Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
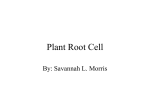
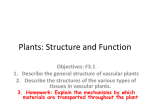
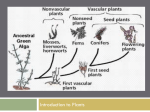
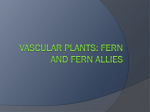
Five Rivers Vascular Network Operational Policy Introduction With the drive by the Vascular Society of Great Britain and Ireland (VSGBI) to halve the elective mortality rate for Abdominal Aortic Aneurysm (AAA) surgery by 2013, the framework for improvement of quality for elective AAA repair recommended that hospitals undertaking fewer than 100 elective AAA interventions in a three year period should not continue to offer these procedures. The Ipswich and Colchester hospitals have worked together successfully since April 2007 to provide an emergency (unplanned) vascular surgery service to people living in the areas of east Suffolk, north east Essex and the Colne Valley, serving a population overall in excess of 700,000 Subsequently, to achieve optimal surgical outcomes, all major arterial and all emergency vascular surgery was centralised to the Colchester Hospital University Foundation Trust (CHUFT) site as from July 2012. An Abdominal Aortic Aneurysm (AAA) screening service was also set up in April 2012 as part of the National AAA Screening Programme to incorporate North East Essex, East Suffolk and parts of Mid Essex in the Colne Valley. Following the review by the Royal College of Surgeons in June 2014 a number of recommendations and changes in service provision have been made. These have been included in this operational policy and are denoted as (RCS) Patient Cohorts All major arterial surgery is undertaken at the Colchester Hospital site. This includes: AAA Surgery (Open, Laparoscopic, and EVAR’s) Carotid surgery Arterial surgical procedures. All emergency vascular referrals from IHT site will be treated and transferred for definitive treatment at CGH site. In addition a staged move of interventional radiology from IHT to the CGH site is planned as capacity is developed ( RCS ). The Vascular team Mr Adam Howard is the Clinical Lead for Vascular Network and is responsible for the clinical organization and governance of the service, with reporting relationships to the clinical management in both trusts. The Network has a fulltime service manager, Mrs R Burt who has day to day management responsibility for working with the clinical lead in the organisation of the service Vascular network operational policy December 2014 V1 AH/JB Page 1 and the development of future plans. Mr S Choksy is the Director of the AAA Screening programme and Mr A Assar the MDT convenor. Consultant Vascular Surgeons The 6 Vascular Surgeons are partnered in two teams of three consultants to provide optimal cross-cover as follows: Abdusalam Abu-Own, Chris Backhouse and Sohail Choksy Adam Howard, Isam Osman and Ahmed Assar As far as practicable the teams provide cover for fixed hybrid theatre. If sessions cannot be covered in this way the other team will be involved in using the lists. Annual and study leave will be booked in accordance with the leave policy and notified to the vascular service manager for coordination a minimum of 6 weeks in advance. Cover for emergencies and at the two sites is as follows: Vascular Surgeon on-call (VSOC) The Vascular Surgeon on call will be based at CGH between 8.00am and 6.00pm Monday to Friday and weekend day mornings for ward rounds. The VSOC will manage all aspects of the emergency vascular service at both sites (RCS). The oncall team (consultant and SpR) will be available for emergency opinion (telephone or in person) for any emergency within 30 minutes. All six surgeons contribute equally to the VSOC rota. Vascular Surgeon for the wards (VSW) at IHT site At the Ipswich site there will be a presence from one of the vascular consultants or middle grade (VSW) on site during most sessions 9am-5pm Monday to Friday. They can be contacted via switchboard rota. The VSW should be contacted for urgent and elective referralsemergencies should be triaged via the VSOC as above. Occasionally surgeons in other specialties undertaking otherwise routine elective and emergency procedures require the assistance of a vascular surgeon to address extreme bleeding problems .In the event of a vascular emergency presenting at IHT site (e.g. uncontrolled bleed in theatre) then the VSW surgeon will respond whilst the VSOC is contacted. Conversely,if the VSW is not available for non-emergency cases the VSOC will be contacted. Generally the historically IHT based surgeons have provided the majority of this cover however a schedule for rotation of all surgeons to the IHT is under development and will be commenced in January 2015.(RCS) A summary rota for the vascular teams across the network including VSOC and VSW is held by switchboard at both IHT and CHUFT sites. Vascular Anaesthetists Scheduled lists in the Hybrid theatre are normally be covered by experienced vascular anaesthetists drawn from the CGH and IHT Vascular network operational policy December 2014 V1 AH/JB Page 2 anaesthetic departments as follows: Colchester: Ipswich: Peter Patient, Simon McKenzie, Tamas Malaj Ian Driver, Prakesh Bhagwat In addition to theatre sessions the vascular anaesthetic team attends vascular MDT on a rotating basis and undertake pre-operative assessments on high risk patients. Vascular Interventional Radiology There are six Consultant Vascular Interventional Radiologists who provide a 1:6 rota for emergency vascular radiology cover, four of whom undertake EVARs and attend the MDT meetings. Colchester: Ipswich: Arun Sebastian, Nagendra Thayur, Mohammed Al-Dabbagh Gary Picken, Avi Basu, Patrick Whitear The vascular interventional radiology service includes all aspects of emergency and elective interventional radiology that relates to the treatment of vascular conditions. This includes provision of a 24hr on call radiology nurse to support the Consultant Radiologist rota. The guidance from the BSR states that elective IR, non-EVARs and noncombined procedures could stay in the local hospital. However, all high risk cases will be discussed by the MDT and a decision made by the MDT on the appropriateness of undertaking the procedure on the nonemergency site In addition all interventional radiology procedures arising from emergency admissions will be undertaken at CGH. Any planned high risk procedure at IHT site have an available VSW for support.