Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
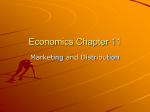
Journal of the American College of Cardiology © 2002 by the American College of Cardiology Foundation Published by Elsevier Science Inc. Vol. 40, No. 7, 2002 ISSN 0735-1097/02/$22.00 PII S0735-1097(02)02140-X Cost/Utility Ratio in Chronic Heart Failure: Comparison Between Heart Failure Management Program Delivered by Day-Hospital and Usual Care Soccorso Capomolla, MD, Oreste Febo, MD, Monica Ceresa, MD, Angelo Caporotondi, MD, Giampaolo Guazzotti, MD, Maria Teresa La Rovere, MD, Marina Ferrari, NS, Francesca Lenta, NS, Sonia Baldin, NS, Chiara Vaccarini, MD, Marco Gnemmi, MD, GianDomenico Pinna, MS, Roberto Maestri, MS, Paola Abelli, MD, Sandro Verdirosi, MD, Franco Cobelli, MD Montescano, Italy This study compared the effectiveness and cost/utility ratio between a heart failure (HF) management program delivered by day-hospital (DH) and usual care in chronic heart failure (CHF) outpatients. BACKGROUND Previous studies showed that about 50% of readmissions for CHF can be prevented by a multidisciplinary approach However, the performance, effectiveness, and cost/utility ratio of a process of HF outpatient management related to evidence-based medicine have not been considered. METHODS A total of 234 prospective patients discharged by a HF Unit were randomized to two management strategies: 122 patients to usual community care and 112 patients to a HF management program delivered by the DH. Management (rate of readmissions, therapeutic interventions), functional parameters (New York Heart Association [NYHA] functional class, left ventricular diameters, and ejection fraction, deceleration time of early diastolic mitral flow, peak oxygen uptake, and mitral regurgitation) and hard outcomes (cardiac death and urgent cardiac transplantation) were evaluated. The cost/utility ratios of the two strategies were compared. RESULTS After 12 ⫾ 3 months of follow-up, the individual rate access in DH was 5.5 ⫾ 3.8 days. The DH subjects were readmitted to the hospital less frequently than were the usual-care group patients (13 vs. 78, p ⬍ 0.00001). Patients allocated to usual-care management showed heterogeneous changes in NYHA functional class (13% improved and 16% worsened p ⫽ NS); In contrast, the DH group showed significant changes in NYHA functional class (23% improved and 11% worsened, p ⬍ 0.009). Hard cardiac events in the one-year follow-up occurred in 25/234 (10.6%) patients; cardiac death occurred in 21/122 (17.2%) of the community group and in 3/112 (2.7%) in the DH group (p ⬍ 0.0007). One DH patient underwent urgent transplantation. Comparison of the two managerial models by Cox regression analysis showed that DH management significantly protected against the appearance of hard events (relative risk [RR] 0.17; confidence interval [CI] 0.06 to 0.66). The cost/utility ratio of the two management strategies was similar (usual care $2,409 vs. DH $2,244). The incremental analysis revealed a cost savings of $1,068 for each quality-adjusted life year gained. The cost/utility ratio for the integration of DH management of CHF was $19,462 (CI $13,904 to $34,048). CONCLUSIONS A heart failure outpatient management program delivered by a DH can reduce mortality and morbidity of CHF patients. This management strategy is cost-effective and has an equitable value from a societal point of view. (J Am Coll Cardiol 2002;40:1259 – 66) © 2002 by the American College of Cardiology Foundation OBJECTIVES Heart failure (HF) is a growing public health problem. Both the incidence and the prevalence of chronic heart failure (CHF) are clearly increasing in industrialized countries, and HF continues to be a significant cause of hospital admissions (1,2). In the U.S. it has been evaluated that about 20% of patients with CHF require hospital management (3). In Italy, the Survey on Heart Failure in Italian Hospital Cardiology Units (SEOSI) study showed that about 65,000 patients with CHF are admitted to cardiology departments in Italy each year (4). Including patients cared for in other From Fondazione “Salvatore Maugeri,” IRCCS, Dipartimento di Cardiologia, Istituto Scientifico di Montescano, Montescano, Pavia, Italy. Manuscript received December 28, 2001; revised manuscript received May 13, 2002, accepted June 27, 2002. hospital wards, a realistic projection might be that about 230,000 patients with CHF are hospitalized annually in Italy (5). In the U.S., CHF costs about $38 billion, of which approximately two-thirds of this amount are spent on readmissions to hospital (6). Pharmacoeconomic studies support the need to rationalize expenditures by containing these repeated admissions (7). Recent studies demonstrate how comprehensive management strategies can improve outcomes and quality of life with fewer hospital admissions and lower consumption of resources (8 –12). However, different organizational patterns, types of patients, and care settings make these other management algorithms poorly applicable, thus influencing outcomes (13). In effect, although researchers identified the elements relevant to the Capomolla et