Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Conduction anesthesia of the lower extremityA technique and literature review
CHARLES A. REESE, CRNA, PhD
San Diego, California
The author reviews the history,
anatomy, and techniques
(complete with step-by-step
illustrations) for conduction
anesthesia of the lower extremity.
This is part of the continuing series
on conduction anesthesia papers
that were presented at the 44th
AANA Annual Meeting and
ProfessionalSessions held during
August, 1977, in Hollywood,
Florida.
While conduction anesthesia for the
lower extremity has not enjoyed as
colorful a history or as enthusiastic support as similar techniques for the upper
extremity, certain commonalities may
be discerned.
Possibly the first recorded attempts
to produce insensibility of the lower
extremity was Hippocrate's application
of snow and ice to treat hemmorhage
and muscle sprain. 1 Baron von Larey,
Napoleon's surgeon general, noted a
decrease in pain associated with amputation in soldiers who had lain wounded
in battlefield snow for prolonged periods. 2 Such refrigeration techniques prevail today in only limited application
and are generally topical ether or ethyl
chloride sprays. Such techniques are
painful to apply, work only superficially
for short periods of time and may cause
irreversible necrotic tissue changes.
In 1784, George Moore described
an elaborate device by which he could
June/1978
apply compression to vessels and nerves
of the lower extremity to produce pain
relief.8 Such attempts were apparently
short lived, as little is seen of them
after this time.
The first attempt at chemical conduction anesthesia was Taylor's application in 1839, of a morphine paste
placed subcutaneously near the vicinity
of major nerves.4 While any analgesia
that was realized was probably more
due to the systemic effects of the morphine than to diminished nerve conduction, the concept of nerve blocking was
being developed.
Alexander Wood's development of
the hollow metallic needle and syringe
in 1855, 5 along with Gaedicke's isolation of cocaine, 6 ushered in the age of
"local anesthetization." While probably
in limited use, it would prove to be
nearly 30 years before reports appeared
introducing such techniques.
In 1884, Carl Koeller 7 and William
Burke8 described topicalization and intermuscular paraneural injection of cocaine, respectively, to produce surgical
anesthesia. By 1885, more than 60 formal papers, including Halstead's 9 classic article espousing regional anesthesia, had lauded the use of cocaine.
In 1892, Schleich 10 introduced the
use of dilute cocaine solutions for massive "infiltration" techniques for virtually all types of surgical procedures.
Late in the nineteenth century, numerous reports of "poisoning" and
shock following the injudicious use of
cocaine resulted in a widespread search
237
for less toxic agents. Braun, 11 in 1901,
suggested the addition of dilute epinephrine to the infiltration solutions-the
effect being to slow the circulatory uptake and thus decrease the central nervous system effects seen with high circulating blood levels of cocaine.
In 1899, Einhorn 12 synthesized
procaine; however it was 1905 before Braun 18 popularized it for regional
techniques. The introduction of procaine, which was less toxic and longer
lasting than cocaine, gave rise to the
development and introduction of numerous regional nerve block techniques
-the most popular of which was the
subcutaneous infiltration of the surgical
site, both with and without the use of
general inhalation anesthesia (ether).
Several significant developments,
including the introduction of spinal
anesthesia by Bier 14 in 1898, demon-
stration of caudal anesthesia by Sicard"1 in 1901, and the popularization
of peridural anesthesia by Pages16 in
1920, have served to inhibit somewhat
the widespread use of the various specialized blocks of the lower extremity.
As surgical techniques became
more sophisticated, there arose a similar
need for increased sophistication in anesthesia. Most conduction anesthesia tech.
niques for the lower extremity were developed during the 1920's and 193 0 's
by such notable authors as Pitkin 17 and
Labat 18 ; these techniques have withstood the test of time. Many "modern"
techniques are simply modifications of
these originals made possible by a better understanding of applied anatomy
and the pharmacokinetics of the more recently developed chemical agents.
In this review article, the author
makes no attempt to give or deny spe-
Figure 1.
The lumbar plexus is formed by the fir lt four lumbar nerves between the quadratus
lumborum and psoas major muscles.
Ouadratus
lumborum m.
Iliohypogastric n.
Illoingulnal n.
Genltofemoral n.