(RCS) with a plan to centralize all such procedures as capacity increases at the CGH site. Junior Medical staffing Junior medical staff training is undertaken across the network. A hybrid middle grade rota commenced in December 2014 which ensures dedicated middle grade cover for vascular emergencies at the CGH site with support from the general surgical rota with a view to fully dedicated rota being developed in 2015. Nursing support and Clinical Nurse Specialist The vascular ward at CGH site has developed a strong cohort of nursing staff with specialist skills in caring for vascular patients. Both sites have support from clinical nurse specialists who provide five main domains of specialist practice, namely patient care, information, education research and management. They possess advanced knowledge and skills in the field of vascular surgery including advanced communication skills and provide a pivotal role Vascular network operational policy December 2014 V1 AH/JB Page 3 in the team. Specialist Podiatrist There are specialist vascular podiatrists at both sites who also contribute to the diabetes MDT work. Multi-Disciplinary Team Arrangements Key decisions on the planning and optimisation of patient care for all major elective cases will be made within the framework of a structured Multidisciplinary Team (MDT). The MDT comprises: Consultant Vascular Surgeons Consultant Interventional Vascular Radiologists Vascular Clinical Nurse Specialists Consultant Anaesthetist Vascular Admissions Officer Attendance at MDT is not discretionary for surgeons or the radiologists who perform EVAR procedures. One Anaesthetist will normally attend all MDT meetings. The group will meet every Wednesday afternoon from 14.00hrs to 17.00hrs. Meetings will utilise teleconferencing facilities in the Colchester Telemedicine room, linked with the diagnostic telemedicine room at IHT. Meetings will be chaired by a MDT lead consultant and supported by the Vascular MDT Co-ordinator. The schedule of required information for each case under review at the MDT is included at Appendix 4. Decisions of the MDT on individual patient treatments will be recorded in the patient notes and in a formal record of each meeting. Patient Pathways The principle routes into the service are: Elective Pathway: GP referral Ward referral Clinic referral referral via the AAA screening Programme tertiary referrals: nationally for laparoscopic vascular surgery and thoracic outlet compression syndrome Vascular network operational policy December 2014 V1 AH/JB Page 4 Elective patients There is an integrated referral pathway across the network where referrals are received from different sources at both sites. Urgent cases are pooled via the MDT to allow optimal treatment times. All elective patients for vascular surgery and interventional radiology are discussed in the MDT and are treated in accordance with the 18 week pathway across the network. (RCS) GP Outpatient Referral Primary care referrals for patients requiring a vascular specialist opinion will be made to the contact centre at CHUFT or the call centre at Ipswich Hospital Trust (IHT). Referrals are prioritised as appropriate from information in the GP communication and assigned to a Consultant and a clinic appointment. Screening Programme referral Patients identified from the screening programme with abnormal aortic features will be referred to the next available consultant outpatient slot. Essex residents will normally be given CHUFT appointments; Suffolk residents will normally be given IHT appointments. The referral should be made by the co-ordinator within one working day of the screening clinic, with a referral letter being sent directly to the secretary of the vascular surgeon. Mr Choksy director of AAA screening ensures an equal rotation of AAA referrals to each consultant. All referrals should be seen in vascular outpatients within two weeks of the referral. If the AAA has a diameter of over 7.5cm, an urgent referral should be made with a view of seeing the patient at the next available outpatient clinic- which will be within 2 weeks, followed by urgent risk assessment and discussion at the MDT. Patients from the screening programme will follow a common elective pathway as those from GP referral once in the outpatient assessment pathway. Outpatient Appointment The first outpatient appointment will be held wherever possible at the patient’s local hospital unless urgency of the situation dictates otherwise. Patient assessment within the outpatient department will follow an agreed vascular assessment pathway and use common documentation. (Appendix 2) Diagnostics Patients who are being investigated for major arterial conditions will be subject to an agreed selection of diagnostics as outlined in the pathway documentation. (Appendix 2) All diagnostic testing other than CPEX will be carried out at the patient’s local hospital. Patient requires major arterial surgery Patients will be added to the waiting list following their outpatient appointment Vascular network operational policy December 2014 V1 AH/JB Page 5 and/or following discussion at MDT. All major arterial surgery patient treatment plans will be reviewed by the weekly MDT. Following the MDT the patient will formally transfer to CHUFT clinical administration system. Vascular network operational policy December 2014 V1 AH/JB Page 6 The Vascular Admissions Officer/ MDT coordinator will then work with the consultant concerned to ensure that the administration of the next stages of the patient’s care is planned and communicated to all parties appropriately. Following the MDT review any IHT patient will be added to the CHUFT IP waiting list; their Referral to Treatment pathway will continue from the initial referral point. The vascular admissions officer will agree the date for surgery with the respective consultants, and organise a pre-operative assessment appointment. 