Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
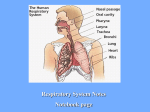
OMM #7 (PTR) Thurs 01/23/03 Turner Slicho, PDF Scribe: Hardeep Hayhre Page 1 of Typical Ribs: Transverse Axis Dysfunction (Note: anything mentioned in class that was not in the power point slides is italicized and bolded also, the rib “head” is the term used for BOTH ends of the rib, where it attaches to the sternum and where it attaches to the thoracic vertebrae) I. Objectives A. Accurately diagnose transverse axis rib somatic dysfunction B. Design and implement appropriate OMT to address somatic dysfunction of the ribs C. Understand the concept of transverse axis rib motion II. Rib Groups: Typical vs. Atypical A. “Typical” Ribs: 1. Ribs 2-10 2. All display both transverse axis (pump handle) and AP axis (bucket handle) motion 3. Upper ribs prefer pump handle 4. Lower ribs prefer bucket handle B. “Atypical” Ribs 1. Ribs 1, 11-12 III. Transverse Axis “Pump Handle” Motion A. Occurs more predominately in upper ribs B. Occurs around a functional transverse axis 1. Axis passes through the posterior tubercle and the head of the rib C. Increases AP diameter of rib cage D. As Inspiration occurs: 1. Anterior rib head moves cephalad (superiorly) 2. Posterior rib head moves caudad (inferiorly) E. As Expiration occurs: 1. Anterior rib head moves caudad (inferiorly) 2. Posterior rib head moves cephalad (superiorly) IV. Inhalation Somatic Dysfunction a.k.a. Inspiratory Lesion A. Think “Stuck in Inhalation” 1. Rib is “stuck” in the inspiratory phase of the respiratory cycle 2. Anterior rib head has moved superiorly, while the posterior head has moved inferiorly 3. A group that doesn’t drop with exhalation (inhalation SD) may be blocked by the most inferior rib 4. Think of it like the rib is stuck in inhalation and can’t move back into exhalation. V. Exhalation Somatic Dysfunction a.k.a. Expiratory Lesion A. Think “Stuck in Exhalation” 1. Rib is “stuck” in the expiratory phase of the respiratory cycle 2. Anterior rib head has moved inferiorly, while the posterior head has moved superiorly 3. A group that doesn’t rise with inhalation (exhalation SD) is often due to most superior rib “pinning the others down” VI. Diagnostic Findings: Rib Somatic Dysfunction A. Anterior narrowing of interspace 1. Above dysfunctional group: Inhalation S/D 2. Below dysfunctional group: Exhalation S/D B. Breathing and/or certain body movements, especially coughing, may precipitate pain C. Tenderness to palpation may be present over the costochondral, costrotransverse or chondrosternal junctions or posteriorly over the rib angles VII. Diagnosis A. Palpate angle of Louis (rib 2) B. Place index finger in 1st and 2nd interspace 1. just lateral to border of manubrium/sternum 2. Place other digits in corresponding spaces 3. Have patient breath slowly 4. Observe any “outliers” in motion C. Palpate for the quality of motion 1. Feel for symmetry and appreciate the differences between inhalation and exhalation a. Sometimes during exhalation, a group of ribs on one side of the rib cage my not move back down and may stay in inspiration VIII. Treatment Tip! A. When treating an inhalation somatic dysfunction (stuck in inhalation) 1. Treat the lowest (caudad) rib of the group of ribs that is restricted B. When treating an exhalation somatic dysfunction (stuck in exhalation) 1. Treat the highest (cephalad) rib of the group of ribs that is restricted IX. Treatment Techniques A. Supine, Direct: Respiratory Cooperation (4821.12B) - “Pump Handle” Inspiratory Lesions 1. Physician stands at head of table, Pt. supine 2. To make sure you are on the right rib, find the rib where it attaches to the vertebrae on the back and push anteriorly on it, you should see that same rib moving on the front of the rib cage 3. Contact the superior aspect of dysfunctional rib (or lowest rib of dysfunctional group) with the lateral margin of his/her thumb at the mid-clavicular line 4. Other hand slides under the patient with fingers hooked under the inferior margin of the posterior angle of rib 5. Flex the upper thorax up to the level of the dysfunctional rib 6. Apply cephalad tension on posterior angle of rib carrying it to restrictive barrier 7. Pt. Instructed to “Take a deep breath and let it out forcibly, as the patient breathes out, push down on the anterior head of the rib and pull up on the posterior head 8. Anterior hand carries anterior portion of dysfunctional rib caudad and holds rib at new restrictive barrier, when the patient inspires again, resist them and try not the let that rib go back into inhalation B. Supine, Indirect: Respiratory Cooperation (4821.12C) - “Pump Handle” Inspiratory Lesions 1. Pt is supine, with physician on side of dysfunction 2. Contact dysfunctional rib: a. Anterior: superior margin of the angle of dysfunctional rib b. Posterior: interspace below dysfunctional rib c. Lateral: Both thumbs contact rib shaft along the mid-axillary line 3. Gently try to squeeze your 2 index fingers on either end of the rib together to disengage the rib, add a little bit of traction 4. Use both hands simultaneously to move both the posterior angle and anterior end of the rib in the direction of inhalation to the point of balanced ligamentous tension, carry it into the motion it likes to do 5. Instruct patient to “inhale deeply and hold your breath as long as you can” C. Supine, Direct: Muscle Energy (4821.22B) - “Pump Handle” Expiratory Lesions 1. Pt supine, with doctor on side of dysfunction 2. Hooks fingers of caudad hand over superior margin of the angle of the dysfunctional rib 3. Apply caudad tension 4. Pt rotates head away from side of dysfunctional rib and places the forearm of the side of the dysfunction over his/her forehead 5. Physician places other hand over the patient’s elbow and forearm 6. Pt applies a contractile force against the physician’s hand a. The patient’s contractile force is directed as follows: i. Towards the contralateral (opposite side) nipple for upper ribs (ribs 2-4) - Pectoralis minor m. ii. Towards the contralateral ASIS for middle ribs (ribs 5-7) - Serratous anterior m. iii. Towards the ipsilateral (same side) hip for lower ribs (ribs 8-10) - Latissimus dorsi m. 7. Contraction is held for 3-5 second, while physician offers isometric counterforce 8. Physician allows tissue to relax, and takes up the slack with the caudad hand at the rib angle to the new restrictive barrier 9. Repeat ~ 3x