Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Neuropsychopharmacology wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Orphan drug wikipedia , lookup
Pharmaceutical marketing wikipedia , lookup
Compounding wikipedia , lookup
Pharmacognosy wikipedia , lookup
Theralizumab wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Neuropharmacology wikipedia , lookup
Drug interaction wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Drug design wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
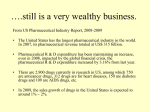
Expert Opinion on Drug Discovery ISSN: 1746-0441 (Print) 1746-045X (Online) Journal homepage: http://www.tandfonline.com/loi/iedc20 Open Access Could Transform Drug Discovery: A Case Study of JQ1 Zeeshaan Arshad, James Smith, Mackenna Roberts, Wen Hwa Lee, Ben Davies, Kim Bure, Georg A. Hollander, Sue Dopson, Chas Bountra & David Brindley To cite this article: Zeeshaan Arshad, James Smith, Mackenna Roberts, Wen Hwa Lee, Ben Davies, Kim Bure, Georg A. Hollander, Sue Dopson, Chas Bountra & David Brindley (2016) Open Access Could Transform Drug Discovery: A Case Study of JQ1, Expert Opinion on Drug Discovery, 11:3, 321-332, DOI: 10.1517/17460441.2016.1144587 To link to this article: http://dx.doi.org/10.1517/17460441.2016.1144587 Accepted author version posted online: 21 Jan 2016. Published online: 16 Feb 2016. Submit your article to this journal Article views: 219 View related articles View Crossmark data Full Terms & Conditions of access and use can be found at http://www.tandfonline.com/action/journalInformation?journalCode=iedc20 Download by: [University of Southern Indiana] Date: 29 April 2016, At: 09:42 EXPERT OPINION ON DRUG DISCOVERY, 2016 VOL. 11, NO. 3, 321–332 http://dx.doi.org/10.1517/17460441.2016.1144587 REVIEW Open Access Could Transform Drug Discovery: A Case Study of JQ1 Zeeshaan Arshada,b, James Smithc,d, Mackenna Robertsd, Wen Hwa Leea, Ben Daviesc,d, Kim Buree, Georg A. Hollanderf,g, Sue Dopsonh, Chas Bountraa* and David Brindleyc,d,h,i,j,k* Downloaded by [University of Southern Indiana] at 09:42 29 April 2016 a Structural Genomics Consortium, Nuffield Department of Medicine, University of Oxford, Oxford, UK; bSchool of Medicine, University of St. Andrews, St. Andrews, UK; cNuffield Department of Orthopedics, Rheumatology and Musculoskeletal Sciences, University of Oxford, Oxford, UK; dThe Oxford – UCL Centre for the Advancement of Sustainable Medical Innovation (CASMI), The University of Oxford, Oxford, UK; e Sartorius Stedim, Göttingen, Germany; fDepartment of Biomedicine, University of Basel, and Basel University Children’s Hospital, Basel, Switzerland; gDepartment of Pediatrics, University of Oxford, Oxford, United Kingdom; hSaid Business School, University of Oxford, Oxford, UK; iCentre for Behavioral Medicine, UCL School of Pharmacy, University College London, London, UK; jHarvard Stem Cell Institute, Cambridge, MA, USA; kUSCF-Stanford Center of Excellence in Regulatory Science and Innovation (CERSI), San Fransisco, CA, USA ABSTRACT ARTICLE HISTORY Introduction: The cost to develop a new drug from target discovery to market is a staggering $1.8 billion, largely due to the very high attrition rate of drug candidates and the lengthy transition times during development. Open access is an emerging model of open innovation that places no restriction on the use of information and has the potential to accelerate the development of new drugs. Areas Covered: To date, no quantitative assessment has yet taken place to determine the effects and viability of open access on the process of drug translation. This need is addressed within this study. The literature and intellectual property landscapes of the drug candidate JQ1, which was made available on an open access basis when discovered, and conventionally developed equivalents that were not are compared using the Web of Science and Thomson Innovation software, respectively. Expert opinion: Results demonstrate that openly sharing the JQ1 molecule led to a greater uptake by a wider and more multi-disciplinary research community. A comparative analysis of the patent landscapes for each candidate also found that the broader scientific diaspora of the publically released JQ1 data enhanced innovation, evidenced by a greater number of downstream patents filed in relation to JQ1. The authors’ findings counter the notion that open access drug discovery would leak commercial intellectual property. On the contrary, JQ1 serves as a test case to evidence that open access drug discovery can be an economic model that potentially improves efficiency and cost of drug discovery and its subsequent commercialization. Received 19 October 2015 Accepted 18 January 2016 Published online 15 February 2016 1. The need for open access in therapeutic development The process of translation as it currently stands is fundamentally flawed.[1–5] Despite recent advances in our scientific understanding of disease pathology coupled with dramatic technological breakthroughs in patient care, companies have produced relatively few novel drugs as genuine new treatments for existing diseases.[6] With high attrition rates and soaring costs for clinical trials, translational science budgets to investigate novel drugs as opposed to existing and alternative treatments are dwindling. This is partly due to the current restrictive economic climate, which currently hovers at a mere 3.5% of total basic research and clinical development spending.[7] It is clear that industry needs to develop new, sustainable models for drug discovery to adapt.[8,9] CONTACT David Brindley *Joint senior authors © 2016 Taylor & Francis [email protected] KEYWORDS Open Innovation; Open Access; Drug Discovery; Healthcare Translation; JQ1; Bromodomain; Epigenetics; SGC (Structural Genomics Consortium) The average number of new molecular entities (NMEs) approved each year has remained static at 22.7 per year between 2002 and 2010,[10] despite the overall research and development budget doubling within the same period.[7] Current estimates suggest the cost of developing a drug to be a staggering $1.8 billion,[11] having increased at an annual rate of 13.4% per annum since the 1950s.[12] There has been a period of extensive merger and acquisition (M&A) activity in recent decades [13] in an attempt to reduce expenditure and contain risks associated with drug development. Meanwhile, the number of new drugs approved has still stagnated.