3.1.6 Anaesthetic Risk Assessment Some patients will require an extensive pre-operative anaesthetic assessment. This will be organised at the discretion of the surgeon in charge of the case. This will be undertaken on the local hospital site and be arranged in accordance with the agreed documentation and assessment procedures as shown in Appendix 3 3.1.7 Pre-Operative Assessment The pre-operative assessment (POA) will be carried out at either site, though where possible in the POA suite in the Elective care centre (ECC) at CHUFT for all major arterial surgical cases. POA will routinely be conducted by the POA nurses, with anaesthetic input for patients that require this. All major vascular cases will reviewed by a Consultant Anaeasthetist in this clinic at both sites.(RCS) All cardio pulmonary exercise testing, (CPEX) will be carried out at CHUFT for patients requiring this such as all AAA patients. 3.1.8 Admission Patients, where possible, subject to clinical suitability, will be admitted on the day of surgery via the Elective Care Centre at CHUFT. Major cases will be admitted and managed on Wivenhoe ward, the designated vascular surgical ward at an agreed time prior to surgery. The ward is divided to provide clean bays and side rooms rather than separating elective and non- elective cases to maintain good infection control practices, whilst maintaining same sex accommodation. Only clean non-vascular patients should be admitted onto the ward in the event of unused bed base .In 2015 refurbishment of the ward is planned with production of 4 bedded bays an improved shower/toilet facilities. ( RCS) There may be exceptions to this, for example, stroke patients who will go to theatre from the stroke unit and be managed post operatively on Wivenhoe ward. On the IHT site complex medical patients with vascular problems under the care of medical teams will be reviewed by the VSW team regularly. It is important to note that at both sites a minority of patients cared for by vascular consultant team will have general surgical problems or undergoing rehabilitation (RCS) 3.1.9 Theatre Scheduling Following MDT review the patient will be booked on the theatre web system by the vascular booking clerk who will have access to the theatre session Vascular network operational policy December 2014 V1 AH/JB Page 7 timetabling in line with the patient access policy. Any list changes should be entered on to the theatre web by the booking clerk as they occur and wherever possible by 12:00 noon the day prior to the session as per the CHUFT ‘Operating List Booking Procedure’ (Policy 283). If a surgeon is unable to undertake a planned operating session the vascular speciality should make every effort to cover the session internally. When a session reallocation within the speciality is not possible, the Main Theatre receptionist or deputy who attends the weekly rota meeting will have the opportunity to offer any available sessions to alternative specialities up until the two-week cut off point. Emergency patient pathway Emergency Pathway: Referral via Emergency department (ED ‘Blue Light’) or Emergency Assessment Units (EAU GP referred) Ward Reviews and internal transfers- Assessment units, Management and Transfer of emergency patients between sites ( RCS) is outlined in the following guidance including bypass criteria: Standard Operating Procedure: Five Rivers Vascular Network Obtaining timely advice and intervention for emergency and urgent vascular cases at IHT Emergency Department: IHT Inpatients, Intraoperative emergencies, Ward and OPD emergencies Ambulance Protocol for the Conveyance of Vascular Emergencies East of England Ambulance Service and Five Rivers Vascular Network East Suffolk vascular (AAA) pathway- primary divert (Ipswich Hospital) Flowcharts showing the core pathway elements are attached.(Appendix 1b). Emergencies to the vascular service may also arise from other hospital services at CHUFT and IHT, including: Stroke patients requiring revascularisation procedures Diabetic patients requiring revascularisation procedures/amputations Patients on general wards requiring vascular management e.g. revascularisation, ulcer management, etc. Intraoperative surgical cases requiring urgent specialist vascular support in theatre The network has set new standards for management of emergency patients to ensure timely transfer to definitive treatment ( RCS). Vascular network operational policy December 2014 V1 AH/JB Page 8 Emergency cases such as ruptured AAA should reach theatres in 90 minutes of ED referral and ischemic limbs that require surgery should reach theatre within 6 hours of ED referral. Cases requiring immediate (life/limb saving) Surgical Intervention Cases requiring emergency immediate surgery will normally be admitted through the CGH A&E services, reviewed by the Vascular Surgeon, and routed via diagnostic CT to the operating theatre using the CEPOD list (In hours, M-F 9-5) or the emergency theatre team (at other times). It may, in some cases, require the Vascular Theatre to be opened for these cases if the fixed angiography equipment (C-arm) is to be used in treatment (e.g. emergency EVARs) For emergency patients it is the responsibility of the vascular consultant on call to ensure that the patient details are entered onto theatre web prior to the patient leaving the operating theatre. Cases that require urgent treatment Lists in the Vascular Theatre on Wednesdays (9 to 5) will be available for all urgent cases (e.g. CEAs, amputations, debridement, etc.). Otherwise cases will be allocated to available capacity on planned vascular lists or use the CEPOD list dependent on clinical need. Multiple trauma The VSOC will be required to support multiple trauma cases, involving vascular damage at both CGH and IH. During Monday to Friday 8-6pm first line major trauma support at IH will be available via the IH Based VSW on site (see 3.2.1.2 above) Vascular network operational policy December 2014 V1 AH/JB Page 9 Critical care and extended recovery There is provision for 13 critical care beds at CHUFT in addition to a 24 hour theatre recovery, to support further high dependency care Medical management on critical care unit Medical management within critical care is led by the Critical Care team (intensivists and anaesthetists),with the parent team (and other teams) being consulted when needed. The admission and discharge of patients is decided by the CC team in liaison with the parent team. Post-operative patient pathways Model patient pathways and documentation has been agreed for use with all vascular ward patients. Details are included in Appendix 5. Repatriation A repatriation protocol has been developed to support the Network and has been agreed between the