. Patient Wishes – previous Advanced Health Directive, ARP etc. c. Consultation with NOK, POA- relatives and family physician. d. Hunt and Hess grading/Fisher scale: Based on CT (ref. to tables respectively) e. Neurosurgical consultation f. Blood pressure control, g. Prevention of Hypoxia , stopping of Warfarin , ICP control etc GR GCS Motor Survival Rate I 15 0 70% II 14-13 0 60% III 14-13 Y IV 12-7 V 6-3 CR CT findings 1 No Blood 2 Different deposition, No clots, No layers > 1mm 50% 3 Clots (+) >1mm Y/N 40% 4 Y/N 10% Intracerebral/intervertebral clots Figure 2 Hunt -Hess Grading Figure 1 Fisher Scale ( based on CT ) 2003:1 VAQ 7 CJJ 7 This 12 year old boy was a back seat passenger in a high speed road traffic accident. a. Describe 3 features of this fracture? What is the name of this fracture? b. What associated injuries should be sought for in this patient? c) What is the mechanism of this injury? 2003:1 VAQ 7 CJJ 7 This 12 year old boy was a back seat passenger in a high speed road traffic accident. a. Describe 3 features of this fracture? What is the name of this fracture? It is a Chance fracture b. 1) Transverse fracture through the vertebral bodies 2) Fracture through neural arch 3) Occurs at the thoracolumbar junction What associated injuries should be sought for in this patient? Intrabdominal inuries (pancreatic, small bowel, ) Spinal cord injuries c) What is the mechanism of this injury? It’s a flexion distraction injury. Shows widening of the interspinous interval resulting from improperly wearing seatbelt most commonly. In this case not sitting on a booster seat could be problem if the child is smaller size. Question 5 A 48 year old man presents to your emergency department via ambulance following a syncopal episode. He is confused with a GCS of 12 (E3V4M5). His observations otherwise are within normal limits. He has had a CT scan of his head performed. a) What does his CT show b) What features would you seek on history from this man Question 5 A 48 year old man presents to your emergency department via ambulance following a syncopal episode. He is confused with a GCS of 12 (E3V4M5). His observations otherwise are within normal limits. He has had a CT scan of his head performed. a) What does his CT show - Extra-axial, unilateral mass of mixed attenuation typical of an extradural hematoma b) - What features would you seek on history from this man Trauma Blood thinners Epilepsy Alcohol abuse Bleeding diathesis Co-morbidities SAQ Question 1 A patient presents with neck pain following a motor vehicle crash. a) Outline 2 rules you could use to clear this patients c-spine - - Nexus o o o o No midline c-spine pain Nil ALOC/Intoxication Nil focal neurology Nil distracting injuries Canadian c-spine rules o Can be used for any patients with GCS 15 in stable trauma patients o Any high risk factors that mandates radiography? Then Can’t clear Age >65 Dangerous mechanism Fall from elevation >5 stairs/3 feet Axial load to head MVC high speed >100km/hr Rollover, ejection Motorized recreational vehicles Bike crash Paraesthesias in extremities o Any low-risk factor that allows safe assessment of range of motion if no can’t clear c-spine Simple rear end MVC Sitting position in ED Ambulatory at any time Delayed onset of neck pain Absence of midline cervical spine tenderness o Able to actively rotate neck left and right – yes and no high risk factors and low risk factors present then clear Question 5 A 72 year old patient presents to the ED with acute left hemiparesis a) What is your DDx? b) What is the rationale for thrombolysis c) Indications for thrombolysis d) List 2 factors associated with increased hemorrhagic risk Question 5 A 72 year old patient presents to the ED with acute left hemiparesis a) What is your DDx? Ischaemic stroke Haemorrhagic stroke TIA SOL Subdural hematoma Brain abscess Postictal neurological deficit – Todd’s paraesis Encephalitis Metabolic or drug induced Hyopglycaemia MS Migraine b) What is the rationale for thrombolysis Following onset of stroke, neurons surrounding ischaemic core may remain viable for a period of time Early correction of ischaemic may rescue these neurons in the ischaemic penumbra Thrombolysis may degrade clot and relieve ischaemia (alteplase acts by converting inactive plasminogen into the active form plasmin which promotes thrombolysis) c) Indications for thrombolysis Positive trials: NINS, IST3, ECASS III Acute ischemic CVA within 3 hours of onset after exclusion of hemorrhage d) List 2 factors associated with increased hemorrhagic risk Increased age especially >80 Increased severity of stroke Early CT changes of large ischemic stroke 20010.1 VAQ 8 Radiology Quiz 027 Scenario An 11 year old boy has an isolated head injury after falling from a skateboard 10 hours ago. He has a GCS of 4 with decerebrate posturing. Q1) describe the features of this CT scan Q2) What immediate steps will you take for this young boy ? 20010.1 VAQ 8 Radiology Quiz 027 Scenario An 11 year old boy has an isolated head injury after falling from a skateboard 10 hours ago. He has a GCS of 4 with decerebrate posturing. Q1) describe the features of this CT scan a) b) c) d) Axial CT head with left sided extradural hematoma measuring approx. 3cm at the max diameter. >1 cm midline shift Ventricular effacement Dilatation of the contralateral ventricle suggesting early hydrocephalous due to obstruction of the duct aqueduct of Sylvius or interventricular foramen. e) No obvious skul;l fracures seen f) No swirl sign ( over 10 hours ago therefore no fresh blood seen ) Q2) What immediate steps will you take for this young boy ? 