Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
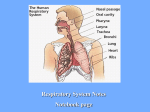
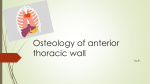
OMM 2- Thoracic Rib and Chest Wall SD Function of Ribs and Sternum Respiration Protection of vital organs Pump for venous and lymphatic return Support structure for the upper extremities Embryology The sternum develops independently in somatic mesoderm in the ventral body wall Two sternal bands are formed on either side of the midline and later fuse to form cartilaginous models of the manubrium, sternebrae, and xiphoid process Sternum Anatomy Manubrium Sternal Notch Anterior to T2 Angle of Louis Articulation of second rib Synchondrosis Anterior to T4 Gladiolus (Body) Xiphoid Process Joint is anterior to T9 OMM 2- Thoracic Rib and Chest Wall SD Rib Nomenclature True ribs: 1-7: Attach directly to the sternum via costochondral cartilage False ribs: 8-10: Attach via a synchondroses to the costochondral cartilage of rib 7 Floating: 11-12: Do not attach to the sternum at all Typical ribs (3-9) will have all of the following anatomical landmarks Tubercle- articulates with corresponding transverse process Head- articulates with corresponding and immediately superior vertebrae via demifacets Neck- between tubercle and head Angle- beginning of anterior curve, 5-6 cm lateral to head Shaft- AKA the body, contains costal grove inferiorly Atypical ribs Rib 1 - articulates only with T1, has no angle and no costal groove Rib 2 – atypical because of large tuberosity on shaft for serratus anterior and lack of costal groove Rib 10 – atypical because articulates with corresponding vertebrae only Ribs 11,12 – articulates only with corresponding vertebrae and lack of tubercles (articulation laterally with the vertebrae) OMM 2- Thoracic Rib and Chest Wall SD Rib Articulations Costochondral Rib 1: Synchondrosis (non-synovial) Ribs 2-7: Synovial articulations Posterior Three articulations Costotransverse joint Superior costovertebral joint (inferior costal facet) Inferior costovertebral joint (superior costal facet) Rule of Three’s Rule of Threes – approximates the positions of the thoracic spinous processes in regard to the transverse processes T1-3—equal (SP compared to TP) T4-6—1/2 level up T7-9—1 level up T10-12—Reverses each level Muscles of Inspiration Principal Intercostalis int. & ext. Diaphragm Breathing takes up to 50% of your caloric expendature every day. Good function of these muscles, rib and vertebral mechanics is vital to the efficiency of your respiration. Thus the importance of this area in OMT OMM 2- Thoracic Rib and Chest Wall SD Diaphragm Central tendon makes up most of the horizontal aspect of the muscle Actual muscular portion of diaphragm is oriented vertically Efficient contraction relies on using the abdominal viscera as a fulcrum and the verticality of the muscle in relation to the chest wall as a lever Major Accessory muscles activated with inhalation Anterior and posterior serratus Serratus Anterior Origin: outer aspects of upper 8 to 10 ribs Inserts: anterior surface of vertebral (medial border of scapula Action draws scapula forward & laterally; rotates scapula in raising arm Serratus Posterior External intercostals Levatores Costarum Sternocleidomastoid Muscle Attaches to clavicle & sternum from the base of the occiput/mastoid Scalenes Attaches from the cervical spine to the first two ribs Scalenus anterior Origin: transverse process of 3rd to 6th cervical vertebrae Inserts scalene tubercle of 1st rib Raises ist rib bends neck forward and rotates to opposite side Scalenus Medius Origin: TP of ist 6 cevical vertebra; Inserts upper surface of 1st rib Raises 1st rib bends neck to same side Scalenus Posterior Oriigin: transverse process of 4th to 6th rib Inserts: outer aspect of 2nd rib Raises 1st & 2nd rib bends neck to same side. Scalenus Minimus Origine tp 7th cerv vertebrae Inserts 1st rib & Pleura Tenses dome of the pleura Muscles of Exhalation Active breathing Intercostalis int. Rectus abdominis Obliques, int. & ext. Transversus abdominis Quiet breathing Results from passive recoil of the lungs Rectus Abdominis Origin: crest & symphysis of pubis Inserts:xiphoid process; 5th to 7th costal cartilages Action: tenses abdominal wall, flexes vertebral column; draws thorax downward OMM 2- Thoracic Rib and Chest Wall SD Intercostal Muscles External lower border of one rib to upper border of rib below Draws ribs together Internal lower border of rib; costal cartilage inserts Upper border of rib and costal cartilage below Draws ribs together Intimi Internal surface of superior border of rib Inserts internal surface of inferior border of rib above Draws ribs together. Latissimus Dorsi Origin: Sp of Vertebrae T7 to S3, thoracolumbar fascia, iliac crest, lowere four ribs inferior angle of scapula Inserts: floor of intertubercular of humerus in bicipital groove Adducts, extends, rotates arms medially. Mechanical pump—fluid model Pressure gradient between the thoracic and abdominal cavities allow lymphatic and venous fluids to flow from the body to the upper thoracic area. Contraction of muscles and pulsation