trusts. The protocol is designed to operate when a Suffolk domiciled patient is surgically fit to leave the vascular unit at CGH but requires some element of on-going medical management, which can be given in a setting closer to their home family and friends. The decision to repatriate will be taken by the patient’s consultant. Therapy and rehabilitation services Patients will receive general physiotherapy as inpatients as required. Patients repatriated back to Ipswich hospital will require a discharge handover report. Patients who are discharged home out of area will be referred to Suffolk PCT for further rehab if required. Amputees are currently referred to CGH for prosthetic rehab if they are within NEEPCT. Suffolk PCT have a contract with Norfolk and Norwich for prosthetic care so these patients will need to be referred there on discharge. Diabetic Foot service The diabetic foot service at both sites is NICE complaint. Vascular network operational policy December 2014 V1 AH/JB Page 10 Outpatients with intermittent claudication are assessed by the vascular consultants or CNS. Those deemed suitable for the exercise class attend twice weekly for 8 weeks and are then reassessed. Discharge management Patients will be discharged from Colchester and IHT will receive a copy of their discharge letter and appropriate medications, plus a discharge information leaflet and will be asked to complete the electronic patient discharge questionnaire survey. Outpatient and telephone follow up arrangements Patients will be followed up at the hospital OPD nearest their home. For patients who have had an AAA repair they will also receive a telephone follow up from their consultant or designated substitute three to four days following discharge from hospital. The telephone contact will be documents using the pathway template (Appendix 6) When patients are transferred between sites, either for surgery or repatriation purposes, the vascular health records and discharge summary will be copied in their entirety and sent to the receiving hospital either via a secure fax or a contract taxi will need to be booked through the service desk. Discharge summaries are sent electronically to the GP. A further copy is given to the patient and a copy is retained in the patient notes and a copy faxed to IHT hospital for uploading onto the evolve electronic health record system. Network Governance and Audit Vascular Services are managed within the Surgical Division at CHUFT. The centralised services referred to in this policy will form part of the overall responsibility of that division under the leadership of the Associate Director and Divisional Director working in close conjunction with the Director of Surgery at the IHT site. The Clinical Lead co-ordinates governance issues relating to vascular services across the network and reports to the Surgical Divisional Governance meeting. All vascular staff can report incidents via the CHUFT DATIX system and incidents from IHT site are reported at the governance meeting. All consultants are encouraged to become incident investigators and undertake Serious Incident investigation training. All deaths are to be reported on the DATIX system for tracking purposes. All staff are expected to be up-to-date with mandatory training. Key Quality performance indicators have been developed and incorporated into a dashboard to monitor service provision across the network and are reviewed at the service governance meetings along with other relevant action plans. There are monthly governance meetings which cover various areas e.g. risk, incidents, complaints. Vascular network operational policy December 2014 V1 AH/JB Page 11 Whilst clinically the vascular service is substantially separated from general surgery, junior medical staffing arrangements will require continued close liaison with the colorectal and GI service clinical teams at both CGH and IH AAA Screening Programme Separate standard operating procedures exist for the AAA screening programme, which complies with the NAAASP requirements and are in operation. Audit Morbidity and mortality audits are undertaken monthly and there is also a quarterly combined audit meeting with the critical care team at CHUFT. An annual audit plan has been agreed. National Vascular Database All patients undergoing reference procedure surgery will be reported to the National vascular database. The vascular surgical team (consultants, middle grade and nurse specialists) are responsible for inputting data following the patient’s surgery. Any complications that may occur are updated and the information is submitted once the patient has been discharged. Follow up data is completed after outpatient follow up assessment. Vascular network operational policy December 2014 V1 AH/JB Page 12 15 Patient Experience Patient communication leaflets have been developed to assist patients with their pathway through treatment. Whilst patients are in hospital on the vascular ward they are provided with a .patient discharge leaflet, their discharge summary and appropriate advice. Patient are asked to complete an electronic patient discharge questionnaire survey to audit patient satisfaction and feedback on care. 16 Financial Arrangements Agreement has been reached between CHUFT and IHT in relation to the management of income and expenditure arising from the service model. Income will accrue to the site on which the activity takes place. The service model requires consultants and other staff to cover services at both sites. Arrangements will be made and reviewed annually between the trusts for payment for services rendered at the non-employing hospital site APPENDIX 1a Model elective patient pathway flow chart for elective admission 1b Model emergency patient pathway flow chart for emergency admission 2a Patient pathway document for outpatient department assessment 2b Patient pathway document for outpatient AAA safe intervention outpatient 3 Patient pathway document for vascular pre-admission clinic assessment 4a Patient pathway document for vascular MDT assessment for AAA/limb intervention/other 4b Patient pathway document for vascular MDT assessment for Carotids 5 Patient pathway document for vascular post-operative patient document 6 Patient pathway document for AAA telephone follow up 7 Vascular surgeons, anaesthetists and hybrid theatre timetable Vascular