1) 2) 3) 4) 5) 6) 7) 8) Activate the trauma team Primary survery & resuscitation Airway intubate RSI – prevent hypotension & hypoxia Ventilation rate higher than normal 15lit/min , PaCO2 35+/_2, Rate 18-24/min Target MAP 70mm of Hg Raise head Steps to reduce ICT 0.25 to 1 gm iv bolus Mannitol or 3% saline Urgent Neurosurgery intervention or if unavailable do Burr hole under Neurosurgery guidance in the ipsilateral side Question 6 A 30 year old man undergoes a lumbar puncture in the emergency department for investigation of fever, headache, and vomiting. His lumbar puncture results are shown below a) Describe the results (3 marks) b) What potential organisms can be responsible for this picture? (4 marks) c) Outline further investigations you may consider in order to identify the cause of these findings. (4 marks) Question 6 Answers a) Describe the results (4 marks) Moderately elevated opening pressure most consistent with infective meningitis. o DDx: Benign intracranial hypertension, space occupying lesion, abscess Turbid appearance indicating elevated red cell and white cell counts in CSF, most consistent with infective meningitis. Moderately elevated leucophilia with lymphocytic predominance consistent with viral meningitis. Mildly elevated RBC likely due to traumatic tap. Marked elevation of CSF protein also indicative of meningitis. o DDx; Space occupying lesion, polyneuritis Low CSF glucose indicative of likely diffuse meningeal inflammation (ie early bacterial meningitis or partially treated bacterial meningitis) o Would expect CSF glucose to be 60-80% of serum glucose o CSF to serum glucose ratio < 0.4 consistent with bacterial meninitis o Would expect CSF glucose to be normal in viral meningitis Negative gram stain shows no responsible organisms to date identified. b) What potential organisms can be responsible for this picture? (4 marks) Bacterial Meningitis Neisseria meningitides Streptococcus pneumoniae Listeria Klebsiella pneumoniae Staph aureus If immunocompromised: E.Coli Viral Meningitis Enteroviruses Herpes simplex Echovirus Varicella zoster virus Epstein Barr virus Others Mycobacterium turberculosis Fungal (Cryptococcus) in the immunocompromised c) Please outline the treatment of query meningitis. (3 marks) Antibiotics: Ceftriaxone 2g IV and Benzylpenicillin 2.4g IV Consideration of acyclovir 10mg/kg IV to cover viral causes. Steroids with IV dexamethasone up to 10mg IV prior to first dose of antibiotics. Admission for continual IV antimicrobials and to await CSF culture to further rationalize treatment with antibiotics. References Dunn’s page 657: Lumbar puncture Cameron’s page 434: Meningitis SAQ 3 A two year old boy has been brought into your tertiary level ED after falling off the top level of a bunk bed three hours ago. He hit his head on wooden floorboards. He is presently alert, but wanting to sleep on his mother’s lap. a. What features on further history would make you consider scanning this child’s head rather than just observing them? (3 marks, ½ mark per answer, must have bold answers) b. What features on examination would make you consider scanning their head? (2 marks) SAQ 3 A two year old boy has been brought into your tertiary level ED after falling off the top level of a bunk bed three hours ago. He hit his head on wooden floorboards. He is presently alert, but wanting to sleep on his mother’s lap. c. What features on further history would make you consider scanning this child’s head rather than just observing them? (3 marks, ½ mark per answer, must have bold answers) LOC > 5mins Abnormal drowsiness 3 or more vomits following head injury Suspicion of NAI Seizure after head injury in a non epileptic patient Amnesia (retrograde/anterograde) > 5mins duration (but a 2 year old might not be able to convey amnesia!) Mechanism – fall from over 3m is the Chalice rule, but this is still potentially almost a 2m fall d. What features on examination would make you consider scanning their head? (2 marks) GCCS <14 Suspicion of penetrating injury – unlikely from falling onto floor Suspicion of depressed skull fracture eg boggy haematoma– possible with fall from this height Signs of BOS fracture Any focal neurological deficit/abnormality Chalice also includes tense fontanelle, but this child is too old for that to be a feature 2. A 28 year old woman (G1P1) presents to the Emergency Department with a 12 hour history of headache. She delivered a healthy baby one week ago. Her pregnancy was unremarkable. Her vital signs are: P 85 beats/min (regular) BP 145/95 mmHg RR 14 /min SaO2 99 % on air Temp 37C a) List 4 differential diagnoses (4 marks) b) List your possible investigations and their clinical indications (4 marks) Investigation Indication 2. A 28 year old woman (G1P1) presents to the Emergency Department with a 12 hour history of headache. She delivered a healthy baby one week ago. Her pregnancy was unremarkable. Her vital signs are: P 85 beats/min (regular) BP 145/95 mmHg RR 14 /min SaO2 99 % on air Temp 37C a) List 4 differential diagnoses (4 marks) Pre-eclampsia Common primary headache: Migraine/tension headache Acute vascular emergency CNS infection b) List your possible investigations and their clinical indications (4 marks) Investigation Indication Urine Proteinuria FBC Platelets (HELLP), WCC/neutrophilia or neutropaenia (inflammatory) LFT HELLP CT head If focal neurology, decreased GCS, possible SAH and concerns of raised ICP or seizures LP Possible meningitis with no CI or ? SAH with negative CT 1. A 48 year old man is brought by ambulance to your tertiary emergency department following a collapse at home. GCS on arrival is 3. He is immediately intubated and ventilated before CT scanning of his head and neck. CT reveals a massive intraparenchymal haemorrhage with obstructive hydrocephalus. The neck CT scan is normal. He was previously well on no medication. His partner is present and requests information about his treatment and prognosis. His observations are: HR 60 beats/min (regular) BP 180/110 mmHg O2 Saturation 100 % (FIO2 1.0) Temperature 36.3 oC a) What are pertinent aspects to consider in your discussion with the partner? b) List your immediate treatment priorities. c) Discuss briefly your disposition options. 1. A 48 year old man is brought by ambulance to your tertiary emergency department following a collapse at home. GCS on arrival is 3. He is immediately intubated and ventilated before CT scanning of his head and neck. CT reveals a massive intraparenchymal haemorrhage with obstructive hydrocephalus. The neck CT scan is normal. He was previously well on no medication. His partner is present and requests information about his treatment and prognosis. a) What are pertinent aspects to consider in your discussion with the partner? - - Private room with comfortable seating Access to telephone, tissues, and refreshments Full, clear, direct communication o No jargon o Explanation of diagnosis o Explanation of likely trajectory (i.e. futile) o Explanation of treatment options available Gentle probing for any previously identified end-of-life wishes/advanced planning o Especially cultural/spiritual Offer of support to contact other family members b) List your immediate treatment priorities. - early consultation with neurosurgery, social worker, anaesthetics and ICU - seek and treat coagulopathy (at risk of DIC) - management of raised ICP: o o o o o posture: elevate head of bed 30deg remove c-collar / sandbags ensure ETT ties loosened