[7] The patent expiry of blockbuster drugs, the so-called ‘patent cliff’, for many leading pharmaceutical giants in the early twenty-first century led to an estimated $113 billion in losses across the industry. [14] Although disputed by some authors [15], the loss in 322 Z. ARSHAD ET AL. Article highlights ● ● ● Downloaded by [University of Southern Indiana] at 09:42 29 April 2016 ● ● The process of translation within drug discovery is currently too costly and inefficient leading to a poor output of new drugs for patients as well as less than optimal return on investment for stakeholders especially in key therapeutic areas such as oncology. Open access is an emerging model of OI with the potential to be an economically viable model that could be used by drug developers. To investigate the effects open access can have on drug development the literature and intellectual property landscapes of open access drug candidate JQ1 was compared to conventionally equivalents: PRI 725 and MK 1775. Our results found that openly sharing the JQ1 molecule led to a greater uptake by a wider and more multidisciplinary research community contributing to greater and more impactful research into the molecule itself as well as its therapeutic target. This has potential to improve understanding regarding the drugs full repertoire of effects and uses within the body leading to improved translation times and reduced attrition rates within clinical trials. Contrary to popular belief, the initial free availability of the JQ1 molecule actually led to greater downstream patenting. This offers clear evidence that open access is a commercially viable model of drug discovery that has the potential to lead to improved commercial gain for drug developers. This box summarizes key points contained in the article. these revenues also contributes to the soaring costs of drug development.[16] In addition, our increasing understanding of disease has led to a desire to treat diseases of a greater complexity and specificity, with costly technology, such as monoclonal antibodies.[17] These approaches often target diseases with low incidence and, therefore, may lead to lower reimbursement, potentially deterring industry investment in these areas.[6] While on average it takes 10–15 years to progress a drug from target discovery to market,[11] many drug candidates can take as long as 30 years to develop from bench to first-in-man clinical trials.[18] Increasing regulation complicating trial design and authorization requirements are a significant factor. [19,20] Many argue that burdensome regulations are unnecessarily delaying drug translation: the time required by an organization to gather data and submit a new drug application (NDA) increased from 3 to 7 years between 1962 and 1989.[21] Lengthening timescales on returns may also dampen investors’ appetite to provide badly needed funding. By contrast, it is imperative to ensure that patient safety is tantamount to prevent incidences, such as the thalidomide tragedy in the mid-twentieth century [22], which resulted in new regulations and, notably, the Kefauver Harris Amendment requiring a drug’s safety and efficacy be proven before authorized.[23] A balance must be achieved that preserves patient safety while retaining reasonable efficiency in translation so that patients equally may benefit from therapeutic progress and the translation process does not become unsustainable.[7] Compounding these problems is the high attrition rates of new drug candidates.[24] On average, only 11% of drugs reaching phase I clinical trials gain regulatory approval,[25] while phase II trials have also have a staggering 25% attrition rate.[26] More bleakly, only one in 24 newly investigated NME’s reach market.[26] The consequential, significant loss to the industry in terms of capital, other resources and manpower are detrimental. Among the factors responsible, is a lack of scientific understanding of disease pathology, drug targets, toxicity and/or mechanism of action for treatment efficacy.[27,28] Beyond the science, however, there are factors that relate to the current precompetitive model for drug discovery in the pharmaceutical industry, which conducts unreported research behind closed doors engendering secrecy while molecular structures are patented. Multiple corporations, therefore, inadvertently often duplicate chemical compound investigations on the same molecule, thereby wasting money and resources when the majority will fail and could have been prevented if results shared.[29] Industry as well as academic centers justify this superfluous waste and duplication by the potential it may discover valuable competitive know-how and patentable drugs notwithstanding the high attrition rates. An example of this is the massive losses industry faced while trying to develop an NK1 receptor antagonist to treat pain.[29] If the industry had worked together, this problem could potentially have been noticed earlier – preventing any further wastage of time and effort. Attrition rates vary meaningfully by therapeutic area: cardiovascular drug candidates have a 20% success rate compared to 8% [25] in neurodegenerative disease. This variation suggests different models such as translation including open access, which may be better suited to certain research fields than others.[30] The discovery of novel drug treatments of neurodegenerative diseases such as Alzheimer’s, therefore, is potentially a ripe area for open access drug discovery to share research efforts and avoid duplication.[31] There are currently five approved drugs to treat Alzheimer’s disease, which function only to slow down progression.[32] Despite extensive efforts, with a heavy focus on amyloid plaques as a target, no new drug has been brought to market since the approval of memantine, an N-methyl-D-aspartate receptor antagonist, in 2003.[33] With one of the worst attrition rates in any therapeutic area at 0.4% during the period 2002– EXPERT OPINION ON DRUG DISCOVERY 323 Possible Indications Closed Model Secrecy = long lag before community takes interest Serendipity= uncoordinated accumulation of knowledge • • • • Knowledge accumulation is linear, repetitive & slow Longer to de-risk drug candidate Limited access to global academia Small, non-pooled funds Closed Healthcare Translation Downloaded by [University of Southern Indiana] at 09:42 29 April 2016 Possible Indications Open Open Probes = faster adoption and de-risking/ narrowing of indication Each square represents an arbitrary amount of effort/resources spent on validating a new target for different indications Open Model Target Validation • • • • Open access & freedom to operate ensures much quicker adoption of drug candidate Knowledge accumulation is exponential, less repetitive and fast Unlimited access to global academics Larger pooled funds Figure 1. Comparing the closed (upper half) model to the open (lower half) model: the free availability of open access tools in drug discovery allows the research community to explore the drug candidate in multiple models of disease and report back through publication. The increased research in the open model can lead to improved understanding of drug candidate and target and thus lower attrition rates in clinical trials while allowing drug developers to focus on the most promising indications, whilst reducing the level of effort (open squares), wastage, and duplication present to a greater extent in the closed model (adapted from Lee WH (2015) Open Access Target Validation Is a More Efficient Way to Accelerate Drug Discovery. Permission granted for use. 2012 [34], there is a dire need to come up with a solution to this age-related disorder in the context of the current ageing population.