network operational policy December 2014 V1 AH/JB Page 13 Appendix 1a Model elective patient pathway flow chart for elective admission AAA SCREENING ABNORMALITY IDENTIFIED GP REFERRAL CGH IHT ESSEX RESIDENT IHT OPD 1st APPOINTMENT CGH OPD 1st APPOINTMENT IHT DIAGNOSTICS CGH DIAGNOSTICS OPD REVIEW CONSIDERING SURGERY SUFFOLK RESIDENT OPD REVIEW CONSIDERING SURGERY REFER TO MDT MDT DISCUSSION/ AGREEMENT ON MANAGEMENT NON-SURGICAL MANAGEMENT BY LOCAL SERVICE SURGICAL MANAGEMENT VIA CGH Vascular network operational policy December 2014 V1 AH/JB Page 14 Appendix 1b Model emergency patient pathway flow chart for emergency admission NORTH EAST ESSEX RESIDENTS EAST SUFFOLK RESIDENTS EoEAS diagnosed vascular case Urgent Vascular Clinic Referral CGH Ward referral CGH GP Referred via EAU CGH A&E presentation IHT A&E presentation IHT GP Referred via EAU Review by VSOC Review by VSOC Review by GS Reg and/or VSOC Review by A&E Consultant then GS Reg and VSOC Review by A&E Consultant Review by GS Reg discuss with VSOC Stabilise Diagnostics Accept referral as vascular case Remain with physicians NO Accept referral as vascular case IHT Ward referral Review by VSW on site Arrange transfer to CGH if needed YES NO YES Stabilise Diagnostics Stabilise Diagnostics CGH SAU hold – waiting for bed or prepare for theatre CGH A&E hold – waiting for bed or prepare for theatre Ward Admission under VSOC Straight to Theatre under VSOC (CEPOD List) EoEAS transfer to CGH Remain with IHT physicians Urgent theatre or Radiology Vascular network operational policy December 2014 V1 AH/JB Page 15 2a Patient pathway document for outpatient department assessment Vascular network operational policy December 2014 V1 AH/JB Page 16 Reference WOE1334 Issue date May 2012 a Vascular (Arterial) Outpatient Clinic Hospital/NHS number Consultant Patient label Patients name OPCS code Presenting complaint Allergies & Intolerances Current vascular symptoms, complaints & history Duration Left Right Bilateral Past Endovascular / vascular surgery & interventions Year Previous anaesthetic problems? No Yes – specify: Vascular risk factors / conditions Smoker per day for years Diabetes Hypertension CABG – coronary stent - date: / / Type: Hypercholesterolemia CCF / LVF - SOB on exercise: distance: Rheumatic fever Renal failure / disease – creatinine: DVT / PE Clotting disorder Venous skin changes Malignancy: () boxes that apply Ex-smoker - Given up for: years/months PVD / claudication – distance: yards / miles MI / Angina Valve replacement – mechanical? Yes No Stroke / TIA / Am. Fugax – date: / / Family history AAA dx Pacemaker AF / Arrhythmia – Warfarin? Yes No Varicose veins Venous ulcer Vascular Outpatient Clinic Limb claudication - claudication distance: yards/miles Leg or foot ulcers or tissue loss/gangrene Rest pain, toes / feet Night pain, toes / feet relieved by dependency Aortic Aneurysm (see details overleaf) TIA / CVA / Amaurosis Fugax / Asymptomatic Carotid Disease Popliteal Aneurysm Arm claudication/Raynaud’s Varicose veins (delete) – pain / skin changes / ulcer Others/details: Duodenal / gastric ulcer Vascular network operational policy December 2014 V1 AH/JB Page 17 Medications Cerebrovascular diagnosis () Dysphasia/other Symptomatic side Date TIA’s (Anterior / Posterior) CVA Amaurosis Fugax Vertebral disease CEA or Carotid stent Vascular network operational policy December 2014 V1 AH/JB Page 18 Record patient name & ID if photocopying this page: Aneurysmal disease IAAA / JAAA / SAAA / TAAA? No Yes – date: AAA surveillance? No Yes – date: / / date: / / No Yes – date: / / Diameter (cm) on Duplex / CT: Open operation / EVAR? / / Arterial complications: Vascular Outpatient Clinic Clinical examination Peripheral pulses / venous disease & tissue loss Draw location of arterial or venous ulcers / amputations Recent or clinic ABPI’s / Admission ABPI’s / or toe pressure (date / / ): Right = Carotid bruit: Right = Left = Left = Right Left Ulcers (arterial/venous) Rest pain Gangrene Buerger’s (+/-) Right Left Right Left Management plan & further action () Aspirin Clopidogrel Warfarin Statin Assasantin Dipyrimadole/ Persantin Vocal cord check (carotid surgery) Other: Vascular network operational policy December 2014 V1 AH/JB Page 19 Print name / designation Signature Grade Date / Vascular network operational policy December 2014 V1 AH/JB / Page 20 2b Patient pathway document for outpatient AAA safe intervention outpatient Vascular network operational policy December 2014 V1 AH/JB Page 21 Reference WOE1333 Issue date May 2012 b AAA Safe for intervention Outpatient checklist Please complete this checklist in the op clinic. Patient details Consultant Patient label Patients name Date of birth Pre-admission date / / / / Age Procedure date / / AAA Safe for intervention checklist Questions Y N Has the patient had a myocardial infarct or unstable angina/ angina at rest in the last 3 months? Has the patient had new onset of angina in the last 3 months? Does the patient have a history of poorly controlled heart failure? (nocturnal dyspnoea or inability to climb one flight of stairs due to SOB) Does the patient have severe or symptomatic cardiac valve disease? (e.g. Aortic stenosis with gradient >60mmHg or requiring valve replacement, drop attacks) Does the patient have significant arrhythmia? (Symptomatic, ventricular, severe bradyarrhythmias or uncontrolled supraventricular tachycardia) If available, does the patient have any of:1. FEV1 < 1.0 L or <80% of predicted value ; 2. PO2 < 8.0 kPa; 3. PCO2 > 6.5 kPa If the answer to any of 1 – 6 is yes, the patient is coded RED and is very high risk for surgery. Questions Y N Does the patient get SOBOE climbing one flight of stairs? (short slope if lives on one floor) Does the patient have evidence of moderate renal impairment (Creatinine >180 micromol/l) or previous renal transplant? Has the patient had treatment for cancer in last 6 months, or has life threatening tumour? Does the patient have poorly controlled diabetes mellitus? (HbAlc > 7.5%, blood sugar usually >10 mmol/l) Does the patient have uncontrolled hypertension (i.e. SBP >190; DBP >105) Has the patient had a TIA or CVA within the last 6 months? If the answer to any of 7-12 is yes, the patient is coded AMBER and is higher risk for intervention. Questions Y N If the answers to all of the above are no, the patient is coded GREEN and