airway: maintain PaO2 ~100 hyperventilate aiming for PaCO2 35 ensure adequate sedation/analgesia/paralysis avoid excessive suctioning of ETT circulation: target: MAP > 80, CVP 0-2 hyperosmolar therapy: Mannitol: 0.5-1g/kg of 20% over 1hour hypertonic saline recommended over mannitol in ICH - 150mL of 3% saline; or 30mL 23% saline supportive therapies: euglycaemia normothermia euvolaemia eunatraemia seizure prophylaxis c) Discuss briefly your disposition options. ICU – if ongoing support in preparation for donation, or further decision-making required OT – if NROS think non-futile and partner keen ED – only if withdrawal of Rx and palliative measures pursued, AND partner happy 1. A 25 year old man is brought to your emergency department, which has an acute neurosurgical service, following an assault. He has an isolated head injury. His GCS on arrival to the ED was 14 (E4, M6, V4) A CT head is performed. On return from CT his observations are: GCS 11 (E3, M5, V3) HR 60 beats/min RR 16 /min BP 150/80 /mmHg a) List 5 findings on this CT. b) List 3 key treatment measures required for this man, and your rationale for each. Treatment Rationale 1. A 25 year old man is brought to your emergency department, which has an acute neurosurgical service, following an assault. He has an isolated head injury. His GCS on arrival to the emergency department was 14 (E4, M6, V4) A CT head is performed. On return from CT his observations are: GCS 11 (E3, M5, V3) HR 60 beats/min RR 16 /min BP 150/80 /mmHg a) List 5 findings on this CT. air in soft tissues large scalp haematoma overlying the right frontoparietotemporal area large extradural haematoma in the right frontal area depressed/displaced skull fracture of the R frontal bone signs of mass effect/raised ICP obliteration of ventricles, effacement of sulci/loss of fissure space/mild midline shift evidence of contracoup injury Frontal reactive oedema non-uniform appearance of haematoma suggesting active bleeding b) List 3 key treatment measures required for this man, and your rationale for each. Treatment Rationale Urgent neurosurgical intervention reduces mortality and severe disability in adults if performed within 6 hours of injury Intubation and ventilation Pro-active measure in light of falling GCS, ensures adequate oxygenation; enables tight pCO2 control Hyperosmolar therapy hyperosmolar agents exert their effect by removing water from remaining normal brain tissue in proportion to the volume of undamaged brain tissue, thus decreasing ICP (Dunn p140) 6. A 21 year old man is brought to the emergency department by ambulance after an MVA rollover where he was the unrestrained driver. His observations are: GCS 8 (E2, M4, V2) BP 80/50 mmHg HR 50 beats/min O2 Saturation 91 % on 15 L/min O2 via non-rebreather mask Lateral cervical spine X-ray is shown. a) List three key features seen on this man’s XR b) Define ‘neurogenic shock’ c) Outline the main features of neurogenic shock. 6. A 21 year old man is brought to the emergency department by ambulance after an MVA rollover where he was the unrestrained driver. His observations are: GCS 8 (E2, M4, V2) BP 80/50 mmHg HR 50 beats/min O2 Saturation 91 % on 15 L/min O2 via non-rebreather mask Lateral cervical spine X-ray is shown. a) List three key features seen on this man’s XR - posterior shift of C5 on C6 - displaced anterior fracture of C5 - inadequate view and need for further imaging - disrupted spino-laminal line - soft tissue swelling seen in in prevertebral space - not intubated - no hard collar visible b) Define ‘neurogenic shock’ “state of hypoactivity of the sympathetic nervous system in patients with quadriplegia or high paraplegia” (Dunn p1159) c) Outline the main features of neurogenic shock. • bradycardia (HR usually 50 - 60 /min) • hypotension (systolic BP usually 90-100 mmHg) • poikilothermia • Associated with : flaccid paralysis of skeletal muscle, paralytic ileus, flaccid paralysis of bladder - (Dunn p1159) Question 4 A 25 year old male was assaulted with a baseball bat. He had a witnessed LOC for 5 minutes and GCS was 10 when paramedics attended. On arrival to the ED, he had a generalised seizure following which he became agitated and combative with a GCS of 8. His left pupil is dilated and he has already vomited at scene and the ED. R L 1. Describe the 4 abnormalities on this CT (2 marks) 2. List 9 important initial steps in this patient’s initial primary survey, including end points where appropriate (6 marks) 3. Describe the methods of reducing intracranial pressure in this patient and the rationale of each method (2 marks) Question 4 Answer A 25 year old male was assaulted with a baseball bat. He had a witnessed LOC for 5 minutes and GCS was 10 when paramedics attended. On arrival to the ED, he had a generalised seizure following which he became agitated and combative with a GCS of 8. His left pupil is dilated and he has already vomited at scene and the ED. R L 1. Describe the 4 abnormalities on this CT (2 marks) midline shift acute left subdural haemorrhage acute right extradural haemorrhage left frontal intracerebral haemorrhage 2. List 9 important initial steps in this patient’s initial primary survey, including end points where appropriate (6 marks) secure the airway/ intubate C-spine immobilisation maintain normoxaemia PO2 100mmHg ventilate to maintain PCO2 35-40mmHg secure IV access, crystalloids to maintain MAP >65mmHg, SBP > 90mmHg inotropes noradrenaline once fluid deficit corrected to maintatin MAP>65 maintain normoglycaemia normothermia phenytoin loading dose to minimise early seizures/ secondary brain injury NB score 2 marks for each 3 steps named 3. Describe the methods of reducing intracranial pressure in this patient and the rationale of each method (2 marks) hyperventilation – temporary vasoconstriction at the expense of cerebral perfusion prior to theatre mannitol – 0.25 1.0g/kg – osmotic gradient, can be detrimental with disrupted blood brain barrier or cardiovascular instability hypertonic saline head elevation 30 degrees optimise cerebral venous drainage NB need to describe 4 methods to score 2 marks Question 5 Answer Dr Ien Ly A 45 year-old female has long standing low back pain was discharged the preceding day by a JMO in your ED with a diagnosis of malingering. She now presents to the ED with a sudden and severe lower back pain radiating down the legs. In the department she was unable to control herself and was incontinent of urine. 