al. Cost/Utility Ratio in CHF 1260 Abbreviations and Acronyms ACE ⫽ angiotensin-converting enzyme CHF ⫽ chronic heart failure CI ⫽ confidence interval DH ⫽ day-hospital DRG ⫽ diagnosis-related group EBM ⫽ evidence-based medicine HF ⫽ heart failure HFU ⫽ Heart Failure Unit IV ⫽ intravenous LVEF ⫽ left ventricular ejection fraction NYHA ⫽ New York Heart Association functional class QALY ⫽ quality-adjusted life years RR ⫽ relative risk VO2 ⫽ oxygen uptake process of care decisions, the different management patterns and complexities of illness render both the process and the link between management and outcome poorly defined. In the early 1990s, a Heart Failure Unit (HFU) was opened in the Medical Center of Montescano. In 1998, a day-hospital (DH), dedicated and open to the community, was established within the HFU, increasing the HF management options available. In this study we describe our comprehensive HF outpatient management program and evaluate cost-effectiveness of this different approach relative to the usual program of care after discharge from an HFU. METHODS Study Design This study was conducted in the setting of a “proof-ofconcept” phase of the disease management program (14). Patients referred to our HFU had a prognostic evaluation, their therapy was optimized, and they were then randomized to one of two management strategies: 1) usual care: the patient returned to the community and was followed up by a primary care physician with the support of a cardiologist; 2) DH care within the HFU, which implemented an individualized HF management program. The primary outcomes employed to evaluate any difference between the two strategies were readmissions because of hemodynamic instability and death from cardiac causes. Secondary outcome measurements considered were tailored therapy management, quality of life (using the time trade-off method), and New York Heart Association (NYHA) functional class (15). The study design included an evaluation of the cost/utility ratio of the two strategies. Patients Patients with CHF referred to the HFU of Montescano Medical Center and the Heart Transplantation Program of the Cardiac Surgery Division of Policlinico S. Matteo, Pavia, between January 1999 and January 2000 were considered. The diagnosis of CHF was supported by clinical history, physical signs and symptoms, and by echocardio- JACC Vol. 40, No. 7, 2002 October 2, 2002:1259–66 graphic findings (left ventricular ejection fraction [LVEF] ⬍40%). At referral, patients underwent an initial cardiac prognostic stratification that included a clinical examination, functional status evaluation (NYHA functional class), cardiopulmonary exercise test (peak oxygen uptake [VO2]), echo-Doppler examination (LVEF, mitral regurgitation, left end-diastolic and end-systolic diameters, and deceleration time of early diastolic filling wave), and right hemodynamic measurements (pulmonary wedge pressure, cardiac index). After this first step the patients were prescribed individual tailored therapy following heart practice guidelines and evidence-based medicine (EBM) (16 –18). At discharge the patients were randomized either to receive usual care or to enter the HF management program performed in the DH of the HFU. Management Strategies Usual care. Patients were referred to their primary care physician and cardiologist. During follow-up the process of care was driven by the patient’s needs into a heterogeneous range of emergency room management, hospital admission, and outpatient access. After 12 months all patients were reevaluated at the HFU by repeating the baseline tests and investigations. Day-hospital. STAFF. The staff of the HF management program consists of one cardiologist, four trained nurses with consolidated experience, and two physiotherapists. There is also part-time participation of a dietician, a psychologist, and a social assistant. The objectives of the multidisciplinary staff are prevention and functional recovery of consequences of acute hemodynamic instabilization. The team members also have the task of creating, analyzing, and correcting the organization that supports the process of treatment identified in an individual care plan (19). There are three different organizational levels (physician, nurse, physiotherapist), each of which coordinates with the others to achieve the treatment objectives. The team management used current HF guidelines and EBM criteria. PROCESS OF CARE. The process of care is discussed in collaboration among the different health care professionals. A plan of care is structured for each patient (20) and defines: 1) appropriateness of the access; 2) type of access (new patient, patient activated in a program of cardiac transplantation, control or open access); 3) objective of the process (prognostic stratification, therapeutic optimization, analysis of the primary pathology, check of clinical stability, review of cardiovascular risk factors, review of factors of risk for hemodynamic instabilization); 4) use of tools (cardiac echoDoppler, cardiopulmonary exercise test, Holter monitoring, right heart catheterization, psychological support, nutritional intervention, counseling); 