is fit to proceed, provided they are on appropriate preoperative medication Other Risk Factors Other risk factors that increase the risk (amber) or preclude (red) repair (circle): Yes / No (e.g. dementia, cancer, stoma, adhesions - specify if yes):……………………………….. Patient is coded: Proposed Action: Not recommended for immediate intervention – Specialist review required if Red surgical treatment still to be considered. Amber Significant comorbidity requiring preoperative optimisation. Green Fit to proceed to further stage of formal assessment Vascular network operational policy December 2014 V1 AH/JB Vascular AAA Safe for intervention checklist Hospital/NHS number Page 22 N.B. It is recommended that all patients scoring red or amber should be reviewed by an Anaesthetist with experience in Vascular anaesthesia prior to listing for intervention. Print name / Designation Signature Grade Date / Vascular network operational policy December 2014 V1 AH/JB / Page 23 3 Patient pathway document for vascular pre-admission clinic Vascular network operational policy December 2014 V1 AH/JB Page 24 Reference WOE1337 Issue date May 2012 Vascular Elective Pre-admission Clinic Please complete this checklist and write additional details or a traditional clerking in the patient's hospital notes. Patient details Hospital/NHS number Consultant Patient label Patients name / Planned procedure Dates - Pre-admission 1. 2. 3. 4. 5. / / Age OPSC code Open / Laparoscopic AAA / Endoleak repair EVAR Carotid Endarterectomy Bypass procedure: L R Other: / TCI / Clerking doctor / Procedure / / Nurse Allergies & intolerances Latex sensitivity? No Yes – theatre notified (if required) MRSA status Risk factors / conditions () boxes that apply Cardiovascular Venous Smoker per day for years Ex-smoker - Given up for years/months Diabetes PVD / claudication – distance: yards / miles Hypertension MI / Angina CABG – date: / / Valve replacement – mechanical? Yes No Hypercholesterolemia Stroke / TIA / Am. Fugax– date: / / CCF / LVF - SOB on exercise: distance: Family history AAA dx Rheumatic fever Pacemaker Renal failure / disease – creatinine: AF / Arrhythmia – Warfarin? Yes No General DVT / PE Clotting disorder Varicose veins Venous ulcer Venous skin changes Malignancy: Alcohol: units per week Epilepsy Chronic back pain Duodenal / gastric ulcer Hiatus hernia Gastritis / oesophagitis Jaundice Hepatitis Sickle Cell Hyper/hypo thyroidism Asthma / COPD / TB Erectile dysfunction Learning disabilities Current medication Drug Dose Frequency Vascular network operational policy December 2014 V1 AH/JB Drug Dose Vascular Elective Pre-admission Clinic Date of birth Frequency Page 25 Drug allergies: Medication to stop pre-operation: Warfarin OCP HRT Clopidogrel Dipyridamole Others: Vascular network operational policy December 2014 V1 AH/JB Page 26 Record patient name & ID if photocopying this page: Investigations requested (state reason if not requested) Pre-admission Clinic Blood tests WBC Hb Platelets INR Na K Urea Creatinine Random Glucose HbA1c LFT Coagulation screen MRSA screen Sickle cell Thyroid function Result Test Results ECG CXR* CPEX Respiratory function* Standard echo MUGA or stress echo* Carotid duplex Vein mapping Arterial limb duplex Other: * Not required unless unsuitable for CPEX or specifically indicated VTE Risk assessment VTE Risk assessment completed? No Yes – prophylaxis given? No Yes: Measurements for anti-embolism stockings: Calf: Ankle: Length: ERP? (For AAA) No Yes – Infacol / Nebs / Hibiscrub / Fresubin (delete) Physical examination Height Weight BMI BP L Pulse Resps O2 Sats Peak flow R Reg / Irreg CVS: GIS: RS: Local examination: Summary of further action Checklist Clexane None / 20mg / 40mg Drug chart completed? Yes / No Post-op analgesia? Yes / No Amputation care package given (if applicable)? Yes / No Previous or FH anaesthetic problems? Yes / No Nurse – print name Nurse signature Vascular network operational policy December 2014 V1 AH/JB Grade Date Page 27 Appendix 4a Patient pathway document for vascular MDT assessment for AAA/limb intervention/other Vascular network operational policy December 2014 V1 AH/JB Page 28 a WOE1336 Issue date June 2012 Vascular Multidisciplinary Team – AAA / Limb Intervention Vascular Multidisciplinary Team Proforma Elective AAA / Limb Intervention / Other Complete at MDT by Registrar. Patient details Team present Hospital number Surgeon Patient label NHS number Radiologist Patients full name Co-ordinator Date of birth / MDT meeting date / Age / Other: / Allergies / intolerances Medical risk factors () Risk Details Cardiac impairment Respiratory impairment Renal impairment Other (e.g. malignancy) Investigations completed (state reason if not requested) () Risk Significant details of results (N = normal / A = abnormal) FBC HbA1c (if diabetic) U&E LFT Coagulation screen MRSA screen ECG CXR Vascular network operational policy December 2014 V1 AH/JB Page 29 Mortality risk: CPEX % AT: Ventilatory equivalent: normal / abnormal Respiratory function* Standard echo MUGA or stress echo* * Not required unless unsuitable for CPEX or specifically indicated Vascular network operational policy December 2014 V1 AH/JB Page 30 Appendix 4b Patient pathway document for vascular MDT assessment for Carotids Vascular network operational policy December 2014 V1 AH/JB Page 31 WOE1335 Issue date May 2012 b Vascular Multidisciplinary Team Carotid disease Complete at MDT by Registrar. Patient details Team present Hospital number Surgeon Patient label NHS number Radiologist Patients full name Co-ordinator Date of birth / / MDT meeting date Age / Other: / Allergies / intolerances No Yes – date: Thrombolysis? / / Carotid checklist Indication for surgery Affected area L Side R Date of event Amaurosis Fugax Transient ischaemic attack (TIA) Stroke Asymptomatic Other: Current neurological status (TIA’s only) ABCD2 score If ABCD ≥ 4 then 48 hours. If ABCD < 4 then 2 weeks. 