[35] To develop a solution to this and other devastating diseases, the pharmaceutical industry, and in particular the process of translation, needs to become more efficient. Although there is no definite remedy, open access is an option that offers a promising alternative to traditional models of drug development.[36,37] This study investigates the impact of this model by comparison through literature and patent landscape analysis to compare the development of JQ1, a drug developed with no IP (Intellectual Property) restrictions until validated and conventionally developed equivalents. 2. Quantitative and qualitative assessment of open access in drug development 2.1. Research and development stage – academic impact Open innovation (OI) is a multifaceted concept [38] that is difficult to define because it represents a continuum of states from completely closed systems at one end and open access at the other.[39] Organizations utilize the concept to different degrees by varying the permeability of the boundaries [36] where ideas and resources can be exchanged.[38] Pharmaceutical companies such as AstraZeneca have adopted OI methods through the ‘licensing in and out’ of resources to reduce risk and share reward.[40] Open access is a narrow and more precise aspect of OI. Its distinguishing feature is that it involves no restriction on the use of information in the public open domain, meaning no fee, licenses, or conditions for use or access to information (see Figure 1). Organizations such as the Structural Genomics Consortium (SGC, University of Oxford, U.K.) and the Single Nucleotide Polymorphisms Consortium (National Institute of Health, Bethesda, MD, U.S.A.) have taken this OI concept of licensing technology platforms further to more controversially adopt a fully open access drug discovery model. JQ1, a BRD4 inhibitor, is an example of a drug candidate that was developed through open access methods. The target BRD4 was initially explored through the open access work between the SGC and GlaxoSmithKline (GSK, Brentford, U.K.) in 2009. Just 11 months later this led to the discovery of JQ1 and its investigation to treat the rare cancer NUT midline carcinoma [41] at the Dana Farber Cancer Institute, where it was then made publically available. It is currently in phase I/II clinical trials as well as investigation for the treatment of several other malignancies. To investigate the impact that open access can have on the process of drug translation, the development of JQ1, since it was discovered and made publically available, was compared to two conventional drug discovery candidates: PRI 724 and MK 1775 (control drugs Downloaded by [University of Southern Indiana] at 09:42 29 April 2016 324 Z. ARSHAD ET AL. candidates) that were never made available to the public domain. The control drug candidates were selected via the following criteria that they must be: (i) first-inclass, (ii) used to treat cancer in the first instance, and (iii) small molecules (<600 molecular weight). The initial development of all drugs were compared, this time being the point of target discovery to drug discovery, to ensure similarity in terms of transition times up until JQ1 was discovered and made available on an open access basis to highlight differences from the point that JQ1 was made publically available. Two metrics were employed to evaluate and compare the research and development (R&D) stages of translation for each drug molecule: the literature landscapes, and the intellectual property patent landscapes. To further compare the impact of an open access drug discovery model with OI licensing models adopted by pharmaceutical companies, the open access JQ1 probe and the control drug candidates were then compared to selumetinib, which is currently being developed in AstraZeneca’s (London, U.K.) OI pipeline. Before going onto discussion, here we present a short overview of the controls and selumetinib: PRI-724, a beta- catenin inhibitor in the wnt-signaling pathway was originally implicated in colon cancer in 2004. It is currently in phase I/II clinical trials being investigated in colonic cancer, pancreatic cancer, hepatitis C induced liver cirrhosis as well as a range of hematological malignancies. MK-1775 is a WEE1 inhibitor and was implicated in cancer in 2009 when it was discovered that it would prevent cancer cells making it across the G1/S cell cycle checkpoint, and therefore, should be investigated as a potential cancer treatment. It is currently in phase I/II clinical trials involving a range of cancers including acute myeloid leukemia (AML), chronic myeloid leukemia (CML), gynecological, and gastrointestinal tract malignancies. Selumetinib, a MEK inhibitor, is a part of AstraZeneca’s OI pipeline and earlier this year received orphan drug approval for the treatment of uveal melanoma – a rare intraocular cancer affecting various tissues in the eye. The drug is also being investigated in clinical trials for thyroid cancer, KRAS mutation positive lung cancer, and neurofibromatosis type 1. Note for all drug candidates, the date they were discovered is not known (apart from JQ1) and as such the date of first publication regarding each drug candidate was taken as T0 to allow fair comparison between them. The first papers regarding the drug candidates in a therapeutic context, and their citation metrics, were identified using Web of Science software (Thomson Reuters, New York, NY, U.S.A.) (see Table 1 for an overview of the search). A brief overview of the search methodology and analysis is as follows. The first publication for each drug candidate was identified using the Web of Science Software. The search was then narrowed to include articles published within 4 years from but not including the first publication year for each drug candidate. The results were then manually reviewed to confirm the relevance of search results and to remove any duplicates. The cleaned results were broken down by year, author, source title, and research area for analysis. The search only included authors that had more than two publications as the search criteria had to be narrowed to allow the software to compute the results for JQ1. It should be noted