5) markers of outcomes, and finally 6) follow-up counseling. TAILORED INTERVENTIONS. According to the characteristics of the patient and the phase of the illness, particular areas of intervention are: Capomolla et al. Cost/Utility Ratio in CHF JACC Vol. 40, No. 7, 2002 October 2, 2002:1259–66 1. cardiovascular risk stratification. In daily practice we grade the patient’s severity of disease by NYHA functional class, left ventricular end-systolic diameter, deceleration time of early diastolic filling, natremia, and peak VO2. Based on these criteria, we make a risk-ratio score to manage the following strategy that incorporates the therapeutic interventions and timing of follow-ups and possible heart transplantation; 2. tailored therapy according to national and international guidelines, and integration of physical training and counseling on daily life activities; 3. checking clinical stability according to EBM criteria; 4. correction of the risk factors for hemodynamic instabilization; 5. health care education: during planned use of the DH, nurses coordinate open discussion, focusing on knowledge about CHF, pharmacologic therapies, selfmanagement (daily weight monitoring, fluid restriction, nutrition); moreover, physiotherapists educate patients in self-managed physical training and tailor daily physical activity in relationship to exercise capacity as defined by cardiopulmonary exercise testing; 6. counseling: this is a continuous process between different staff members and the patient, taking place at different times. The patient is made aware of his or her own situation in such a way as to promote self-management with realistic behavioral changes. In this framework counseling becomes a tool for processing and restructuring the different but interrelated manifestations of the illness. Each morning the nursing staff gives the physician a report on the status, care plan, and decision making concerning the patients. The nursing team uses the telephone extensively to provide counseling and continuity with community care. PATIENT FOLLOW-UP. Access to the DH is modulated according to the demands of the care process. If organ function deteriorates during follow-up, or if signs/ symptoms of HF develop, the patient re-enters the DH through an open-access program allowing extemporaneous performance of a new care process (intravenous [IV] therapy, laboratory examinations, instrumental controls, therapeutic changes). If the decompensation requires full-time observation, the patient is transferred to the HFU. OUTCOME MEASUREMENTS. Three types of outcomes were identified: readmission in hospital and pharmacologic tailored therapy were evaluated as management outcomes; NYHA functional class, left ventricular diameters and ejection fraction, deceleration time of early diastolic filling wave, mitral regurgitation, peak VO2, and quality of life, appraised by the time–trade-off method, were considered as functional outcomes. Finally, death from a cardiac cause was analyzed as a hard outcome. These outcomes were evaluated after a mean follow-up of 12 months. 1261 Economic Analyses Costs. The cost/utility analysis was performed in a societal perspective (21). The initial and final admissions were not included in the costs of managing the two groups. Cost of readmissions and the management costs of the DH during the follow-up were calculated using the Medicare diagnosisrelated group (DRG) reimbursement. We assessed the costs of daily medical therapy by using the average dose of therapy at exit from the two management processes to calculate the number of tablets taken during the follow-up and multiplying this number by the cost per tablet reported in the annual formulary (22). These costs were actualized by assuming an annual rate of increase of 5% (23) and are expressed in U.S. dollars. Life expectancy. For the evaluation of life expectancy, the two management strategies were considered outcome predictors, adjusting for age, gender, etiology, NYHA functional class, LVEF, peak VO2, baseline heart rate, and mean arterial pressure. The association between predictor variables and outcome was assessed by fitting follow-up data with a Cox proportional hazards regression model. All patients who died from noncardiac causes and those who underwent elective cardiac transplantation were considered as censored observations. The end point of the study was cardiac mortality or urgent heart transplantation. Event-free distribution functions were estimated by the Kaplan-Meier method. Life expectancy was calculated as the area under each curve. The increase in life expectancy was evaluated as the difference between the areas under the two curves (24). Sensitivity analysis. The sensitivity analyses were performed by recalculation of the cost/utility ratio using an analysis of the extremes; we varied survival (confidence limits) and costs in both prospectives (higher and lower); utility was also recalculated to reflect the current state of health in the new scenario. Statistical Analysis Between-group comparisons of baseline clinical and functional parameters were performed by one-way analysis of variance