2 2 Score Age ≥60 years 1 Blood pressure ≥140/90 mmHg Any unilateral weakness (face/hand/arm/leg) Speech disturbance (without motor weakness) ≥60 minutes 10-59 minutes Yes 1 2 1 2 1 1 Clinical features Duration of symptoms Diabetes mellitus Vascular Multidisciplinary Team – Carotid Disease Reference Score given Total Rankin Score Vascular network operational policy December 2014 V1 AH/JB Score Page 32 No symptoms at all. No significant disability despite symptoms; able to carry out all usual duties and activities. Slight disability; unable to carry out all previous activities but able to look after own affairs without assistance. Moderate disability; requiring some help but able to walk without assistance. Moderately severe disability; unable to walk without assistance and unable to attend to own bodily needs without assistance. Severe disability; bedridden, incontinent and enquiring constant nursing care and attention. Vascular network operational policy December 2014 V1 AH/JB 0 1 2 3 4 5 Page 33 Appendix 5 Patient pathway document for vascular post-operative patient document Vascular network operational policy December 2014 V1 AH/JB Page 34 Reference WOE1331 Issue date May 2012 Operation Vascular Procedure Diagram & Codes To be used with the Theatre ICP Patient details Affix patient label below Consultant Hospital/NHS № Patient label Operation procedure diagram & codes Patients full name Date of birth / / Age Operative diagram PTA Site(s) EVAR Stent details Closure devices used & site Comments: Bed rest duration hours Radiologist name Vascular network operational policy December 2014 V1 AH/JB Page 35 Radiologist sign Vascular network operational policy December 2014 V1 AH/JB Page 36 Record patient name & ID f photocopying this page: Tick codes used in this patient’s pathway. If procedure is not listed below, look at full laminated list and record in the blank row at the bottom of this page. (Red = Level 3 Blue = Level 4) Procedure codes – Code AORTA A75.2 Excision of thoracic sympathetic nerve A79.2 Destruction of thoracic sympathetic nerve NEC Emergency replacement of aneurysmal segment of thoracic aorta by L18.2 anastomosis of aorta to aorta NEC Emergency replacement of aneurysmal segment of suprarenal abdominal aorta L18.3 by anastomosis of aorta to aorta Emergency replacement of aneurysmal segment of abdominal aorta by L18.5 anastomosis of aorta to aorta NEC Emergency replacement of aneurysmal bifurcation of aorta by anastomosis of L18.6 aorta to iliac artery L18.8 Other specified emergency replacement of aneurysmal segment of aorta L18.9 Unspecified emergency replacement of aneurysmal segment of aorta L19.3 L19.4 L19.5 L19.6 L19.8 L19.9 L20.3 L20.6 L20.8 L20.9 L21.6 L21.8 L21.9 L25.8 L27.1 L27.3 L27.4 L27.5 L27.6 L27.8 L27.9 L28.1 L28.5 L28.6 L28.8 L28.9 Replacement of aneurysmal segment of suprarenal abdominal aorta by anastomosis of aorta to aorta NEC Replacement of aneurysmal segment of infrarenal abdominal aorta by anastomosis of aorta to aorta NEC Replacement of aneurysmal segment of abd. aorta by anastomosis of aorta to aorta NEC Replacement of aneurysmal bifurcation of aorta by anastomosis of aorta to iliac art. NEC Other specified other replacement of aneurysmal segment of aorta Unspecified other replacement of aneurysmal segment of aorta Emergency bypass of segment of suprarenal abd. aorta by anastomosis of aorta to aorta Emergency bypass of bifurcation of aorta by anastomosis of aorta to iliac artery NEC Other specified other emergency bypass of segment of aorta Unspecified other emergency bypass of segment of aorta Bypass of bifurcation of aorta by anastomosis of aorta to iliac artery NEC Other specified other bypass of segment of aorta Unspecified other bypass of segment of aorta Other specified other open operations on aorta Endovascular insertion of stent graft for infrarenal abdominal aortic aneurysm Endovascular insertion of stent graft for thoracic aortic aneurysm Endovascular insertion of stent graft for aortic dissection in any position Endovascular insertion of stent graft for aortic aneurysm of bifurcation Endovascular insertion of stent graft for aorto-uniiliac aneurysm Other specified transluminal insertion of stent graft for aneurysmal segment of aorta Unspecified transluminal insertion of stent graft for aneurysmal segment of aorta Endovascular stenting for infrarenal abdominal aortic aneurysm Endovascular stenting for aortic aneurysm of bifurcation NEC Endovascular stenting for aorto-uniiliac aneurysm Other specified transluminal operations on aneurysmal segment of aorta Unspecified transluminal operations on aneurysmal segment of aorta L42.4 Operations on aneurysm of renal artery L45.1 Bypass of visceral branch of abdominal aorta NEC Endarterectomy of visceral branch of abdominal aorta and patch repair of L45.3 visceral branch of abdominal aorta NEC L45.4 Endarterectomy of visceral branch of abdominal aorta NEC L46.4 Operations on aneurysm of visceral branch of abdominal aorta NEC Code CAROTID L29.1 Replacement of carotid artery using graft L29.3 Bypass to carotid artery NEC L29.4 Endarterectomy of carotid artery and patch repair of carotid artery L29.5 Endarterectomy of carotid artery NEC L29.8 Other specified reconstruction of carotid artery L31.1 Percutaneous transluminal angioplasty of carotid artery L31.2 Arteriography of carotid artery L31.8 Other specified transluminal operations on carotid artery L35.2 Arteriography of cerebral artery L29.9 Unspecified reconstruction of carotid artery Vascular network operational policy December 2014 V1 AH/JB Code L54.1 L54.2 LIMB Percutaneous transluminal angioplasty of iliac artery Percutaneous transluminal embolectomy of iliac artery L54.3 Arteriography of iliac artery L54.4 Percutaneous transluminal insertion of stent into iliac artery Bypass of femoral artery by anastomosis of femoral artery to femoral artery NEC Bypass of femoral artery by anastomosis of femoral artery to popliteal L59.2 artery using prosthesis NEC Bypass of femoral artery by anastomosis of femoral artery to popliteal L59.3 artery using vein graft NEC Bypass of femoral artery by anastomosis of femoral artery to tibial artery L59.4 using prosthesis NEC Bypass of femoral artery by anastomosis of femoral artery to tibial artery L59.5 using vein graft NEC Bypass of femoral artery by anastomosis of femoral artery to L59.6 peronealartery using prosthesis NEC Bypass of femoral artery by anastomosis of femoral artery to peroneal L59.7 artery using vein graft NEC L59.1 L60.1 Endarterectomy of femoral artery and patch repair of femoral artery L60.2 L62.2 Endarterectomy of femoral artery NEC Open embolectomy of femoral artery L63.1 Percutaneous transluminal angioplasty of femoral artery L63.4 Arteriography of femoral artery L66.5 L72.1 L74.2 L74.6 Code