that one paper was removed as it was deemed irrelevant in relation to JQ1 and one duplicate author was also removed for JQ1. It is clear that, even when not accounting for the number of years since publication, the paper regarding JQ1 has a greater number of citations compared to the controls, suggesting that open access can increase Table 1. An overview of citation and publication analysis for each drug candidate that was carried out using Web of Science. Drug JQ1 Search terms ‘JQ1’ OR ‘SGCBD01’ ‘PRI-724’ OR ‘PRI724’ OR ‘PRI 724’ OR ‘ICG-001’ OR ‘ICG001’ OR ‘ICG 001’ MK-1775 ‘MK-1775’ OR ‘MK1775’ OR ‘MK 1775’ OR ‘AZD-1775’ OR ‘AZD 1775’ OR ‘AZD1775’ Selumetanib ‘Selumetinib’ OR ‘AZD6244’ OR ‘AZD-6244’ OR ‘AZD 6244’ OR ‘AZD6244’ OR ‘AZD-6244’ OR ‘AZD 6244’ OR ‘ARRY142886’ OR ‘ARRY-142886’ OR ‘ARRY 142886’ PRI-724 First paper Selective inhibition of BET bromodomains A small molecule inhibitor of catenin/ CREB- binding protein transcription Discovery of gene expression -based pharmacodynamic biomarker for a p53 context-specific anti-tumor drug Wee1 inhibitor Targeted agents for the treatment of advanced renal cell carcinoma Year of first publication/years analyzed Citing articles within years required Published articles within years required 2010/ 2011–2014 294 98 2004/ 2005–2008 29 5 2009/ 2010–2013 14 25 2005/ 2006–2009 18 48 EXPERT OPINION ON DRUG DISCOVERY 160 a.) JQ1 140 350 325 b.) 300 250 PRI-724 200 Selumetinib Number of Authors 60 Selumetinib 20 PRI-724 JQ1 PRI-724 JQ1 PRI-724 d.) JQ1 Number of Citations Number of Publications 30 Number of Journals 1200 JQ1 40 Number of Research Areas 1400 c.) 50 Number of Countries Selumetinib 4 MK-1775 3 Selumetinib 2 Number of Years After First Publication MK-1775 1 Selumetinib 0 0 JQ1 50 20 JQ1 100 40 MK-1775 150 60 PRI-724 80 Selumetinib 100 MK-1775 Number of Citations MK-1775 120 1000 800 600 400 Selumetinib MK-1775 Downloaded by [University of Southern Indiana] at 09:42 29 April 2016 10 200 MK-1775 PRI-724 PRI-724 0 0 1 2 3 4 Number of Years After First Publication 1 2 3 4 Number of Years After First Publication Figure 2. a.) Figure presents the number of citations first papers regarding each drug candidate in a therapeutic context gained in the four years after publication b.) Figure presents the first papers regarding the drug candidates in a therapeutic context, and their citation metrics, in the four years after publication c.) The figure represents the number of articles published with the said drug candidate as a key word in the four years after its discovery d.) The figure represents the number of citations articles published with the said drug candidate as a key word gained, in the four years after their discovery. T0 was taken as the beginning of the next whole year after publication. Figure was created using the Web of Science Software. dissemination and awareness of a drug candidate’s discovery. The results were then limited to the number of citations each paper received within 4 years following initial publication reporting discovery (Figure 2a). The mean increase in the number of citations for the paper regarding JQ1 was 73.5 per year compared to the control average of 5.4 per year, suggesting that open access leads to an increased rate of acknowledgment of drug candidate discovery. Selumetenib did not fare better either suggesting OI is not as effective an oncology drug discovery model, in this respect, as open access. Further, open access may lead to wider, more multidisciplinary community acknowledgment of drug candidate discovery, as citations of JQ1 were from a greater number of countries, research areas, and by a greater number of authors in a broader range of journals (Figure 2b). This broader diaspora of knowledge into the research community brought by open access methodology has the potential to spark intellectual discussion and experimentation into novel drug candidates. Lack of innovation, after all, can be seen as another contributing factor to the pharmaceutical industry’s recent decline [42], and as such drawing on a broader range of skills and a greater variety of innovative minds to investigate drug candidates could meaningfully improve drug innovation. JQ1 appears to have improved innovation (Figure 2c and d). Based on the number of articles published naming the drug candidates in the 4 years after its discovery, open access seems to have catalyzed further research into the application of JQ1 by comparison to the controls. Although, selumetinib stimulated later research more than the controls, JQ1 still outstripped selumetinib. This is one of the factors that highlight the success of the R&D stage of the development of JQ1. JQ1 is not the only a drug candidate that has evolved from open access models of innovation. The Biomarkers Consortium (Foundation of the National Health Institute, Bethesda, MD U.S.A.) is a public–private research partnership. It aims to develop and gain approval for biomarkers in the hope of developing new drugs and diagnostic test paving the path for personalized medicine by making their work available on an open access basis. Similar motivations can be seen in other open access organizations such as the SGC that was set up in 2004 as a not for profit organization to determine the structures of proteins of medical interest, and then make the work available on an open access basis with a priority being benefit to society rather than capital or personal gain. One of the SGC’s main focuses has been epigenetics, in particular areas that are under-studied. In addition, in this respect, the findings have been ground breaking: 326 Z. ARSHAD ET AL. 40 Average Number of Citations per Article BRD4 (JQ1) 35 beta-catenin (PRI724) 30 WEE1 (MK-1775) 25 MEK1/2 (Selumetinib) 20 JMJD3 15 10 5 0 0 1 2 3 4 5 Downloaded by [University of Southern Indiana] at 09:42 29 April 2016 Year After First Publication Figure 3. This figure shows data collected showing the number of citations per article published regarding each drug candidate’s therapeutic target in the four years after each candidate’s discovery. Data was collected using the Web of Science software. The SGC open access target JMJD3, while still in the very early stages of development, shows promising potential. determining the structure of the ZMPSTE24, a nuclear zinc metalloprotease involved in progeria [43] as well as the discovery of the target JMJD3, a histone demethylase.[44] The small molecule GSK J1, has been shown to inhibit JMJD3 and, thus stops the production of cytokines such as tumor necrosis factor that are associated with the inflammatory response, and as a result been implicated in inflammatory disorders such as rheumatoid arthritis.