for continuous variables and by the chi-square test for categorical variables. For the purpose of the prognostic evaluation, the two management strategies were considered as predictors of outcome, adjusting for age, gender, etiology, NYHA functional class, LVEF, peak VO2, baseline heart rate, and the mean arterial pressure. The combined end point was cardiac mortality and urgent heart transplantation. Event-free distribution functions were estimated by using the KaplanMeier method. Associations between predictor variables and outcome were assessed by fitting follow-up data with a Cox proportional hazards regression model. All patients who died from noncardiac causes and those who underwent elective cardiac transplantation were considered as censored observations. Prognostic information was expressed as relative risk (RR) with 95% confidence interval (CI). Descrip- 1262 Capomolla et al. Cost/Utility Ratio in CHF JACC Vol. 40, No. 7, 2002 October 2, 2002:1259–66 Table 1. Baseline Clinical, Doppler Echocardiographic, and Hemodynamic Characteristics in All Patients and in the Patients Grouped According to Management Strategies All Patients Usual Care No. of patients 234 Age (yrs) 56 ⫾ 10 Gender (M/F) 196/38 Etiology (ischemic/idiopathic) 95/139 NYHA functional class 153/81 I–II/III–IV Heart rate (beats/min) 82 ⫾ 13 Systolic pressure (mm Hg) 118 ⫾ 18 Peak VO2 (ml/min/kg) 17 ⫾ 4 LVEDD (mm) 70 ⫾ 10 LVESD (mm) 58 ⫾ 11 LVEF (%) 29 ⫾ 7 Cardiac rhythm (SR/AF) 196/38 Deceleration time E (ms) 167 ⫾ 48 Mitral regurgitation moderate/ 108 (40) severe (ⱖ2⫹), n (%) Therapy High-ceiling diuretics, n (%) 194 (83) K⫹ saver, n (%) 51 (22) Digitalis, n (%) 87 (37) ACE inhibitors, n (%) 227 (97) Beta-blockers, n (%) 93 (40) Nitrates, n (%) 108 (46) 122 56 ⫾ 9 102/20 50/72 80/42 Table 2. Goals and Tools of Care Process of Patients Exposed to Heart Failure Management Program Dayp Hospital Value 112 56 ⫾ 8 94/18 45/67 73/39 NS NS NS NS 80 ⫾ 14 81 ⫾ 16 120 ⫾ 18 114 ⫾ 16 17 ⫾ 4 17 ⫾ 4 70 ⫾ 9 68 ⫾ 10 59 ⫾ 9 57 ⫾ 9 31 ⫾ 8 29 ⫾ 10 99/23 97/15 163 ⫾ 50 155 ⫾ 55 60 (49) 48 (44) NS NS NS NS NS NS NS NS NS 99 (81) 29 (24) 47 (39) 117 (96) 48 (39) 60 (49) NS NS NS NS NS NS 95 (85) 22 (20) 40 (36) 110 (98) 45 (40) 48 (43) Continuous variables are described as mean ⫾ SD. ACE ⫽ angiotensin-converting enzyme; AF ⫽ atrial fibrillation; LVEDD ⫽ left ventricular end-diastolic diameter; LVESD ⫽ left ventricular end-systolic diameter; LVEF ⫽ left ventricular ejection fraction; NYHA ⫽ New York Heart Association class; SR ⫽ sinus rhythm; VO2 ⫽ oxygen uptake. tive statistics are presented as mean ⫾ SD. A probability value of ⬍0.05 was considered as statistically significant. Statistical analyses were performed with the SAS/STAT statistical package, release 6.12 (SAS Institute, Cary, North Carolina). RESULTS Between July 1999 and December 2000, a total of 234 patients were admitted to our HFU with a diagnosis of CHF; 122 patients were randomized to community care and 112 patients to DH-based management. No significant clinical or instrumental differences were observed between the patients in the two groups (Table 1). Their mean LVEF was 29%. The goals and tools of the HF management program are reported in Table 2. Management Outcomes During the management program, 53/112 (47%) patients underwent cardiac risk reevaluation; in 50/112 patients (45%) therapeutic variations were made. Overall, 85/112 (76%) patients participated in health education sessions and had physical training programmed. After 12 ⫾ 3 months of follow-up, 91 hospital admissions had been required for 56 patients; 78 (86%) of the admissions were for communitytreated patients, 13 (14%) for patients managed by the DH (p ⬍ 0.00001). There were 49 open-access interventions in 27 patients. Table 3 summarizes the medical regimen at Goals Check clinical stability (EBM), n (%) Cardiovascular risk stratification, n (%) Tailored therapy, n (%) Management of risk of heart failure, n (%) Health education, n (%) Counseling, n (%) Physical training, n (%) Open access, n (%) Multidisciplinary intervention, n (%) Tools Access, n Open access, n ECG, n (%) Laboratory examination, n (%) Echo-Doppler, n (%) Cardiopulmonary exercise test, n (%) Right hemodynamics, n (%) Holter monitoring, n (%) Psychological assessment, n (%) Nutritional counseling, n (%) 112 (100) 53 (47) 50 (45) 12 (11) 85 (76) 112 (100) 85 (76) 27 (24) 21 (19) 612 49 112 (100) 112 (100) 76 (68) 58 (52) 32 (28) 44 (39) 19 (17) 21 (19) ECG ⫽ electrocardiogram; EBM ⫽ evidence-based medicine. baseline and after the different management strategies. After one year, the dosages of both long- and short-acting angiotensin-converting enzyme (ACE) inhibitors, nitrates, and beta-blockers were significantly higher in the DH group than in the community group, whereas the dosages for diuretics and digitalis were lower. After one year, the frequency of use of the various drugs remained substantially unchanged, while the percentage of patients taking beta-blockers increased significantly in the DH group (40% vs. 71%, p ⬍ 0.0001) but not in the community (39% vs. 40%, p ⫽ NS). Functional Outcomes The effects of the two management