of arteries also helps to propel lymphatic fluids The diaphragm has been shown to play an important role in lymphatic absorption from the peritoneal cavity Costal Lymphatics Parasternal (internal thoracic) lymph nodes Intercostal lymph nodes Diaphragmatic lymph nodes Costal Nerves Intercostal nerves Lie on inferior portion of rib in the costal groove Derived from the sympathetic chain ganglia via white and grey rami communicantes Provide innervation to thoracic and abdominal walls (1 and 2 send fibers to upper extremities, subcostal sends fibers to gluteals) Sympathetic chain ganglia lay just anterior to the rib heads bilaterally Rib motion Best detect motion far away from the axis (with ribs you will feel it move anteriorly better) Pump-Handle motion: Primarily ribs 1-5 (pull up in front, posterior goes down Ribs move anterior and superior with inhalation Motion predominantly in sagittal plane Best palpated at mid-clavicular line Axis of motion is costovertebral-costotransverse line As Inspiration occurs: Anterior aspect moves cephalad (superiorly) Posterior rib head moves caudad (inferiorly) Expiration: Opposite of inspiration! OMM 2- Thoracic Rib and Chest Wall SD Bucket-Handle motion: Primarily ribs 6-10 (lift handle to the side to raise) Ribs move laterally and increase transverse diameter with inhalation Motion predominantly in coronal plane Best palpated at mid-axillary line Axis of motion is a costovertebral-costosternal line The rib shaft is the handle of the bucket Rib shaft lifts during inhalation, falls with exhalation Increases the transverse diameter of rib cage Caliper motion: Primarily ribs 11,12 (book closing and opening) Ribs externally rotate with inhalation Motion predominantly in transverse plane Best palpated 3-5 cm lateral to transverse processes Axis of motion is vertical line Typical vs Atypical Motion “Typical” Ribs: Ribs 3-9 display both transverse axis (pump handle) and AP axis (bucket handle) motion Upper 1/3 ribs- predominant pump handle type mechanics around a transverse axis Middle 1/3 ribs- mix of pump and bucket handle mechanics Lower 1/3 ribs- predominant bucket handle mechanics around an AP axis “Atypical” Ribs Ribs 1,2, 10-12 Rib Somatic Dysfunction Impaired or altered function of related components of the somatic system (body framework): skeletal, arthrodial, and myofascial structures, and related vascular, lymphatic, and neural elements. Identified through palpation to determine the presence of tissue texture changes, asymmetry, restricted motion (barrier) and tenderness OMM 2- Thoracic Rib and Chest Wall SD Specific Structural Dysfunctions Superior subluxations (first rib) A/P subluxations Respiratory Dysfunctions Inhalation SD Pump handle (exhalation restriction) Inhalation SD Bucket handle (exhalation restriction) Inhalation SD Caliper (exhalation restriction) Exhalation SD Pump handle (inhalation restriction) Exhalation SD Bucket handle (inhalation restriction) Exhalation SD Caliper (inhalation restriction) Goal in Rib treatment Improve Rib Motion Improved rib motion modulates sympathetic function Improved rib motion allows for improved respiration and improves diaphragmatic function Improved rib motion increases intrathoracic pressure during respiration, which increases lymphatic and venous return to the heart Decrease Pain Improve spinal mechanics Case Presentation 21 y/o college basketball player with recent injury to L rib cage shows fractured ribs on CXR. Improved with rest and 6-8 weeks post injury returns to cardiovascular exercise with now chest pain and shortness of breath with activity associated with sharp quality better with rest Pt found to have T 6 Ext SLRL lesion Pt with exhalation rib somatic dysfunction of ribs 6-9 Rib General Treatment Principles First unclog the sink!!!(address the Thoracic inlet/CT junction) Treat thoracic spine (especially Nonneutrals Type 2) Warm up the soft tissues Inhalation somatic dysfunction (stuck up need to be brought to knees/down a notch/humbled) – tx the lowest rib Exhalation somatic dysfunction (stuck down pull up by your bootstraps) tx the highest rib with dysfunction Recheck and if not improved with tx focus to identify the key rib or tx the other side (Inhalation on R may be Exhalation on L) When treating an inhalation SD (“stuck up in inhalation”) Treat the lowest rib of the group of ribs that is restricted When treating an exhalation SD (“stuck down in exhalation”) Treat the highest rib of the group of ribs that is restricted OMM 2- Thoracic Rib and Chest Wall SD DDx of Thoracic Pain: Non-traumatic Infection (pnuemonia/bronchitis, effusion/empyema, TB, herpes zoster) Pleurisy or Costochondritis (inflammation) Pneumothorax spontaneous Tumor (Pulm CA, LN CA, distant metastasis, sarcoidosis) Asthma/COPD (bronchospasm with inflammation) Pulmonary embolus Cardiac (ie MI, pericarditis, CHF, aneurysm) Esophageal (ie GERD, Esophagitis, etc) Viscerosomatic (Gallbladder, Pancreas, etc) DDx of thoracic Pain: Traumatic Fracture Pneumothorax (esp tension) Costochondritis Somatic Dysfunction Pulmonary contusion Effusion (cardiac tamponade, hemothorax)