1. What 6 features would suggest cauda equina syndrome? (3 marks) 2. List the essential test to aid the assessment of a patient with suspected cauda equina syndrome (1 mark) 3. You investigate and find that the JMO did not examine the patient, wrote no notes and was heard by the ED RN to tell the patient that there is nothing wrong with them and they should not have come to the ED, again. You are the JMO’s supervisor. Outline your approach to this situation (4 marks) 4. Outline the immediate steps in the management of this patient (2 marks) Question 5 Answer Dr Ien Ly A 45 year-old female has long standing low back pain was discharged the preceding day by a JMO in your ED with a diagnosis of malingering. She now presents to the ED with a sudden and severe lower back pain radiating down the legs. In the department she was unable to control herself and was incontinent of urine. 1. What 6 features would suggest cauda equina syndrome? (3 marks) sciatica variable motor and sensory loss both lower limbs urinary incontinence bowel dysfunction saddle anaesthesia bilaterally absent ankle reflexes need to score 2 correct answers for each 1 mark 2. List the essential test to aid the assessment of a patient with suspected cauda equina syndrome (1 mark) MRI 3. You investigate and find that the JMO did not examine the patient, wrote no notes and was heard by the ED RN to tell the patient that there is nothing wrong with them and they should not have come to the ED, again. You are the JMO’s supervisor. Outline your approach to this situation (4 marks) Arrange to speak with the JMO privately Assess if any drugs, alcohol, mental health issues with the JMO and if concern escalate to ED Director and or medical board Educate that not appropriate was of handling this situation Document record of conversation Inform JMO that patient may complain – should contact medical defence and write contemporaneous notes Review departmental protocol for JMO supervision NB if mentions 6 of the above score 4, if 4-5 score 3, if 3-4 score 2, if 1-2 score 1 4. Outline the immediate steps in the management of this patient (2 marks) Bed rest with pressure relieving mattress bladder scan/ urinary catheter analgesia neurosurgical review discectomy/ laminectomy Question 23 A 32 year old lady who is 36 weeks pregnant presented with headache, drowsiness and her observations and results are as follows: Pulse 110 bpm BP180/110mmhg RR24/min Sats 96%air; Hb 9gm/dl WCC 8 x109/L PLT 34 x109/L LFT: AST 120 u/L, ALT 135 u/L, LDH 750 u/L 1. What is the diagnosis? (2 marks) 2. What 2 anti-hypertensive drugs would you consider to treat her blood pressure? (2 marks) 3. You have paged the PICU doctor and obstetrician to your resuscitation room, however, your patient starts to have a seizure. What are the first four things you would do? (4 marks) 4. What are the 4 signs of maternal toxicity with magnesium sulphate which would predict either respiratory or cardiac arrest? (2 marks) Question 25 A 22 year old male with known cerebral palsy presented to ED with a seizure. He complains of worsening headache and is known to have VP shunt. His observations are stable and GCS15. 1. List the 3 most likely causes of worsening headache in this man? (2 marks) 2. How do you interpret shunt function after locating and pressing the chamber? (2 marks) 3. What 2 radiological investigations will you arrange for a suspected blocked VP shunt. Explain your rational for each (2 marks) 3. The neurosurgical registrar asks you to perform a shunt tap. Outline the steps (2 marks) 4. What are the possible outcomes of the shunt tap and what is their significance? (2 marks) Question 25 Answer Dr Mana Ittimani A 22 year old male with known cerebral palsy presented to ED with a seizure. He complains of worsening headache and is known to have VP shunt. His observations are stable and GCS15. 1. List the 3 most likely causes of worsening headache in this man? (2 marks) developing hydrocephalus due to shunt blockade (shunt malfunction or infection) intracranial trauma OR infection (either answer acceptable) 2. How do you interpret shunt function after locating and pressing the chamber? (2 marks) Difficulty compressing the chamber indicates distal flow obstruction slow refill, defined as refill requiring >3 seconds after compression, generally indicates a proximal obstruction NB compression is inaccurate in identifying shunt obstruction 3. What 2 radiological investigations will you arrange for a suspected blocked VP shunt. Explain your rational for each (2 marks) shunt series of plain from skull to abdomen (for ventriculoperitoneal shunts) will identify kinking, migration, or disconnection of the shunt system. Brain CT is required to evaluate ventricular size .Comparison with previous CT scans is needed, because many patients with shunts have an abnormal baseline ventricular size.. 3. The neurosurgical registrar asks you to perform a shunt tap. Outline the steps (2 marks) Consent/ explain to patient Locate site over the valve system PPE with sterile gloves and gown Sterile field with antiseptic A 23-gauge needle or butterfly attached to a manometer is inserted into the reservoir 4. What are the possible outcomes of the shunt tap and what is their significance? (2 marks) If no fluid returns or flow ceases, a proximal obstruction is likely. The opening pressure should be measured while the reservoir outflow is occluded. An opening pressure of ≥20 cm H2O (normal 12 ± 2 ) indicates a distal obstruction, whereas low pressures indicate a proximal obstruction. 1. A 19 year old university student presents to the ED via ambulance. She is confused and has a widespread purpuric rash but no meningism. Her temperature is 38.7°C, HR 140 /min, BP 70/30 mmHg. a. What is the likely diagnosis? (1 mark) b. List 4 immediate drug management priorities with doses. (4 marks) c. What other management needs to be considered? (2 marks) d. The patient is deteriorating despite aggressive intervention. The parents arrive in the resus room and 5 minutes later the patient has a cardiorespiratory arrest. Outline 3 issues around having the parents present in the resus room. (3 marks) 1. A 19 year old university student presents to the ED via ambulance. She is confused and has a widespread purpuric rash but no meningism. Her temperature is 38.7°C, HR 140 /min, BP 70/30 mmHg. a. What is the likely diagnosis? (1 mark) Meningococcal Septicaemia b. List 4 immediate drug management priorities with doses. (4 marks) 1. Immediate antibiotic administration ceftriaxone 2g IV 2. IV fluids initial bolus 30ml/kg then further 20ml/kg titrated to response 3. Noradrenaline if poor