Lat. femoral
cutaneous n.
Psoas major m.
Iliacus m.
Femoral n.
Obturator n.
(Reprinted with permission from the article by Alon P. Winnie, MD, et al, "The Inguinal Paravascular
Technique of Lumber Plexus Anesthesia," Anesthesia and Analgesia, Vol. 52, Nov-Dec, 1973.)
Journal of the American Association of Nurse Anesthetists
oific credit for the techniques described
but rather attempts to delineate several
conduction anesthesia techniques, as
modified, of the lower extremity which
are currently employed at his institution. Thus, the intent is to attempt to
revitalize techniques which may have
been overshadowed by the frequent employment of spinal or epidural anesthesia in the practice of most anesthetists.
As in all conduction anesthesia
techniques, a keen appreciation of the
anatomy involved is a fundamental prerequisite (sine que none). The anesthetist must first realize that the lower extremity, unlike the upper extremity, is
supplied by major nerves which take
origin from two separate, but related,
central nerve plexus, namely the lumbar
plexus and the sacral plexus.
Lumbar plexus
The lumbar plexus is formed by
the mergence of the roots of the first
four lumbar nerves. 19 (See figure 1.)
It lies anterior to the quadratus lumborum muscle and either posterior to
or within the fascial sheath of the
psoas major muscle and gives rise to
the three primary nerves of the lower
extremity.
The first nerve to emerge is the
lateral femoral cutaneous nerve which
contains elements of L2 and L3. This
nerve courses across the iliacus muscle
Figure 2.
Cutaneous sensory innervation provided by the lateral femoral cutaneous nerve.
LATERAL
ANTERIOR
POSTERIOR
ky
June/1978
MEDIAL
^nom
239
obliquely toward the anterior superior
iliac spine of the pelvis and then passes
below the lateral end of the inguinal
ligament. The lateral femoral cutaneous
nerve provides sensory innervation to
the lateral thigh (figure 2) and has no
motor function.
The second nerve to emerge from
the lumbar plexus is the obturator nerve
which is formed by the anterior primary divisions of the second, third,
and fourth lumbar nerves. The nerve
runs within the substance of the psoas
major muscle along the posterior wall
of the abdomen and lateral to the hypogastric and iliac vessels. It traverses
through the pelvis and enters the lower
extremity via the obturator foramen
where it then divides into anterior and
posterior branches.
In approximately one-third of the
population, an "accessory obturator"
nerve is present. 20 It is formed from
the third and fourth lumbar nerves and
runs tangential to the psoas major muscle to the posterior edge of the pelvis.
It then traverses the pelvis and passes
anterior to the superior ramus of the
pubis where it merges with the anterior
branch of the obturator nerve.
The sensory component of the obturator nerve supplies the cutaneous aspect of the medial thigh as far down as
the knee. (See figure 3.) Additionally,
Figure 3.
Cutaneous sensory innervation provided by the obturator nerve i. This nerve additionally gives rise to articular branches to the hip and knee joints.
LATERAL
ANTERIOR
240
;
POSTERIOR
MEDIAL
Journal of the American Association of Nurse Anesthetists
the anterior branch contributes an articular branch to the hip joint while the
posterior branch supplies a similar articular branch to the knee joint. Block
of the obturator nerve is essential when
use of an upper-leg tourniquet is anticipated or the proposed surgery entails manipulation of the hip and/or
knee joint.
The last nerve to emerge from the
lumbar plexus, the femoral nerve, is its
largest constituent and is formed by the
mergence of the anterior primary divisions of the second, third, and fourth
lumbar nerves. (See figure 1.) The
formed nerve descends from the plexus
in a groove created by the psoas major
and iliacus muscles. It enters the thigh
by passing behind the inguinal ligament
anterior to these muscles and lateral
to the femoral vessels where it immediately divides into two brush-like bundles-an anterior and a posterior
branch.
The anterior or superficial branch
contains the sensory components which
supply the anterior and medial aspect
of the thigh as far down as the knee.
(See figure 4.) The posterior or deep
branch contains the motor fibers which
innervate the quadriceps and the articular fibers which innervate the hip
Figure 4.
Cutaneous sensory innervation provided by the femoral nerve. This nerve additionally gives rise to the saphenous nerve which provides cutaneous sensory innervation to the medial aspect of the lower leg to the medial malleolus.
