Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cell Bio 17- Visual Pathways and Lesions
Overview of Visual Fields
•
•
Geniculostriate Pathway
The geniculostriate (main) pathway relays in the LGN of the thalamus and continues to the primary visual cortex
via the optic radiations
The extrageniculate pathways (~20%) bypass the LGN via the brachium of the superior colliculus and relay in the
pretectal area and superior colliculus
Layers 1, 4 and 6 = contralateral eye inputs
Layers 2, 3, and 5 = ipsilateral eye inputs
Layers 1 and 2 = Magnocellular division
• Light and motion information
Layers 3-6 = Parvocellular division
• Spatial discrimination and color information
Optic Radiations
•
•
•
LGN to visual cortex (geniculostriate pathway)
Inferior fibers (Meyer’s loop) pass through the temporal lobe
Superior fibers pass through the parietal lobe
Cell Bio 17- Visual Pathways and Lesions
Geniculostriate Tract
Optic Radiations
Parietal loop
• Upper LGN to upper bank
Temporal (Meyer’s) loop
• Lower LGN to lower bank
The retinogeniculate and geniculostriate pathways in the sagittal plane (Upside down and backwards)
•
•
Columns of Visual Cortex
Ocular dominance columns and orientation columns in the cortex, and their relationship to the layers of the
lateral geniculate nucleus (LGN)
Ocular dominance columns: Contralateral (C) versus Ipsilateral (I) eye inputs
– Orientation columns within a particular ocular dominance column
Cell Bio 17- Visual Pathways and Lesions
•
•
Primary Visual Cortex
Image produced by primary visual cortex is relatively incomplete, but the basic outline of the stimulus is defined
Primary visual cortex will then project this image to the association cortices for further analysis and
development
Visual Lesions
Definitions
• Lesions always named for visual field deficit, not the physical entity damaged
• Think upside down and backwards
• Scotoma = small deficit
• Anopsia (Anopia) = large deficit
Cell Bio 17- Visual Pathways and Lesions
1. Right optic nerve
• All inputs from the right eye are cut off blindness specific to right eye
2. Optic Chiasm Lesion
• Inputs that would cross are cut off (nasal retinal field from left and right eyes, receiving inputs from left and right
temporal visual hemifields) bitemporal hemianopia
3. Optic chiasm lesion (lateral lesion specific to uncrossed fibers from right temporal retina)
• Inputs from temporal retina are cut (right nasal visual field affected) left hemianopia, right eye only
4. Right optic tract lesion
• Inputs from left nasal retina, right temporal retina are affected (resulting in left visual hemifield deficits) left
homonymous hemianopia
5. Meyer’s Loop Lesion
• Inputs from left nasal retina, right temporal retina are affected (resulting in left visual hemifield deficits), but
now only for the superior visual quadrant left superior quadrantanopia
6. Right optic radiations lesion (both Meyer’s loop and superior/parietal loop affected)
• Inputs from left nasal retina, right temporal retina are affected (resulting in left visual hemifield deficits) left
homonymous hemianopia
7. Right optic radiations lesion (superior/parietal loop affected), or upper bank of calcarine fissure (visual cortex) where
those fibers terminate
• Inputs from left nasal retina, right temporal retina are affected (resulting in left visual hemifield deficits, only for
inferior quadrant since it’s only the superior/parietal loop) left inferior quadrantanopia
8. Right optic radiations lesion (Meyer’s loop affected), or lower bank of calcarine fissure where those fibers terminate
• Inputs from left nasal retina, right temporal retina are affected (resulting in left visual hemifield deficits; superior
visual quadrant since it’s Meyer’s loop) left homonymous hemianopia
Cell Bio 17- Visual Pathways and Lesions
Vestibulo-ocular Movements
Argyll Robertson Pupil
• Involves lesion of pretectum
• Caused by neurosyphilis
• Pupil is small and irregular
• The Argyll Robertson pupil is small and constricts
• Accommodation reflex present
poorly to direct light, but briskly when a target
• Pupillary light reflex absent
within reading distance is viewed ("light-near
• Mnemonic is ARP - PRA
dissociation")
Accommodation Reflex
• Functions to keep object in focus as it moves from far to near distance
• Pathway poorly understood
• Three events occur
• Ciliary muscle fibers contract, Lens thickens, Pupils constrict
Cell Bio 17- Visual Pathways and Lesions
Horner’s Syndrome
Depending on the location of the lesion, some or all of these features will be present:
1. Miosis (constriction of the pupil) with a pupil that is slow to dilate
2. Mild (1-2mm) ptosis (drooping eyelid)
3. Ipsilateral anhidrosis (lack of sweating)
4. Apparent enophthalmos (affected eye appears to be sunken)
•
•
•
•
•
•
•
•
•
•
Associated with a lesion of spinal cord above T1
– Pancoast’s tumor (cancer in lung apex), hemisection, syringomyelia
3-neuron oculo-sympathetic pathway
– 1st neuron: from hypothalamus to Intermediolateral column of spinal cord
– 2nd neuron: to superior cervical (sympathetic) ganglion,
– 3rd neuron: to pupil, eyelids, sweat glands of forehead & face
– Interruption of any these results in Horner’s Syndrome
Holmes-Adie syndrome (HAS)
Neurological disorder affecting the pupil of the eye and the ANS
Characterized by one eye with a pupil that is larger than normal and constricts slowly in bright light, along with
the absence of deep tendon reflexes, usually in the Achilles tendon
HAS is the result of a neurotrophic viral infection that causes inflammation and damage to neurons in the ciliary
ganglion and the dorsal root ganglion
HAS begins gradually in one eye, and often progresses to involve the other eye. At first, it may only cause the
loss of deep tendon reflexes on one side of the body, but then progress to the other side.
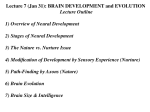
Ross Syndrome
A 34-year-old woman reported that the right side of her face was warmer than the left and had an unusual
propensity for sweating. (Panels A and B were obtained after she had been running.) Six years earlier, anisocoria
(unequal size of the pupils) of the left eye had developed that was diagnosed as Adie's pupil. On exam, she had a
left-sided tonic pupil with light–near dissociation.
In addition, ankle jerks were absent and she had pathological autonomic functions, confirming the presence of
Adie's syndrome.
The occurrence of Adie's syndrome and segmental anhidrosis or hypohydrosis has been referred to as Ross
syndrome and consists of cranial postganglionic parasympathetic and sympathetic dysfunction in association
with more widespread autonomic failure that is rarely clinically relevant.
The course is usually benign with a possible expansion of the dyshidrotic area.
Key Concepts
•
•
Lesions & the visual pathway
Clinical conditions
– Ross Syndrome
– HAS
– Argyll Robertson Pupil
– Horner’s Syndrome