[44] This has been possible through the open access work of the SGC and its partners: GlaxoSmithKline and Cellzome, in this instance. This success story behind open access highlights another important part of how it has potential to improve R&D though improved target validation. GSK J1 and JQ1 have led to more impactful research into their therapeutic targets (Figure 3 and Table 2 present an overview of the search with the methodology and analysis being the same as discussed previously). It should be noted that selumetinib did not fare better than the drugs developed via conventional drug development strategies in this respect. A better understating of a drug candidates therapeutic target is imperative to understanding its mechanism of action and how it may behave in the human body in terms of efficacy and toxicity. This understanding is often lacking within the pharmaceutical industry as illustrated by the fact that only 7% of approved small molecular drugs have a known target.[27] The effects of a thorough understanding of a therapeutic target during drug development can be exemplified by the success of Gleevec (Novartis, Basel, Switzerland), a first-in-class treatment for chronic myeloid leukemia that was approved by the Federal Drug Table 2. An overview of citation and publication analysis for each drug candidate therapeutic target that was carried out using Web of Science. Search term ‘BRD4’ OR ‘Bromodomain 4’ OR ‘Bromodomain Four’ ‘Beta-catenin’ OR ‘β-catenin’ WEE1 ‘MEK1’ OR ‘MAPKK1’ OR ‘MKK1’ OR ‘PRKMK1’ OR ‘ERK activator kinase 1’ OR ‘MAP kinase kinase 1’ OR ‘MAPK/ERK kinase 1’ OR ‘mitogenactivated protein kinase kinase 1’ OR ‘ME K2’ OR ‘MAPKK2’ OR ‘MKK2’ OR ‘PRKMK2’ OR ‘ERK activator kinase 2’ OR ‘MAP kinase kinase 2’ OR ‘MAPK/ERK kinase 2’ OR ‘mitogen-activated protein kinase kinase 2’ JMJD3 Drug JQ1 Target BRD4 PRI-724 Beta-catenin MK-1775 WEE1 Selumetanib MEK1/2 GSKJ1 JMJD3 Publications within years required 289 8970 242 1263 117 Association (FDA) in 2001.[45] Unlike other cancer therapies, the effects of Gleevec are highly specific to leukemic cancer cells that display the typical cytological genetic mutation, the Philadelphia chromosome, present in 95% of those who suffer from the once fatal CML. The drug targets the fusion protein bcr–abl, a tyrosine kinase, created as a result of reciprocal translocation of chromosomes 9 and 22.[46] This high specificity was achieved through the advent of rational drug design [47] in which, once a good understanding of the therapeutic target is achieved, a systematic approach is taken to identify an inhibitor.[45] The drug has also EXPERT OPINION ON DRUG DISCOVERY 327 Table 3. An overview of patent search that was carried out using Thomson Innovation Software. Downloaded by [University of Southern Indiana] at 09:42 29 April 2016 Drug Broad target Dates searched Search terms CTB = (bromodomain* OR BRD1 OR BRD2 OR BRD3 OR BRD4 OR BRD5 OR BRD6 OR BRD7 OR BRD8 OR BRD9 OR BRDT OR JQ1 OR extra terminal OR (extra NEAR2 terminal) OR extrac OR (extra adj c)) NOT DC = (C OR S OR T OR U OR V OR W OR X) and AD ≥ (20110101) and AD ≤ (20150615); CTB = ((wnt NEAR5 pathway NEAR5 inhibitor) OR (wnt NEAR5 modulator) OR ICG001 OR (ICG adj 001) OR (canonical NEAR5 wnt) OR (CBP NEAR5 catenin) OR ((β adj catenin) NEAR5 (inhibitor OR antagonist)) OR ((beta adj catenin) NEAR5 (inhibitor OR antagonist)) OR ((wnt NEAR5 pathway) NEAR5 (inhibitor OR antagonist)) OR (beta adj catenin NEAR5 signal*) OR (wnt NEAR5 (inhibitor OR antagonist)) OR (wnt NEAR5 signaling NEAR5 inhibitor)) not DC = (C OR S OR T OR U OR V OR W OR X) and AD ≥ (20050101) and AD ≤ (20090615); CTB = (wee1 OR (wee adj 1) OR wee2 OR (wee adj 2) OR (wee adj like adj protein*) OR (wee1 adj (kinase* OR tyrosine* OR inhibitor*)) OR MK1775 OR (MK adj 1775) OR (checkpoint adj kinase*)) NOT DC = (C OR S OR T OR U OR V OR W OR X) AND AD≥(20100101) AND AD ≤ (20140615); JQ1 Bromodomain 01/01/2011–15/06/2015 PRI-724 WNT pathway 01/01/2005–15/06/2009 MK-1775 Checkpoint kinase 01/01/2010–15/06/2014 been approved for treating gastrointestinal tract stromal tumors [48] and many say has paved the way to other targeted cancer therapies such as Herceptin (Genentech Inc., San Francisco, CA, U.S.A.) and Gefitinib (AstraZeneca; London, U.K.). Gleevec’s success, as further illustrated by the fact that the drug gained approval within just 3 years of entering clinical trials, [47] can, at least in part, be attributed to good understanding of the drug’s target. This understanding, however, took years to build with the discovery of the Philadelphia chromosome occurring decades before the advent of Gleevec. Open access offers a possible path to achieve better target understanding at a more rapid rate by catalyzing research, without the wasteful costs of duplicative work among industry. 2.2. Product discovery stage – intellectual property Intellectual property is a key concern in models of OI. [49] In many respects, IP is necessary to allow organizations to benefit financially from inventions and thus spur R&D into new products that can benefit society as a whole, while creating capital for organizations to further innovate.[50] This is especially true within the pharmaceutical industry. With multibillion dollar investments in molecules that can easily be recreated by competitors, investors require proof of protection of their assets. It is therefore natural to assume that open access may jeopardize this, as it is a widely held belief that an exclusivity period is required for an organization to profit from a new drug.[51] Initial number of DWPI families Final number of DWPI families 241 222 149 125 144 125 To investigate the impact that open access can have on intellectual property practices, the IP landscapes of both control targets and bromododomains were compared. In respect of bromodomains, these patents refer to the patents filed after JQ1 was discovered and made available on an open access basis in relation to its therapeutic target. Patent families were harvested regarding the broad target of each drug using Thomson Innovation software (Thomson Reuters, New York, NY, U.S.A.) in the four and half years after their respective discoveries (Table 3 presents an overview of the search). The search includes both granted patents and published patent applications. Keyword searches were performed of a patent’s title, abstract and claims sections across a complete global dataset of 50 patent authorities. The search time period was restricted to 4.5 years from the year of discovery, as determined by the year of first publication. Table 3 lists the patent search results collapsed by Derwent World Patents Index (DWPI) families, meaning one invention per family of member patents. This enables a clearer assessment of the number of inventions that has resulted since discovery of the drug molecule rather than the total number of patent publications that has