strategies on functional outcomes are reported in Table 3. Patients allocated to community management showed heterogeneous changes in NYHA functional class (13% improved and 16% worsened, p ⫽ NS). In the DH group, NYHA functional class changed significantly (23% improved and 11% worsened, p ⬍ 0.009). Hard Outcomes Hard cardiac events in the one year follow-up occurred in 25/234 (10.6%) patients; cardiac death occurred in 21/122 (17.2%) of the community group and in 3/112 (2.7%) in the DH group (p ⬍ 0.0007). One DH patient underwent urgent transplantation. Comparison of the two managerial models using Cox regression analysis showed that DH management significantly protected against the appearance of hard events (RR, 0.17; CI 0.06 to 0.66). Pharmacoeconomic Analyses Pharmacologic costs. At discharge from the initial hospitalization, there was no difference between the two patient groups in terms of dosage and rate of use of drugs. At one Capomolla et al. Cost/Utility Ratio in CHF JACC Vol. 40, No. 7, 2002 October 2, 2002:1259–66 1263 Table 3. Outcomes in Patients Grouped According to Management Strategies Usual Care Management outcomes 1. Therapy ACE inhibitors long-acting (mg/day) ACE inhibitors short-term (mg/day) Beta-blockers (mg/day) High-ceiling diuretics (mg/day) K⫹ saver (mg/day) Digitalis (mg/day) Nitrates (mg/day) 2. Patients rehospitalized (n (%)) 3. No. of rehospitalizations (%) 4. Individual access Functional outcomes Systolic pressure (mm Hg) Peak VO2 (ml/min/kg) LVEDD (mm) LVESD (mm) LVEF (%) Deceleration time E (ms) Mitral regurgitation (ⱖ2⫹) NYHA (I–II/III–IV) Hard outcomes Cardiac death Urgent transplantation Day-Hospital Baseline 1 yr Baseline 1 yr 15 ⫾ 9 100 ⫾ 40 13 ⫾ 12 74 ⫾ 50 40 ⫾ 31 0.140 ⫾ 0.05 68 ⫾ 40 — 14 ⫾ 7 101 ⫾ 31 10 ⫾ 19 70 ⫾ 57 35 ⫾ 33 0.130 ⫾ 0.07 60 ⫾ 34 — — 12 ⫾ 10 103 ⫾ 39 14 ⫾ 29 85 ⫾ 107 40 ⫾ 29 0.230 ⫾ 0.08 40 ⫾ 29 37 (35) 78 (86) — — 20 ⫾ 8†* 139 ⫾ 26†* 34 ⫾ 23†* 61 ⫾ 44† 78 ⫾ 37†* 0.109 ⫾ 0.6† 84 ⫾ 46†* 9 (8)† 13 (14)† 5.5 ⫾ 3.8 120 ⫾ 18 17 ⫾ 4 70 ⫾ 9 59 ⫾ 11 31 ⫾ 7 163 ⫾ 50 2.4 ⫾ 0.4 80/42 113 ⫾ 18 16.4 ⫾ 4 71 ⫾ 10 59 ⫾ 10 30 ⫾ 9 163 ⫾ 52 2.5 ⫾ 0.9 73/49 114 ⫾ 16 17 ⫾ 4 68 ⫾ 10 61 ⫾ 10 29 ⫾ 10 155 ⫾ 55 2.7 ⫾ 0.5 73/39 117 ⫾ 20 17.8 ⫾ 5 68 ⫾ 10 54 ⫾ 12†* 34 ⫾ 7† 172 ⫾ 49 2.1 ⫾ 0.9* 91/22†* — — 21 (17.2) — — — 3 (2.7) 1 (0.9) Continuous variables are described as mean ⫾ SD. *p ⬍ 0.05 versus baseline DH. †p ⬍ 0.05 versus usual care. ACE ⫽ angiotensin-converting enzyme inhibitor; E ⫽ early diastolic filling wave of mitral flow; LVEDD ⫽ left ventricular end-diastolic diameter; LVESD ⫽ left ventricular end-systolic diameter; LVEF ⫽ left ventricular ejection fraction; NYHA ⫽ New York Heart Association functional class. year, the annual cost per patient to maintain care was greater in the DH group than in the community group ($741 vs. $490 p ⬍ 0.000001) (Table 4). Care management costs. Care management costs are the largest component of direct costs of treating CHF patients. The averaged annual cost of readmissions of community patients was $178,553. In contrast, the averaged DH care management cost was $167,785, of which $138,026 was for managed care and $29,759 for readmissions. A cost comparison of the two strategies identified that the DH model is cost-effective, with a cost-saving of $10,768. Life expectancy. Actuarial survival at one year was 96% in the DH patients and 78% in the community patients (log rank p ⬍ 0.0002) (Fig. 1). The incremental life expectancy was 0.083 years per patient. The cumulative incremental life expectancy in the DH group was 9.8 years. Time trade-off. At one year, the weighted mean utility measured by the time trade off method was greater in the DH than in the community group (0.72 ⫾ 0.17 vs. 0.63 ⫾ 0.22, p ⬍ 0.008). This result identified that DH patients were willing to trade 10 years of their present health for 7.2 years of excellent health, whereas patients in the community group were willing to trade 6.3 years. Quality-adjusted life years (QALY). Day-hospital management produced a higher QALY than that achieved in the community group (79.4 vs. 70.5, p ⬍ 0.01). Cost/utility analysis. The DH model showed a better cost/utility ratio than that of community management ($2,244 vs. $2,409). Furthermore, the incremental analysis revealed a cost-saving of $1,068 for each QALY gained. Considering an increase of 0.080 QALY per patient, an annual cost of $1,483 per patient and a 5% annual increase Table 4. Economic Profile of Patients Grouped According to Management Strategies Costs Usual Care Day-Hospital p Value Annual pharmacologic costs ($) Health management costs ($) Rehospitalization costs ($) Strategy costs ($) Cost/utility ($) Incremental cost/utility ($) (95% CI) 490 ⫾ 164 — 1,332 ⫾ 1,992 178,553 2,409 741 ⫾ 206 1,243 ⫾ 868 268 ⫾ 801 167,785 2,244 19,462 (13,904–34,048) 0.000001 — 0.000001 — — CI ⫽ confidence interval. 