Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Myocardial infarction wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Electrocardiography wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
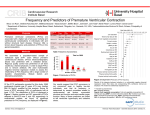
TECHNION – Israel Institute of Technology Department of Electrical Engineering Physiological Signal Processing Laboratory dLldLLaboratory PVC definition (pvb , ves) Ectopic (premature) ventricular complexes (PVCs) Some patients will have regular QRS complexes interspersed with occasional unusual-looking complexes. These unusual conformations are called PVCs This aberrant activity can cause more serious ventricular arrhythmias. Clinical deterioration depends on the frequency of the PVCs. A PVC is a depolarization that arises in either ventricle before the next expected sinus beat, i.e., prematurely. It may result from the firing of an automatic focus or reentry. Since PVCs originate in the ventricle, the normal sequence of ventricular depolarization is altered, i.e., instead of the two ventricles depolarizing simultaneously, they depolarize sequentially. In addition, conduction occurs more slowly through the myocardium than through specialized conduction pathways. This results in a wide (0.12 second or greater) and bizarre-appearing QRS. The sequence of repolarization is also altered, usually resulting in an ST segment and T wave in a direction opposite to the QRS complex. The interval between the previous normal beat and the PVC (the coupling interval) usually remains constant when PVCs are due to reentry from the same focus (uniform VCs). When the coupling interval and the QRS morphology vary, the PVCs may be arising from different areas within the ventricles, or if the PVCs are arising from a single focus, ventricular conduction may vary. Such PVCs are referred to as multifocal or more appropriately, multiformed. A PVC may occur nearly simultaneously with the firing of the sinus node. The antegrade impulse originating in the sinus node (resulting in normal atrial depolarization) and the retrograde impulse traveling toward the atria from the ventricles may meet in the AV node. Then neither can spread further because of the other's refractory period. Since the rhythm of the sinus node is undisturbed, a fully compensatory pause usually results (i.e., the next P wave should occur at the proper time.) However, on occasion, retrograde conduction can spread to the atria and reset the SA node. PVCs may occur as isolated complexes, or they may occur repetitively in pairs (two PVCs in a row). When three or more PVCs occur in a row, VT is present. When VT lasts for more than 30 seconds, it is arbitrarily defined as sustained ventricular tachycardia. If every other beat is a PVC, ventricular bigeminy is present. If every third beat is a PVC, the term ventricular trigeminy is used. If every fourth beat is a PVC, ventricular quadigeminy is present, and so forth. A PVC that falls on the T wave (during the so-called vulnerable period of ventricular repolarization) may precipitate VT or VF. However, PVCs occurring after the T wave may also initiate such VT. Simple PVCs Simple PVCs have the following characteristics: Occur beyond the T wave of the preceding QRS complex Morphology is uniform Occur in an isolated fashion and do not present in pairs or triplets Generally exhibit constant coupling intervals with the preceding QRS complex. This type of PVC is frequent in the general population and, as age increases, the frequency of such PVCs increases; approximately 70 percent of persons between the ages of 40 and 60 have simple PVCs, and they are seen in most individuals over the age of 60. Simple PVCs that occur in persons without any type of cardiac disease do not require treatment. However, it is important not to overlook the fact that the majority of sudden deaths occur in persons who were previously believed to be healthy and normal. Therefore, when confronted with a patient with simple PVCs, the physician must rule out any associated cardiac or electrolyte abnormalities that may predispose the patient to sudden death. If the physician is confident that there is no associated heart disease, then this type of PVC should not place the patient at increased risk for sudden death. Complex PVCs Complex ventricular ectopy can be defined as PVCs that: Occur in pairs, triplets or more prolonged runs of ventricular tachycardia Fall in the vulnerable period of the cardiac cycle (R on T) Have more than one morphology A close correlation exists between the complexity of PVCs and the risk of developing ventricular tachycardia and fibrillation in patients with cardiac disease. Patients who have complex ventricular ectopy without apparent cardiac disease only rarely experience life-threatening ventricular arrhythmias. Summary of ECG criteria QRS: Not normal looking. Usually broadened to more than 0.12 second. Rhythm: Irregular. P waves: The sinus P wave is usually obscured by the QRS, ST segment or T wave of the PVC. It may, however, sometimes be recognized as a notching during the ST segment or T wave. Retrograde P waves may occur. The presence of a sinus P wave (when it cannot be seen) may be inferred by the presence of a fully compensatory pause. PVC This ventricular ectopic - or premature ventricular contraction (PVC) - has had an effect on all three traces in the above diagram: The ECG QRS earlier than expected (premature) i.e. shorter RR interval than normal QRS wider than normal (usually more than 0.12 sec) QRS voltage higher than normal inverted T wave obscured P wave next RR interval longer than normal The arterial pressure ejection earlier than expected low systolic pressure generated The CVP large a wave a wave at expected time(not premature) Characteristics of (most) PVCs wide and bizarre QRS, often with a high voltage and inverted T wave reduced or no left ventricular ejection large CVP a wave fully compensatory pause Not all PVCs are followed by a pause. If a PVC occurs early enough (especially if the heart rate is slow), it may appear sandwiched in between two normal beats. This is called an interpolated PVC. The sinus impulse following the PVC may be conducted with a longer PR interval because of retrograde concealed conduction by the PVC into the AV junction slowing subsequent conduction of the sinus impulse. Wavelets transform http://engineering.rowan.edu/~polikar/WAVELETS/WTtutorial.html