resulted, which does not account for duplication when the same invention is patented in multiple jurisdictions. All initial collections of search results were cleaned by manual review and irrelevant patent documents were removed. The initial open access availability of JQ1 positively impacted the number of patents filed regarding Z. ARSHAD ET AL. inventions involving bromodomains (Figure 4a). Although the number of patents filed in the first year after creation is similar for both JQ1 and controls, by the fourth year a difference is apparent, with 105 patents regarding bromodomains and a mean of just 29 for MK 1775 and PRI 724 – highlighting the effect that open access can have on downstream patenting. Although concerns regarding open access and IP are understandable, JQ1 is premise against this issue as the availability of the drug has catalyzed the generation of new inventions, while retaining the inventors’ rights to benefit from them. Since patents hold value in themselves it could be concluded that open access has the potential to create commercial value: increasing a company’s worth, while also encouraging investment. Similar phenomena have occurred in other fields [52] such as the software industry. Initially, the industry thought that the value was in the hardware and then software. However, when the computer-programming licenses were opened to users, it actually encouraged more innovation and better quality programming. This was eventually more lucrative to the industry than if it had clung to protecting proprietary ownership.[36] The patterns highlighted in the R&D stage of JQ1’s development seem to be reiterated in the product discovery stage (Figure 4b). The wider diaspora of knowledge created in the R&D stage of development has continued along the process of translation, leading to greater patent diversity in the product discovery stage. This is testament to the fact that open access has the potential to spark innovation. Greater patent diversity 100 3. Conclusion In conclusion, the output of new drugs by pharmaceutical companies has been declining. Open access is an emerging model of OI with the potential to be an economically viable model that could be used by drug developers to help combat this problem. To investigate the effects, open access can have on drug development 100 a.) b.) 90 Bromodomain (JQ1) 80 60 40 in terms of inventors and assignees can be seen as a positive: preventing a single organization from dominating the market and encouraging other, often-smaller, organizations, to get a piece of the action. On the other hand, it could also lead to patent thickets that hinder development [53], although this does not yet seem to be the case. Comparing the maps (Figure 5) for all three drugs, the field of bromodomains has had patents filed in a broader range of therapeutic areas – ranging from male contraception to kidney disease as well as a range of different cancers. The themescape maps for both controls also have white peaks in certain therapeutic indications highlighting areas of high patent activity. This is in contrast to the map concerning bromodomains, indicating that patent activity is not occurring in a single area and as such, lowering the chances of patent thickets forming. This will allow the greater number of patent holders (Figure 4b.) to take their ideas in different directions without having to navigate each other’s patents – offering clear potential for more capital gain as well as patient benefit. WNT Pathway (PRI724) Number of Patent Families 120 Number of Patent Families 80 70 60 50 40 30 20 10 Countries Inventors WNT Pathway Checkpoint Kinase Bromodomain WNT Pathway Checkpoint Kinase 1 2 3 4 Number of Years After First Publication Bromodomain 0 WNT Pathway Checkpoint Kinase (MK-1775) Checkpoint Kinase 0 20 Bromodomain Downloaded by [University of Southern Indiana] at 09:42 29 April 2016 328 Assignees Figure 4. a.) Figure represents the number of patent families regarding each broad drug target in the four years after each drug candidate discovery. Patent families were harvested using the Thomson Innovation software using key search terms for each target. T0 was taken to be the date of first publication regarding the drug candidates. Datasets were manually sorted to exclude irrelevant patent families based on the title, abstract and claims of each patent document. b.) This figure shows number of countries patents have been filed in as well as the number of assignees and inventors of those patents for each drug class. The figure was produced using the Thomson Innovation software. Downloaded by [University of Southern Indiana] at 09:42 29 April 2016 EXPERT OPINION ON DRUG DISCOVERY 329 Figure 5. Figure 5 is map representing the different therapeutic areas patents have been filed under for each respective drug class. It aims to give a very broad overview of the therapeutic areas each drug target is implicated in, and can assist in visualizing clusters of patents in particular therapeutic areas. Thomson Innovation software was used to search through the uses section of each patent document and cluster therapeutic areas together that came up often. Each dot represents a patent and the contours proportionally represent the degree of patent activity. this study compared the literature and intellectual property landscapes of open access drug candidate JQ1 and conventionally developed equivalents: PRI 725 and MK 1775. Our results found that openly sharing the JQ1 molecule led to a greater uptake by a wider and more multidisciplinary research community contributing to greater and more impactful research into the molecule itself as well as its therapeutic target. This has potential to improve understanding regarding the drugs full repertoire of effects and uses within the body leading to improved translation times and reduced attrition rates within clinical trials. This improved R&D accelerated innovation, evidenced by the broader range of therapeutic areas patents were filed in regarding JQ1 and its target. More interestingly, our study found that contrary to popular belief, the initial free availability of the JQ1 molecule actually led to greater downstream patenting something that offers clear evidence that open access is a commercially viable model of drug discovery that has the potential to lead to improved commercial gain for drug developers in the long run. 4. Expert opinion It is apparent that certain therapeutic areas such as neurodegenerative disease are facing a critical lack of innovation in current drug development models. Open access, although in its infancy, offers a promising approach to tackle the problems facing drug developers in these areas. Although OI in industry improves aspects of translation, as exemplified by AstraZeneca’s OI candidate selumetinib, the benefits appear to be reduced in comparison to open access. Improved R & D leading to a greater understanding of therapeutic target has potential, as exemplified by the success story of Gleevec, to lead to shorter transition times in the later stages of translation. Increased understanding regarding drug candidate through more widespread and impactful research has also the potential to reduce attrition rates. Although open access may lead to greater innovation and therefore potential drug candidates, hopefully by sharing knowledge the ones that do not have potential to reach market will be weeded out as early as possible, even as early as the preclinical stages of development. In addition, it has been argued that making early stage drug research available to others, may spur additional investment and partnership opportunities through avocation of an organizations work.