response to fluid bolus 10mg in 100mls at 1-20mls/hr aim MAP >65 (or other reasonable dosing schedule) 4. PPE for staff particularly airway Dr c. What other management needs to be considered? (2 marks) Prepare for physiologically difficult intubation Public health notification and staff plus contact prophylaxis Treatment of coagulopathy Disposition ICU d. The patient is deteriorating despite aggressive intervention. The parents arrive in the resus room and 5 minutes later the patient has a cardiorespiratory arrest. Outline 3 issues around having the parents present in the resus room. (3 marks) Many documented benefits for family: reduced PTSD, helps grief, seeing that everything done, felt supported patient, aids family cohesion/bonding. Negatives are can disrupt the resus and need to be removed, needs a dedicated staff member to look after family 12. A 7 year old child presents to the ED with a 12 hour history of headache and photophobia, but no rash. Urea and Electrolytes as follows Na+ K+ U Cr 125 3.7 3.2 51 mmol/L mmol/L a. Give 2 possible neurological diagnoses for the symptoms described. (2 marks) b. What is the neurological cause for the Hyponatraemia? (1 mark) c. What are 2 complications of Hyponatraemia? (2 marks) d. List 5 investigations you would perform in the ED for a patient with Hyponatraemia. (5 marks) 12. A 7 year old child presents to the ED with a 12 hour history of headache and photophobia, but no rash. Urea and Electrolytes as follows Na+ K+ U Cr 125 3.7 3.2 51 mmol/L mmol/L a. Give 2 possible neurological diagnoses for the symptoms described. (2 marks) Meningitis, intracranial haemorrhage, Migraine, Encephalitis b. What is the neurological cause for the Hyponatraemia? (1 mark) Meningitis c. What are 2 complications of Hyponatraemia? (2 marks) Seizure, anorexia, headache, drowsiness, nausea and vomiting, tachycardia and about 10 million others d. List 5 investigations you would perform in the ED for a patient with Hyponatraemia. (5 marks) Urinalasis, FBC, U&Es, LFTs, BM/glucose, urine osmolality, ECG, CXr, consider CT head, LP if no signs of raised ICP 19. A 28 year old man has been out kite surfing and was thrown into the water at high speed. He is brought in on a spinal board with C-spine protection. He is intubated and ventilated and put on a propofol infusion. His observations are: Pulse 65 /min, BP 90/60 mmHg and he is warm and well perfused. The C-spine film and tomogram are shown below. a. Describe 3 abnormalities on the x-ray. (3 marks) b. Describe 2 aspects of his cardiovascular status. (2 marks). Hypotensive and bradycardic/normocardic c. What is the likely diagnosis? (2 marks) d. What 3 signs would support this? (3 marks) 19. A 28 year old man has been out kite surfing and was thrown into the water at high speed. He is brought in on a spinal board with C-spine protection. He is intubated and ventilated and put on a propofol infusion. His observations are: Pulse 65 /min, BP 90/60 mmHg and he is warm and well perfused. The C-spine film and tomogram are shown below. a. Describe 3 abnormalities on the x-ray. (3 marks) # body C4, loss of space C3-4, probably soft tissue swelling Burst fracture b. Describe 2 aspects of his cardiovascular status. (2 marks). Hypotensive and bradycardic/normocardic c. What is the likely diagnosis? (2 marks) Spinal shock d. What 3 signs would support this? (3 marks) priapism Pink, well perfused peripheries, flaccid paralysis below level C4, increased tendon jerk reflexes below that level (might be absent initially) loss of sensation, very weak respiratory effort, 20. A 42 year old man has been found outside the ED fitting. He is dishevelled and smells strongly of alcohol. His BM is 2.4 a. What is the definition of status epilepticus? (1 marks) b. Name 3 steps in managing his fitting. (2 marks) c. List 3 reasons for organising an urgent CT head on this man.(3 marks) d. Give 4 reasons why alcoholics are more prone to fit. (4 marks) 20. A 42 year old man has been found outside the ED fitting. He is dishevelled and smells strongly of alcohol. His BM is 2.4 a. What is the definition of status epilepticus? (1 marks) Status epilepticus is seizure lasting > 30mins or more than one seizure wiith failure to recover between fits. b. Name 3 steps in managing his fitting. (2 marks) Treatments: support airway and give high flow oxygen. And check BM Give 4mg IV lorazepam or 10mg iv diazemuls. Pabrinex IV replacement and then give 50mls 50% dextrose or 500mls 10% dextrose IV. May need phenytoin 18mg/kg IV or thiopentone 4-3-5mg/kg. c. List 3 reasons for organising an urgent CT head on this man.(3 marks) Reasons for CT. May have intracranial bleed requiring surgery. May have meningitis.encephalitis and need LP and look for SOL. Possibility of closed head trauma d. Give 4 reasons why alcoholics are more prone to fit. (4 marks) more likely to have head injury with complications. Alcohol withdrawal. coagulopathy making bleeds worse, impaired gluconeogenesis causing low BM 62. A two month old infant has been brought in following a brief seizure. She has had coryzal symptoms and high fevers for two days. She has no relevant past history and no allergies. On examination: HR 110 /min, BP 80/45 mmHg, Temp 39.7°C. There is no rash and no clear focus of infection but the child is ill-appearing and drowsy. a. What investigations are required? Investigation Justification A lumbar puncture is performed: CSF white cell count Neutrophils 120 (nil) Lymphocytes 25 (<5) CSF red cell count 200 CSF Protein 1.2 (< 0.4 g/L) CSF glucose 0.4 (> 2.5 mmol/L) b. Interpret these results. c. List and justify the medications you would use to treat this child. Medication Justification Dose d. A senior nurse complains to you that one of the junior doctors involved in this case has been caught stealing a box of ciprofloxacin. A formal incident report has been filed and the nurse wants you to “deal with the JMO”. The doctor says he only wanted to take some as prophylaxis against possible meningococcus. What key principles should you consider in your discussion with the JMO? 62. A two month old infant has been brought in following a brief seizure. She has had coryzal symptoms and high fevers for two days. She has no relevant past history and no allergies. On examination: HR 110 /min, BP 80/45 mmHg, Temp 39.7°C. There is no rash and no clear focus of infection but the child is ill-appearing and drowsy. a. What investigations are required? Investigation Justification WCC (FBC) At 2 months most would consider too young to assess on Other