1264 Capomolla et al. Cost/Utility Ratio in CHF JACC Vol. 40, No. 7, 2002 October 2, 2002:1259–66 Figure 1. Probability of survival among patients managed with different strategies. A survival function was used to estimate life expectancy and the upper and lower limits in the first year for day-hospital (squares) and usual care (circles) patients. of costs ($1,557), the cost/utility ratio for the integration of DH management of CHF was $19,462 (Table 4). Sensitivity Analysis As calculated from the one-year survival curves, the 95% CIs of the 0.083-year year difference in life expectancy between the two groups were 0.041 and 0.125 years. The 95% CIs for overall costs were $1,396 and $1,738. These ranges would determine a cost/utility ratio from $13,904 to $34,048 per QALY product. DISCUSSION We compared the cost/utility ratio of usual care of CHF patients returned to the community with that of processes and outcomes of care provided by a HF management program based in a DH. Most of the patients were in NYHA functional classes II and III, best suited to primary therapeutic optimization in an HFU. This study showed that outpatient CHF management may have a better cost/ utility ratio than usual care. Our results indicate that the implementation of a structured program in a DH, inte- grated to usual care, costs $19,462 per additional QALY saved. There are essentially two points of strength of our study: 1) the formalization of the process of care and 2) the use of an EBM methodology. To define the care process, the clinicians developed the “health care intervention,” identifying the following phases: appropriateness of access to the program; the typology of the patient population; definition of the goals; necessary tools for the organization of the process; modality of the therapeutic intervention; identification and measurement of markers of outcome; evaluation of cardiovascular risk, and definition of follow-up. The EBM methodology offers valid and strong support to the decision of the process of care. In particular, EBM provided the informational and clinical elements to identify the best use of the single procedures activated in the different health care plans. Furthermore, EBM allowed us to identify the best algorithm to define individual cardiovascular risk, therapeutic treatment, and consequent follow-up. This procedure allows 1) reduction of the use of ineffective and inefficient JACC Vol. 40, No. 7, 2002 October 2, 2002:1259–66 procedures for the type of clinical case being managed; 2) avoidance of repetition of procedures caused by occasional evaluations of the clinical syndrome; and 3) simulation analysis of consequences of behavior that would subtract resources. Such simulations have allowed us to overcome possible reticence of the health staff in modifying their empirical health care practices. In this perspective the management of CHF patients changes profoundly: health care is not management of an acute event and/or clinical symptoms—a characteristic of the usual care with interventions in emergency room, and often, of the primary care physicians, cardiologists, and/or surgeons— but a continuous modulation of cardiovascular risk with interventions to prevent hemodynamic imbalance and to optimize therapy to improve quality of life and prognostic outcome. This link among process of the care, control of management, and application of EBM has allowed two primary objectives to be reached: 1) better performance effectiveness and 2) reduced absorption of resources and their better allocation. Performance effectiveness. A positive effect of the management program of CHF outpatients might be continuous optimization of therapy such as more titration of long- and short-acting ACE inhibitors. Although 97% of the patients were taking ACE inhibitors, in the DH-managed patients the mean dose of the ACE inhibitors was about 25% higher than usual care patients. Similar considerations can be made about beta-blocker treatment: at the end of the management, 71% of the DH subjects were receiving beta-blockers versus 40% of community-treated patients. Likewise, the average dose of beta-blockers was 58% higher in the DH subjects at the end of management, and essentially unchanged in the patients receiving usual care. Moreover, in about 45% of the patients cardiovascular risk reevaluation led to therapeutic variations. Although we have not yet analyzed the data on compliance and effectiveness of the health education sessions and controlled physical training, 76% of patients were offered a way of self-management of their illness. Open access was another important component of the program management. This modality of access is reserved for patients who exhibited markers and symptoms of hemodynamic imbalance during follow-up, despite therapeutic modifications performed at home. Open access to the DH allows extemporaneous execution of new care processes (IV therapy, laboratory examinations, instrumental controls, and therapeutic adjustments) by the HF care team. This implies that hospital admission—the largest part of usual-care management costs—is managed and integrated in a program of continuous definition of cardiovascular risk by echo-Doppler hemodynamic monitoring, cardiopulmonary exercise testing, measurement of biohumoral parameters, and therapeutic effectiveness evaluated by the same care team. Conversely, in usual care, hospital admission is often a Capomolla et