[54] All these have potential to reduce the exuberant costs associated with drug development: the benefits of which will be felt by all stakeholders in the pharmaceutical industry. IP practices are considered essential in allowing inventors to benefit from their discoveries – however over patenting can be a hindrance to drug developers. By Downloaded by [University of Southern Indiana] at 09:42 29 April 2016 330 Z. ARSHAD ET AL. allowing the initial stages of drug development to be carried out in an open access environment everyone can benefit from the availability of information regarding drug candidates during a time of high risk and attrition. The open access environment would allow this high risk to be distributed among different stakeholders all the while facilitating downstream patenting to allow inventors to benefit from their inventions at a later and more commercially viable stage of drug translation. This could in fact lead to greater profit for an industry that has been suffering from declining reimbursement in the past few decades. The success of organizations such as the SGC and the Single Nucleotide Polymorphisms Consortium shows that open access does in fact have power to drive forward drug development and is therefore a concept that should be applied more by the pharmaceutical industry. Although open access is used within the pharmaceutical industry [31], it makes an appearance in less commercially viable areas such as neglected diseases. An example of this is the open source malaria project. It has been estimated that malaria killed 435,000 children under the age of five in Africa in 2010 alone.[55] With growing concern that the most fatal form of the disease caused by the strain Plasmodium Falciparum is growing resistant to current therapies in parts of the world [56], the open source malaria project aims to test promising new compounds in the treatment of malaria [57], and in doing so, improve these molecules’ capabilities so they can be translated into new therapies for suffering patients. The success story of JQ1 suggests that other areas that are more commercially viable may equally benefit from truly opening up early stage candidate validation as well. To summarize, open access offers a promising path to improve translation in drug development. If open access is adopted more widely it offers potential in improving the R&D stage of translation through catalysis of research into drug candidate and target. In addition, there is evidence to suggest that making early stage drug tools available for free initially may ultimately lead to greater commercial gain later on through greater downstream patenting. This could lead to improvement in the number of novel therapies being approved that would benefit not only industry and investors, but also patients in dire need of new therapy. Financial and Competing Interests Disclosure The authors have been funded by the SENS Research Foundation, the Centre for the Advancement of Sustainable Medical Innovation (CASMI) Translational Stem Cell Consortium, the Said Foundation and the Oxford National Institute of Health Research Musculoskeletal Biomedical Research Unit. In particular, Z Arshad is funded by the SENS Research Foundation Scholarship, CASMI Translational Stem Cell Consortium. DA Brindley is a Said Fellow in Healthcare Translation at Said Business School, the University of Oxford, Oxford, UK and Managing Partner at IP Asset Ventures. The content outlined herein represents the individual opinions of the authors and may not necessarily represent the viewpoints of their employers. DA Brindley is a stockholder in Translation Ventures Ltd. (Charlbury, Oxfordshire, UK), a company that amongst other services provides cell therapy biomanufacturing, regulatory, and financial advice to pharmaceutical clients. DA Brindley is subject to the CFA Institute’s Codes, Standards, and Guidelines, and as such, this author must stress that this piece is provided for academic interest only and must not be construed in any way as an investment recommendation. Additionally, at time of publication, DA Brindley and the organizations with which he is affiliated may or may not have agreed and/or pending funding commitments from the organizations named herein. DA Brindley declares funding from the SAID foundation and the National Institute for Health Research, Oxford Musculoskeletal Biomedical Research Unit. B Davies is a Senior Associate at IP Asset Ventures Ltd. K Bure is a Global Director of Regenerative Medicine at Sartorius Stedim Biotech. C Bountra is a Structural Genomics Consortium Oxford Lead Scientist. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed. References Papers of special note have been highlighted as either of interest (•) or of considerable interest (••) to readers. 1. Kessel M. The problems with today’s pharmaceutical business—an outsider’s view. Nat Biotechnol. 2011;29:27–33. • A summary of the challenges faced by drug developers. 2. Staff NP, Runge BK, Windebank AJ. Breaking down translation barriers: investigator’s perspective. Sci Transl Med. 2014;6:252. 3. Scannell JW, Blanckley A, Boldon H, et al. Diagnosing the decline in pharmaceutical R&D efficiency. Nat Rev Drug Discov. 2012;11:191–200. • Reasoning behind the decline in new drug approvals. 4. Rawlins MD. Cutting the cost of drug development? Nat Rev Drug Discov. 2004;3:360–364. 5. Wells JR, Raabe AR. Pharmaceutical industry in 2005: case study. Harv Buisniness Rev. 2005. 6. A review of UK health research funding. London: The stationary Office, 2006. 7. Fernandez J-M, Stein RM, Lo AW. Commercializing biomedical research through securitization techniques. Nat Biotechnol. 2012;30:964–975. 8. Cockburn IM. The changing structure of the pharmaceutical industry. Health Aff. 2004;23:10–22. 9. Hunter J, Stephens S. Is open innovation the way forward for big pharma? Nat Rev Drug Discov. 2010;9:87–88. 