inflammatory markers – purely clinical grounds. CRP etc Could comment that WCC/CRP do not confirm/exclude SBI Electrolytes Sick child – possible abnormality of fluids in/out Urine Part of septic workup – especially as going to give antibiotics CSF Part of septic workup. While this could be a “simple febrile convulsion” with another source of sepsis LP is mandatory in this setting Blood culture Sepsis workup A lumbar puncture is performed: CSF white cell count Neutrophils 120 (nil) Lymphocytes 25 (<5) CSF red cell count 200 CSF Protein 1.2 (< 0.4 g/L) CSF glucose 0.4 (> 2.5 mmol/L) b. Interpret these results. Highly suggestive of bacterial meningitis. Likely a “traumatic tap” but ratio of RBC:WBC still indicates too many WBCs c. List and justify the medications you would use to treat this child. Medication Justification Dose Cefotaxime Could choose ceftriaxone though 50mg/kg 6th hourly under 3 months usually cefotaxime (hepatic immaturity) (ceftriaxone 100mg/kg 12th hourly) Ben Penicillin To cover listeria 60mg/kg 4th hourly Vancomycin For resistant S pneu – local practice 30 mg/kg 12th hourly varies – depends on local prevalence. Some wait for CSF gram stain or antigen studies Dexamethasone Give before or with antibiotics. 0.15 mg/kg Reduce hearing loss in Hib meningitis (JAMA 1997). Decrease poor outcomes (GOS) & death (NEJM 2002) Paracetamol For fever 15mg/kg d. A senior nurse complains to you that one of the junior doctors involved in this case has been caught stealing a box of ciprofloxacin. A formal incident report has been filed and the nurse wants you to “deal with the JMO”. The doctor says he only wanted to take some as prophylaxis against possible meningococcus. What key principles should you consider in your discussion with the JMO? Non-judgemental, non-confrontational, confidential, document discussion. “Stealing” drugs is potentially serious – disciplinary/employment ramifications Doctor needs counselling - ?apology etc Concern about infection not entirely unreasonable though prophylaxis only indictaed if meningococcus confirmed & close exposure (e.g. suctioning, intubation) 67. A 40-year-old female has been brought in following increasing confusion and agitation at home this morning. She has had no other symptoms. She is day 3 after normal vaginal delivery of a healthy baby at another hospital, but her antenatal history is unknown. Ambulance officers report a generalised tonic-clonic seizure in the ambulance which required 5mg IV midazolam to terminate, followed by ongoing drowsiness and confusion. On arrival in the ED she begins to seize. ED staff and ambulance officers activate the ‘arrest call’ button and transfer her to the Resuscitation Room. When you arrive she is being nursed on a bed and a provisional trainee is supporting her airway with jaw thrust. Her intravenous cannula has tissued. On examination: Airway: snoring / partly obstructed RR 40 /min O2 saturations 95% HR 130 /min BP 180/100 mmHg Generalised tonic-clonic seizure Afebrile a. List the causes of seizure you would consider in this patient. (4 marks) b. What is your initial management? (4 marks) c. If you suspect eclampsia, what initial drugs/ dose/route/rate would you administer? (2 marks) 67. A 40-year-old female has been brought in following increasing confusion and agitation at home this morning. She has had no other symptoms. She is day 3 after normal vaginal delivery of a healthy baby at another hospital, but her antenatal history is unknown. Ambulance officers report a generalised tonic-clonic seizure in the ambulance which required 5mg IV midazolam to terminate, followed by ongoing drowsiness and confusion. On arrival in the ED she begins to seize. ED staff and ambulance officers activate the ‘arrest call’ button and transfer her to the Resuscitation Room. When you arrive she is being nursed on a bed and a provisional trainee is supporting her airway with jaw thrust. Her intravenous cannula has tissued. On examination: Airway: snoring / partly obstructed RR 40 /min O2 saturations 95% HR 130 /min BP 180/100 mmHg Generalised tonic-clonic seizure Afebrile a. List the causes of seizure you would consider in this patient. (4 marks) Eclampsia – timing unusual because post-partum but still likely Cerebral venous sinus thrombosis Meningoencephalitis e.g. post-epidural Hypoxia e.g. due to pulmonary embolus Plus at least one not directly related to pregnancy / delivery: e.g., hypoglycaemia, toxic ingestion, structural intracranial e.g. bleed, epilepsy b. What is your initial management? (4 marks) Form a team and assign roles Address ABCs esp airway: simple adjuncts initially eg suction, NPA and lie on side o Breathing: high flow O2 and nasal CO2 monitor o Circulation: IV/IO access and send bloods / bedside BSL Stop the fit: 2nd step of classic status epilepticus regime: Midazolam IV/IO/IM 5mg Seek and treat a cause from the list above, esp eclampsia (see drugs in Q3) Get help: o Obstetrics, renal / neurology, ICU c. If you suspect eclampsia, what initial drugs/ dose/route/rate would you administer? (2 marks) Magnesium sulphate: officially 4G IV over 30 mins is RNS OG policy, but it comes in 10mmol amps. Closest is 20mmol (=5G). Safe enough to give over 20 mins provided you dilute it and watch the BP. Followed by IV infusion. Hydralazine: 5mg IV over 10 mins, can repeat. 74. A 25 year old man is brought into your regional ED after a bicycle accident. He is not moving his legs and has limited upper limb movement. He has a soft stridor. His vitals are: GCS 14 P 62 BP 80/40 Sats 95 /min mmHg % 10L O2 A CT neck is done as part of his assessment. a. Describe the major abnormalities. (3 marks) b. Outline your management of his airway and breathing. (7 marks) 74. A 25 year old man is brought into your regional ED after a bicycle accident. He is not moving his legs and has limited upper limb movement. He has a soft stridor. His vitals are: GCS 14 P 62 BP 80/40 Sats 95 /min mmHg % 10L O2 A CT neck is done as part of his assessment. a. Describe the major abnormalities. (3 marks) Bilateral facet dislocation atC6/7 with posterior displacement by one vertebral width and spinal cord impingement. Large haematoma anterior to C5-T3 causing tracheal and airway compression at subglottic and glottis level b. Outline your management of his airway and breathing. (7 marks) Needs airway soon but not NOW. Potentially difficult ++ MILI and gentle technique mandatory Careful planning preO2 as much as possible Support BP: fluids then pressors as likely neurogenic shock (must have pressor available if