al. Cost/Utility Ratio in CHF 1265 reactive solution to failure of a care process managed by different providers and at different times during the initial course of hemodynamic imbalance. In our experience the open-access service reduced potential hospital admissions by 79%. These combined interventions on therapeutic strategy and managerial organization justify the impact of this new care process on the outcomes in comparison to usual care. Rehospitalization was reduced by 72%. The impact of our managed program in DH on rehospitalization due to CHF was similar to that in other studies. In a 90-day follow-up of elderly patients, Rich et al. (9) showed a 56% reduction of readmission for HF. In the multifit approach, total hospitalization rates for HF declined by 74% over 12 months (12). Hanumanthu et al. (10) showed that a HF program can reduce hospitalizations for decompensated HF by 63%. Fonarow et al. (8) examined the impact of a HF program on reducing hospitalization. They showed that rehospitalizations fell from 92% in the previous six months to 26% during the study period. A recent study by Hershberger et al. (25) in an outpatient setting demonstrated that a heart failure program can reduce the risk of rehospitalization by 52%. However, some studies show that intensive management by primary-care physicians increases hospital readmission and cost management (26). Using the HFU as a benchmark, we have transferred the experience gained in the HFU into the external setting of the DH with its lower organizational costs while retaining the know-how. This has allowed the creation of a qualified provider able to strengthen and increase the effects initiated by a HF program delivered by the HFU (27,28). This HF program has already had an important impact on mortality, which has been low in patients referred to the HFU, but the effect has been enhanced in the subgroup followed up in the DH program, in whom the annual mortality rate has been reduced by 79% in comparison to that in the group referred to the HFU and subsequently followed up with usual care. The explanation of this result can, to a large extent, be attributed to the better optimized therapy. This study is the first to report effective titration of beta-blockers in 71% of the population. The BRING-UP study (29) underlined how driven titration of therapy could increase the number of beneficiaries of the treatment. Resource allocation. Heart failure is the pathology making most demands on health care and absorbing the greatest amount of economic resources. In consideration of this socioeconomic burden, the application of new managerial models should satisfy two important conditions: 1) improve the quality of the performance and 2) not increase the costs. Our model satisfies these two conditions. The effectiveness of the performance is clearly improved. The variation of resources from usual care— used for the management,of discontinuous and diversified treatments of an acute event—to the HF management program in a DH has a better cost/utility ratio with a cost-saving per QALY incremental product of $1,068. When the model is considered as integration to the usual care, the incremental analysis 1266 Capomolla et al. Cost/Utility Ratio in CHF identifies it as favorable. This service has an equitable value from a societal point of view. In fact, the cost patient/year places it between that of pacemaker implantation ($1,516), annual management of chronic pain ($2,996), and geriatric orthopedic rehabilitation ($5,555). If we compare the incremental cost/utility ratio, it is cost-effective and placed between that of ACE-inhibitor treatment in CHF ($7,777), an intravascular ultrasound-guided procedure ($6,439), a two-vessel coronary artery bypass graft surgery ($17,500), and home hemodialysis ($23,794) (30). We have treated the two management strategies as complementary models. Nevertheless, in a new definition of the scenario, the DH could be considered as a provider in the community, supplying the usual care and reducing the total resources absorbed by this pathology. Study limitations. Various limitations of our study must be acknowledged. Elderly patients and those affected by diastolic HF are poorly represented in our study population. The assessment of the costs could be underestimated because we did not evaluate costs for minor health care services nor indirect costs. Direct and indirect nonhealth care costs were not evaluated. Nevertheless, these factors should be equally distributed between the two study groups and thus should not invalidate the final compared results. The analysis of QALY are referred to the first year of follow-up. But the titration of better therapy could improve survival curves beyond one year, increasing their divergence and the final result. The relationship between the different components of the care process, their absorption of the resources, and relative contributions to the outcomes have not been evaluated. In summary, this randomized prospective study showed that, compared to usual care, a HF management program delivered by a DH improves the cost/utility ratio of managing CHF. Reprint requests and correspondence: Dr. Soccorso Capomolla, Department of Cardiology, Montescano Medical Center, Via per Montescano, 27040 Montescano, Pavia, Italy. E-mail: [email protected]. REFERENCES 1. Massie BM, Shah N. The heart failure epidemic: magnitude of the problem and potential mitigating approaches. Curr Opin Cardiol 1996;11:221–6. 