L75.1 L75.3 W06.1 Y53.1 Y53.2 Y53.3 Percutaneous transluminal balloon angioplasty of artery Arteriography NEC Creation of arteriovenous fistula NEC Creation of graft fistula for dialysis OTHER Excision of congenital arteriovenous malformation Embolisation of arteriovenous abnormality NEC Total excision of cervical rib Approach to organ under radiological control Approach to organ under ultrasonic control Approach to organ under CT scan control Y53.4 Approach to organ under fluoroscopic control Y53.5 Y53.6 Y53.7 Y74.2 Y75.2 Y78.1 Approach to organ under image intensifier Approach to organ under video control Approach to organ under MRI control Thoracoscopic approach to thoracic cavity NEC Laparoscopic approach to abdominal cavity NEC Arteriotomy approach to organ using image guidance with fluoroscopy Arteriotomy approach to organ using image guidance with image Y78.4 intensifier Y78.5 Arteriotomy approach to organ using image guidance with video control Y78.6 Z74.3 Z94.1 Z94.2 Z94.3 Code L76.1 L76.3 L82.1 L84.1 L84.2 L84.3 L85.1 L87.1 L87.2 L87.4 L88.1 L88.2 Arteriotomy approach to organ using image guidance with MRI control First rib excision Bilateral operation Right sided operation Left sided operation VENOUS Endovascular placement of one metallic stent Endovascular placement of two metallic stents Transposition of valve of vein Combined operations on primary long saphenous vein Combined operations on primary short saphenous vein Combined operations on primary long and short saphenous vein Ligation of long saphenous vein Stripping of long saphenous vein Stripping of short saphenous vein Avulsion of varicose vein of leg Percutaneous transluminal laser ablation of long saphenous vein Radiofrequency ablation of varicose vein of leg Page 37 L88.3 Vascular network operational policy December 2014 V1 AH/JB Percutaneous transluminal laser ablation of varicose vein of leg NEC Page 38 Appendix 6 Patient pathway document for AAA telephone follow up Vascular network operational policy December 2014 V1 AH/JB Page 39 Reference WOE1339 Issue date May 2012 AAA Telephone follow-up Patient details Affix patient label below Telephone followup date Hospital/NHS number Patient label Patients name / / Name of clinician carrying out telephone follow-up Operation date / / Signature / GMC № Discharge date / / Procedure Expected post-operative symptoms Patients will still be sore and having difficulty moving, but should be coping with oral painkillers. Does patient require painkillers? Yes Does patient require a flu vaccination? No Question Details / notes How are you feeling following your surgery? (If patient is feeling ill, clarify if it is pain or illness, such as upset tummy/chest problems/cough) Do you have a family member / carer looking after you? Yes No Telephone follow-up This proforma is to be used as a guide for telephone follow-ups for AAA procedures on patients who have been discharged from hospital 48hrs to 1 week after discharge (depending on a locally agreed protocol). (If no, suggest they seek help from family or friends) Were you prescribed pain killers upon discharge? Yes No - ACTION - send new prescription Yes No Have you got any pain? Are you managing pain adequately with the painkillers provided? Yes No Vascular network operational policy December 2014 V1 AH/JB Page 40 Are you clear about the medication you should be taking? Yes No (i.e. statins) Vascular network operational policy December 2014 V1 AH/JB Page 41 Record patient name & ID if photocopying page: Are you clear about what happened during your operation? Yes No (i.e. any complications and how long it should take you to recover) Yes No Is your wound healing satisfactorily? Do you have any stitches or clips still in place? Telepho ne followup Are you aware of when your next follow-up appointment is? Did you get written information given to you before or after your operation? Is your wound dry? Yes No Is there any surrounding redness or discharge? No Yes – ACTION – book early follow-up appointment No Yes – have you a date for having them removed by the District Nurse (usually 10 – 14 days)? No – ACTION – follow this up Yes - / / Yes No – ACTION – check & let patient know Yes No – ACTION – send leaflet Are there any concerns I can help you with today? Actions required () Re-send prescription Pain killer Statin Re-send patient information leaflet Ensure patient has District Nurse appointment & inform them Book for early follow-up appointment Book for standard follow-up appointment Telephone GP Contact Consultant Surgeon Vascular network operational policy December 2014 V1 AH/JB Required Completed Page 42 Notes: Vascular network operational policy December 2014 V1 AH/JB Page 43 Appendix 7 Vascular surgeons, anaesthetists and hybrid theatre timetable Vascular network operational policy December 2014 V1 AH/JB Page 44 AM PM AM PM AM PM AM PM AM PM Backhouse Choksy Choksy Choksy Abu‐Own Abu‐Own Assar Assar Backhouse Choksy Hybrid Theatre Bagwat Bagwat Malaj Malaj TBC TBC Patient Patient McKenzie McKenzie AM PM AM PM AM PM AM PM AM PM Osman Osman Abu‐Own Abu‐Own Choksy Choksy Backhouse Backhouse Howard Howard Driver Driver Malaj Malaj TBC TBC Patient Patient McKenzie McKenzie AM PM AM PM AM PM AM PM AM PM Abu‐Own Abu‐Own Choksy Choksy Backhouse Backhouse Assar Assar Howard Howard Bagwat Bagwat Malaj Malaj TBC TBC Patient Patient McKenzie McKenzie AM PM AM PM AM PM AM PM AM PM Osman Osman Choksy Abu‐Own Howard Howard Backhouse Backhouse Howard Howard Driver Driver Malaj Malaj TBC TBC Patient Patient McKenzie McKenzie AM PM AM PM AM PM AM PM AM PM Backhouse Abu‐Own Choksy Choksy Osman Osman Assar Assar Howard Howard Bagwat Bagwat Malaj Malaj TBC TBC Patient Patient McKenzie McKenzie AM PM AM PM AM PM AM PM AM PM Osman Osman Choksy Abu‐Own Assar Assar Backhouse Backhouse Howard Howard Driver Driver Malaj Malaj TBC TBC Patient Patient McKenzie WEEK 1 Monday Tuesday Wednesday Thursday Friday WEEK 2 Monday Tuesday Wednesday Thursday Friday WEEK 3 Monday Tuesday Wednesday Thursday Friday WEEK 4 Monday Tuesday Wednesday Thursday Friday WEEK 5 Monday Tuesday Wednesday Thursday Friday WEEK 6 Monday Tuesday Wednesday Thursday Friday Vascular network operational policy December 2014 V1 AH/JB Page 45 Vascular network operational policy December 2014 V1 AH/JB Page 46 Vascular network operational policy December 2014 V1 AH/JB Page 47