not given pre induction). Induction drug must be HD Ok (eg ketamine fentanyl, not big dose props) Mandatory backup surgical option considered Options depend on access in institution ; thus OT with fibreoptic/gas; definitie trache primarily with ENT; glidescope in ED with bougie etc. Consider other injuries in decision making 78. A 72 year old man comes in with change in facial appearance and mild headache. a. What are the key clinical findings from this photo? (2 marks) b. What is the likely diagnosis with justification? (2 marks) c. What other findings would you search for on physical exam? (2 marks) d. Outline your disposition and management plan (4 marks) 78. A 72 year old man comes in with change in facial appearance and mild headache. a. What are the key clinical findings from this photo? (2 marks) R facial droop, Forehead sparing on left b. What is the likely diagnosis with justification? (2 marks) Bells palsy as sparing suggests LMN lesion c. What other findings would you search for on physical exam? (2 marks) Herpetic lesions (ears, nose, eyes), other focal neuro abnormality particularly multiple other CNs; ticks in ear/folds; d. Outline your disposition and management plan (4 marks) Usually home if confirmed bells; give Prednisolone consider valaciclovir if <72hr; needs attention to eye care and advice re taping, lubrication; prognosis advice re likely full recovery but risk of partial or non recovery; GP FU with neurology if persisting or DDX not excluded SAQ 1 A 45 year old woman has presented to ED with severe headache You are concerned about possibility of a SAH List 4 risk factors for SAH Smoking HTN PCKD Known AVM or aneurysm Connective tissue disorder List 3 advantages and 3 disadvantages of CT imaging in this place Advantages Disadvantages Sensitivity 98% Radiation exposure Alternative diagnosis visible Sensitivity drops with time (93% at 24h) Quick and non invasive Contrast load if CTA done Not mobile What is the sensitivity of LP in diagnosis of SAH Negative LP and CT >99% sensitivity Most sensitive at 12h post At 24 hours WCC:RCC 1:1000 May start to see raised WCC later on due to chemical meningitis Xanthocromia still present in patients at 2 weeks 70% at 3 weeks Clinical grading system of severity SAQ 2 WFNS o I – GCS 15 no neurology o 2 GCS 13-14 with no neurology o 3 - GCS 13-14 with neurology o 4 – GCS 12-7 +/- neurology o 5 – GCS 3-6 Hunt and Hess o 1 – Mild headache, no neurology o 2 – Severe headache +/- CN deficit o 3 – Somnolent, confused +/- CN deficit o 4 – stupor, motor deficit o 5 – Coma, reflex posturing or flaccid A 65-year-old woman presents to your ED with right-sided arm and leg weakness. You are considering the diagnosis of stroke List the clinical features you would be looking for in your history and examination that would make this patient a possible candidate for thrombolysis History o Time of onset (<4.5 hours) o No contraindication to thrombolysis o Pre-morbid state Examination o Severity NIHSS score >4<22 o Absence of stroke Mimics Seizure Sugar Salt Sepsis SOL List 3 possible causes that might be evident on CT to explain this patients right sided weakness – include the expected CT findings Ischemic stroke – plain normal but detected on perfusion, Dense MCA sign Left sided hemorrhagic stroke – hyperdense areas on CT consistent with blood SOL with surrounding oedema/haemorrhage The patient receives thrombolysis for stroke, 30 minutes later you are called to see the patient due to ALOC – most likely intracranial bleed, GCS 3, HR 100, SBO 180 What are your management priorities? SAQ 3 Very poor prognosis Priority is establishing ceiling of care Influencing factors include o Patients wishes o Advanced health directive o Premorbid function If decide to manage – protect brain tissue still left as best as possible o Airway Protection o Neuroprotection o Urgent neurosurgical involvement o Reverse coagulopathy Tranexamic acid 1g Cryoprecipitate 10units targeted to fibrinogen FFP 10ml/Kg aiming INR >1.5 o If on aspirin give platelets A 16-year-old boy has been referred to ED by his local doctor with headache and fever. Febrile 38.9 and LP performed List your differential diagnosis and explain how CSF would fit with result Differential Viral meningitis Supportive CSF findings Gram stain negative WCC 105 Mainly mononuclear cells Bacterial meningitis WCC 105 Glucose lower Protein raised Fungal No gram stain seen Lowered glucose WCC 105 Partially treated bacterial infection Gram stain negative Rest of bacterial stuff Aseptic meningitis What further tests would you do to determine the causative agent? Blood – Culture, PCR CSF – culture, PCR, India ink (Cryptococcus) Urinary antigens Zielh neilson – TB List treatment priorities for this boy SAQ 4 IV antibiotics – ceftriaxone 50mg/Kg Acyclovir – 10mg/Kg Dexamethasone 4mg/Kg Treat sepsis – IVF 20ml/kg normal saline Contact tracing/treatment BSL A 19-year-old woman has been referred to the ED by her local doctor with suspected Guillain Barre Syndrome. Her presenting problem is progressive bilateral lower limb weakness. List 4 alternative diagnoses for this condition Spinal cord trauma Non traumatic spinal cord injury o Epidural abscess o Hematoma o Malignancy o Demyelination Toxin related – tick paralysis, snake bite, botulism Myopathy – Myasthenia gravis Conversion disorder List the examination features you expect to find in keeping with the diagnosis of GBS Progressive ascending symmetrical weakness without sensory deficit (although in reality get sensation changes) Loss of DTRs Maximal weakness within 2-4 weeks of onset Cranial nerve involvement is common with facial nerve involvement in 70% of cases Autonomic dysregulation in 2/3rd Miller fisher variant – cranial nerve involvement especially bulbar List 2 tests with expectant findings that would support the diagnosis of GBS Test LP Finding High CSF protein Normal glucose Normal cell count Nerve conduction study Consistent with peripheral demyelination MRI To exclude other causes Serology Antiganglioside antibodies, inciting infections – CMV, campylobacter In the ED what 2 life threatening complications may arise – For each list how you will aim to minimize their impact upon the patient Complication Detection/Mitigation Ventilatory Failure Regular PEF Early intubation and ICU referral if concerns Autonomic dysfunction of dysrhythmias Anything that provokes vagal stimulation – Intubation, IDC Cardiac monitoring Avoid sudden posture changes SAQ 5 A 26-year-old male BIBA following a collapse at a building site. Bystanders