2. Sharpe N, Doughty R. Epidemiology of heart failure and ventricular dysfunction. Lancet 1998;352 Suppl I:3–7. 3. Mark D. Economics of treating heart failure. Am J Cardiol 1997;80: 33H–8H. 4. SEOSI Investigators. Survey on heart failure in Italian hospital cardiology units. Results of the SEOSI study. Eur Heart J 1997;18: 1457–64. 5. Bellotti P, Badano LP, Acquarone N, et al. Specialty-related differences in the epidemiology, clinical profile, management and outcome of patients hospitalized for heart failure: the OSCUR study. Outcome dello Scompenso Cardiaco in relazione all’Utilizzo delle Risorse. Eur Heart J 2001;22:596 –604. 6. Steinwachs DM, Collins-Nakai RL, Cohn L, Garson A, Wolk MJ. The future of cardiology: utilization and costs of care. J Am Coll Cardiol 2000;35 Suppl B:91B–8B. JACC Vol. 40, No. 7, 2002 October 2, 2002:1259–66 7. Parmely WW. Cost-effective cardiology: cost-effective management of heart failure. Clin Cardiol 1996;19:240 –2. 8. Fonarow GC, Stevenson LW, Walden JA, et al. Impact of a comprehensive management program on the hospital readmission and functional status of patients with advanced heart failure. J Am Coll Cardiol 1997;30:725–32. 9. Rich MW, Beckham V, Wittenberg C, Leven CL, Freedland K, Carney RM. A multidisciplinary intervention to prevent the readmission of elderly patients with congestive heart failure. N Engl J Med 1995;333:1190 –5. 10. Hanumanthu S, Butler J, Chomsky D, Davis S, Wilson JR. Effect of heart failure program on hospitalization frequency and exercise tolerance. Circulation 1997;96:2842–8. 11. Shah NB, Der E, Ruggiero C, Heidenreich PA, Massie BM. Prevention of hospitalizations for heart failure with an interactive home monitoring program. Am Heart J 1998;135:373–8. 12. West JA, Miller NH, Parker KM, et al. A comprehensive management system for heart failure improves clinical outcomes and reduces medical resource utilization. Am J Cardiol 1997;79:58 –63. 13. Opasich C, Tavazzi L. Di fronte alla nuova pandemia: quale organizzazione per la cura del pazienti con insufficienza cardiaca? Cardiologia 1999;33:554 –65. 14. Schulman KA, Mark D, Califf RM. Outcomes and costs within a disease management program for advanced congestive heart failure. Am Heart J 1998;135:S285–92. 15. Havranek EP, McGovern KM, Weinberger J, Bracato A, Lowes BD, Abraham WT. Patient preferences for heart failure treatment: utilities are valid measures of health-related quality of life in heart failure. J Card Fail 1999;5:85–91. 16. Williams JF, Bristow MR, Fowler MB, et al. Guidelines for the evaluation and management of heart failure. Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Evaluation and Management of Heart Failure). J Am Coll Cardiol 1995;26:1376 –98. 17. Wilson MC, Hayward RS, Tunis SR, Bass EB, Guyatt G. User’s guides to the medical literature. VIII. How to use clinical practice guidelines. B. What are the recommendations and will they help you in caring for your patients? The Evidence-Based Medicine Working Group. JAMA 1995;274:1630 –2. 18. Sackett DL. Evidence-based medicine and treatment choices. Lancet 1997;349:570. 19. Sackett DL, Straus SE. Finding and applying evidence during clinical rounds: the “evidence cart.” JAMA 1998;280:1336 –8. 20. Petrolini J, Walden D. Planning projects and tasks using the 9 steps. Center Quality Manage J 2000;9:3–16. 21. Weinstein M, Stason WB. Foundations of cost-effectiveness analysis for health and medical practices. N Engl J Med 1977;296:716 –21. 22. I farmaci del servizio sanitario nazionale. Anno I—N 1/2001 Ministero della Sanità, Istituto Poligrafico e zecca dello Stato. 23. Drummond MF, Stoddart GL, Torrance GW. Methods for the Economic Evaluation of Health Care Programmes. Oxford, UK: Oxford University Press, 1987. 24. Lee ET. Statistical Methods for Survival Data Analysis. New York, NY: John Wiley, 1992. 25. Hershberger RE, Ni H, Nauman DJ, et al. Prospective evaluation of an outpatient heart failure management program. J Card Fail 2001;7: 64 –74. 26. Weinberger M, Oddone EZ, Henderson WG, for the Veterans Affairs cooperative study on primary care and hospital readmission. Does increased access to primary care reduce hospital readmissions? N Engl J Med 1996;334:1441–7. 27. Banker RD, Charnes A, Cooper WW. Some models for estimating technical and scale inefficiencies in data envelopment analysis. Manage Sci 1984;30:1078 –92. 28. Magnussen J. Efficiency measurement and the operationalization of hospital production. Health Serv Res 1996;31:21–37. 29. Tavazzi L. Significance of the BRING-UP studies. Ital Heart J 2000;1 Suppl:1038 – 42. 30. Berry E, Kelly S, Hutton J, et al. Intravascular ultrasound-guided interventions in coronary artery disease: a systematic literature review, with decision-analytic modeling, of outcomes and cost-effectiveness. Health Technol Assess 2000;4:1–117.