10. Novel New Drugs Summary. Silver Spring (MD): FDA; 2015. Downloaded by [University of Southern Indiana] at 09:42 29 April 2016 EXPERT OPINION ON DRUG DISCOVERY 11. Paul SM, Mytelka DS, Dunwiddie CT, et al. How to improve R&D productivity: the pharmaceutical industry’s grand challenge. Nat Rev Drug Discov. 2010; 9:203–214. 12. Munos B. Lessons from 60 years of pharmaceutical innovation. Nat Rev Drug Discov. 2009;8:959–968. 13. LaMattina JL. The impact of mergers on pharmaceutical R&D. Nat Rev Drug Discov. 2011;10:559–560. 14. Evaluate Ltd. EvaluatePharma alpha world preview. Evaluate Pharma. 2014:3. 15. Brindley D, Reeve B, Mason C. Pharmaceutical industry: investors unfazed by drug-patent expiry. Nature. 2012;481:265. 16. Harrison C. Patent watch: the patent cliff steepens. Nat Rev Drug Discov. 2011;10:12–13. 17. Abboud C, Berman E, Cohen A, et al. The price of drugs for chronic myeloid leukemia (CML) is a reflection of the unsustainable prices of cancer drugs: from the perspective of a large group of CML experts. Blood. 2013; 121:4439–4442. 18. Knapp S, Sundström M. Recently targeted kinases and their inhibitors-the path to clinical trials. Curr Opin Pharmacol. 2014;17:58–63. 19. Emmons W, O’Regan J, Brand M. Note on pharmaceutical industry regulation. Case study. Harv Buisniess Rev. 1991:10. 20. Lasagna L. The development and regulation of new medications. Science. 1978;200:871–873. 21. Ward MR. Drug approval overregaultion. Regulation. 1992;15:47. 22. Kim JH, Scialli AR. Thalidomide: the tragedy of birth defects and the effective treatment of disease. Toxicol Sci. 2011;122:1–6. 23. Greene JA, Podolsky SH. Reform, regulation, and pharmaceuticals — the Kefauver–Harris Amendments at 50. New England J Med. 2012;367:1481–1483. 24. Waring MJ, Arrowsmith J, Leach AR, et al. An analysis of the attrition of drug candidates from four major pharmaceutical companies. Nat Rev Drug Discov. 2015;14:475–486. 25. Kola I, Landis J. Can the pharmaceutical industry reduce attrition rates? Nat Rev Drug Discov. 2004;3:711–715. 26. Bunnage ME. Getting pharmaceutical R&D back on target. Nat Chem Biol. 2011;7:335–339. 27. Gregori-Puigjané E, Setola V, Hert J, et al. Identifying mechanism-of-action targets for drugs and probes. Proc Natl Acad Sci U S A. 2012;109:11178–11183. 28. Bowes J, Brown AJ, Hamon J, et al. Reducing safetyrelated drug attrition: the use of in vitro pharmacological profiling. Nat Rev Drug Discov. 2012;11:909–922. 29. Edwards AM, Bountra C, Kerr DJ, et al. Open access chemical and clinical probes to support drug discovery. Nat Chem Biol. 2009;5:436–440. •• A look at how open access can help in developing new drugs. 30. Munos BH, Chin WW. How to revive breakthrough innovation in the pharmaceutical industry. Sci Transl Med. 2011;3:89. 31. Corbett A, Pickett J, Burns A, et al. Drug repositioning for Alzheimer’s disease. Nat Rev Drug Discov. 2012; 11:833–846. 32. Anand R. Barriers to Alzheimer disease drug discovery and drug development in the pharmaceutical 331 industry. Alzheimer Dis Associated Disord. 2002; 16:S33-39. 33. Robinson DM, Keating GM. Memantine. Drugs. 2012;66 (15):15–34. 34. Cummings JL, Morstorf T, Zhong K. Alzheimer’s disease drug-development pipeline: few candidates, frequent failures. Alzheimer’s Res Ther. 2014;6:37. 35. Brookmeyer R, Gray S, Kawas C. Projections of Alzheimer’s disease in the United States and the public health impact of delaying disease onset. Am J Public Health. 1998;88:1337–1342. 36. Munos B. Can open-source R&D reinvigorate drug research? Nat Rev Drug Discov. 2006;5:723–729. •• A look at how the free availability of information has the potential to accelerate drug translation. 37. Nature Reviews Drug Discovery. Harnessing open innovation. Nat Rev Drug Discov. 2009;8:344–345. •• A look at the potential open innovation holds in the context of drug discovery. 38. Dahlander L, Gann DM. How open is innovation? Res Policy. 2010;39:699–709. •• A look at different models of open innovation and what the concept entails. 39. Chesbrough H, Crowther AK. Beyond high tech: early adopters of open innovation in other industries. R and D Management. 2006;36:229–236. 40. Chesbrough HW. Open innovation: the new imperative for creating and profiting from technology. Boston: Harvard Business School Press; 2003. 41. Filippakopoulos P, Qi J, Picaud S, et al. Selective inhibition of BET bromodomains. Nature. 2010;468:1067–1073. •• Paper detailing the discovery of JQ1. 42. Cohen FJ. Macro trends in pharmaceutical innovation. Nat Rev Drug Discov. 2005;4:78–84. 43. Quigley A, Dong YY, Pike ACW, et al. The structural basis of ZMPSTE24-dependent laminopathies. Science. 2013;339:1604–1607. 44. Kruidenier L, Chung C-W, Cheng Z, et al. A selective jumonji H3K27 demethylase inhibitor modulates the proinflammatory macrophage response. Nature. 2012;488:404–408. 45. Lambert GK, Duhme-Klair A-K, Morgan T, et al. The background, discovery and clinical development of BCR-ABL inhibitors. Drug Discov Today. 2013;18:992–1000. 46. Manley PW, Cowan-Jacob SW, Buchdunger E, et al. Imatinib: a selective tyrosine kinase inhibitor. Eur J Cancer. 2002;38:19–27. 47. Capdeville R, Buchdunger E, Zimmermann J, et al. Glivec (STI571, imatinib), a rationally developed, targeted anticancer drug. Nat Rev Drug Discov. 2002;1:493–502. 48. Din OS, Woll PJ. Treatment of gastrointestinal stromal tumor: focus on imatinib mesylate. Ther Clin Risk Manag. 2008;4:149–162. 49. Chesbrough H. The logic of open innovation: managing intellectual property. Calif Manage Rev. 2003;45:33–58. •• A look into open innovation and intellectual property. 50. Warcoin J. Intellectual property. Nat Rev Drug Discov. 2008;7:369–69. 51. Heller MA, Eisenberg RS. Can patents deter innovation? The anticommons in biomedical research. Science. 1998;280:698–701. 332 Z. ARSHAD ET AL. Downloaded by [University of Southern Indiana] at 09:42 29 April 2016 52. Chesbrough H, Garman AR. How open innovation can help you cope in lean times. Harv Bus Rev. 2009. 53. Roberts M, Wall IB, Bingham I, et al. The global intellectual property landscape of induced pluripotent stem cell technologies. Nat Biotechnol. 2014;32:742–748. 54. Lee WH. Open access target validation is a more efficient way to accelerate drug discovery. PLoS Biol. 2015;13: e1002164. •• A look at some success stories that open access has led to. 55. Murray CJL, Rosenfeld LC, Lim SS, et al. Global malaria mortality between 1980 and 2010: a systematic analysis. Lancet. 2012;379:413–431. 56. Maude RJ, Pontavornpinyo W, Saralamba S, et al. The last man standing is the most resistant: eliminating artemisinin-resistant malaria in Cambodia. Malar J. 2009;8:31. 57. Spangenberg T, Burrows JN, Kowalczyk P, et al. The open access malaria box: a drug discovery catalyst for neglected diseases. PLoS One. 2013;8:e0062906.