saw him collapse to the ground whilst working. He was unresponsive and jerking all limbs for a brief period. His conscious level has improved enroute to the hospital. GCS 13, BP 120/80, HR 100, T=37.8 List 5 causes that you would consider in the differential diagnosis Seizure – primary seizure disorder Cardiac – arrhythmias, WPW, HOCM Metabolic – hypoglycemia, hyponatraemia Neurological – SAH, SOL with bleed Vasovagal Toxins Drug withdrawal List 5 clinical features from the history or examination that would suggest this a seizure rather than another cause of collapse Pre-existing seizure disorder Post ictal state Aura Urinary incontinence Progression of seizure Tongue biting Improvement in GCS Absence of focal neurology What are the factors you would consider in determining his suitability for discharge? Specifics for the condition o GCS returned to 15 o Nil focal neurology o Excluded any serious causes that need treatment o Follow up organized/information if further seizure o Single seizure – full recovery o No serious complication from the seizure o Patients understands risk to self General o Normal vitals o Written and verbal discharge information given o Time of day o Family/parents with them o Understanding when to return He is kept in overnight in the ED SSU. In the morning he expresses the wish to return to work and continue to drive a motor vehicle despite your advice against it. What are 5 medicolegal concepts that this scenario raises for further consideration? Patient interest – Autonomy, confidentiality Community interest – Duty of care to community Local driving laws – Able to alert department of transport despite confidentiality as have duty to community Documentation SAQ 6 55 year old diabetic man has presented to ED after sudden onset of dizziness - established that symptoms are consistent with vertigo 4 features of examination that will be useful in differentiating central from peripheral Peripheral Central Onset Acute Gradual Severity Severe Less intense Duration Paroxysmal, intermittent, minutes to days Constant Positional Yes No Frequent Infrequent Rotary –, horizontal Vertical Fatigue of symptoms Yes No Hearing loss/tinnitus May occur Not usually No Usually Associated nausea Nystagmus CNS symptoms HINTS o Head impulse o Nystagmus o Test of skew List 5 causes of vertigo of peripheral origin BPPV Vestibular neuritis Acute labyrinthitis Meniere’s disease Ototoxicity Eight nerve lesions – acoustic neuromas Post-traumatic vertigo List the steps involved in performing a Dix-Hallpaike test Patient seated upright To test the right posterior semicircular canal the head is initially rotated 30-45 degrees to the right and the patient quickly brought to the horizontal position with the head placed 30-45degrees below the level of the bed A positive test is indicated by rotatory nystagmus towards the affected ear The test is then repeated on the left side Status Epilepticus 2 or more seizures without full recovery of consciousness between or seizures lasting >30min 1ST LINE AGENTS DRUG Midazolam or DOSE IV 5-10mg (0.2mg/kg) NOTES 15% more effective than Diaz Can be given IM/Buccal/Intranasal Diazepam or 10-20mg (0.1-0.1mg/kg) Clonazepam or 1-2mg over 2-5min Can be given PR AND Phenytoin or 15-20mg/kg (max 50mg/min) Valproate 400-800mg (10mg/kg) followed by infusion 2ND LINE AGENTS Phenytoin as above 3RD LINE AGENTS Thiopentone and 3-5mg/kg Suxamethonium 1.5mg/kg Need to follow up with one of these as Benzo’s only work for 30minutes Thrombolytic Therapy in Stroke ASK, MAST-1, MAST E were all negative trials using streptokinase. 2 other RCTs were stopped due to ICH incidence too high NINNDs (National institute of neurological disorders and stroke study) using tPA report a favourable outcome at 3 months with a RR of 1.7 in all causes of stroke o Criticisms Imbalance of stroke severity in treatment groups Groups not highly representative of typical stroke patients – able to show improvement within 3 hours when 50% of patients were treated in half that time Left out comparisons of the median NIH stroke scale despite them being recorded o tPA when administered within 3 hours of onset o Inclusion Within 3 hours of known stroke onset Must have a CT scan excluding ICH o 13% improvement in neurological outcome o 6.4% increase in ICH – half of which were fatal o No overall excess mortality o Increased haemorrhage risk >80 Increased severity of stroke Early changes on CT ECASS 1, 2, 3 – European cooperative acute stroke study – there were 3 of these the latest being published in 2008 o No statistical significance Cochrane review 2009 – can use within 4.5 hours but doctor dependent Preparation and treatment Contraindications – iBUMP 4S o I – Improving or minor symptoms o B – BP >185 o U – unknown onset of time o M – Major neuro deficits o P – PLT <100 o S – Scant CT bad o S – seizure o S – sugars <3 or >20 o S – other standard thrombolysis contraindications (recent surgery, ICH, etc) Thrombolysis in stroke – PROs vs. CONs PRO CON Registry data shows tPA use outside of a trial is same as in the trial (i.e. safe) The 2 major supporting trials were funded by a tPA manufacturer and were relatively small Reported benefit of tPA at 3 months and sustained at 1 year Only 2 trials that showed positive effect had imbalance of stroke severity efficacy likely lower Experts from many specialist societies support its use Virtually no data for those >80 NNT 8 Higher incidence of cardio embolic stroke in trial vs. placebo group Small number of eligible patients means ED is disrupted only occasionally ED patients still disrupted and resources used (CR scanner, resus bay) for a potentially small benefit (when compared with stroke teams) Personal burden of a stroke is high (20% disabled) – change to decrease this could be life changing for the patient and their family Only 5% of those presented to ED with stroke are eligible Stroke mimics Consent difficult to obtain Cost efficacy – may be better to spend money on stroke teams Thrombolysis of stroke vs. AMI AMI Stroke Simple work up Complex work up Pathophysiology similar in all cases Different pathological processes (embolic, lacunar, haemorrhage, avm etc.) 6 hour time frame for treatment 3-4.5hr time frame Greater benefit from large infarcts (1% risk of harm) Greatest benefit for medium sized infarcts Clear mortality benefit Very high risk (3%) and early mortality risk Small functional benefit Possible functional benefit Repeatedly proven in multiple trials >100 000 patients in AMI Small number of patients studied