LATERALTJ
ANTERIOR
June/1978
POSTERIOR
MEDIAL
241
and knee joint. It additionally gives rise
to the saphenous nerve which supplies
cutaneous innervation of the medial aspect of the lower leg to the medial malleolus. As with the obturator, the
femoral nerve must be blocked when
using an upper-leg tourniquet or performing manipulation of the knee or
hip joint.
From the anatomical relationships
previously mentioned, certain consistent
"landmarks" can. be described from
which geometrical projections can be
visualized in order to facilitate isolation of specific nerves and subsequent
performance of percutaneous conduction anesthesia techniques. One such
landmark, which is common to block
techniques of the three nerves presented,
is the inguinal (Poupart's) ligament.
With the patient lying in the supine
position, a mark is made on the skin
from the anterior superior iliac spine
to the pubic symphysis (figure 5), as
these are the boney attachments of this
important ligament. Additional landmarks will be described separately for
each of the specific nerves.
Lateral femoral cutaneous
nerve block
We have noted earlier that the lateral femoral cutaneous nerve passes beneath the lateral end of the inguinal
ligament before entering the muscle
mass of the lateral thigh. An intradermal skin wheal is made with .5% Xylocaine® HC1 approximately / 2 -inch medial to the anterior superior iliac spine
and approximately 1/ 2 -inch below the
inguinal ligament (figure 6). A sterile
/4-inch 23-gauge hypodermic needle,
Figure 5.
The inguinal (Poupart's) ligament provides an important anatomical landmark for lower
extremity nerve block techniques. It attaches to the pubic tubercle and the anterior
superior iliac spine.
If
,-
ll
A4
nctrb
IrquI
rta
Fero
rAl nervC
vetn
3urfoce
iondre&rk3:
Art. sup. spinec
Point of 1rlctclor'
Pubic, bubercltc "
(Reprinted with permission from the book, Regional Block, 4th Edition, by Daniel C. Moore, MD,
Charles C. Thomas Publisher, Springfield, III., 1965.)
Journal of the American Association of Nurse Anesthetists
attached to a sterile 10-cc syringe filled
it has not proven necessary to expose
with an appropriate anesthetic agent,
patients to multiple needle sticks when
is placed through the skin wheal and
but one, placed as described, will suffice.
slowly advanced until a "pop" or loss
As the lateral femoral cutaneous
of resistance is perceived as the needle
nerve contains no motor fibers, conpasses through the tough membranous
firmation of impending nerve block can
fascia lata. With the needle thus propbe assessed by the presence of sensory
erly placed, the syringe is aspirated to
changes in the cutaneous area within
obviate intravascular injection and 8-10
3-5 minutes, depending upon which
cc of the anesthetic agent is injected.
which agent and concentration is used.
A feeling of resistance upon injecting
(See figure 2.)
should alert the anesthetist that he/she
Femoral nerve block
is injecting into muscle mass and not
As was noted previously, the fethe desired fascial plane in which the
moral nerve passes under the inguinal
lateral femoral cutaneous nerve is
found.
ligament anterior to the iliacus and
psoas major muscles and lateral to the
Some authors 21- 24 advocate the use
femoral vessels. These important strucof multiple injections to achieve a "fantures are separated by the thickened
ning" pattern when attempting this
block. It is the author's experience that
iliopectineal fascia and a slip of the
Figure 6.
Anatomical landmarks and a technique for performing a block of the lateral femoral
cutaneous (LFC) nerve. Additional skin markings represent the location at which blocks
are performed for the femoral (FN) nerve and obturator nerve (ON). Other markings
include: PS, pubic symphysis (tubercle); AS, anterior superior iliac spine.
i
^y^-.
"a
' w
1^
^
^--
am-
/
4<
C.
gfF
(Reprinted with permission from the book, Regional Block, 4th Edition, by Daniel C. Moore, MD,
Charles C. Thomas Publisher, Springfield, III., 1965.)
June/1978
psoas major muscle. (See figure 7.)
Pulsation of the femoral artery is palpated and a skin wheal is made approximately 1/2 -inch lateral to the pulse
and distal to the inguinal ligament.
(See figure 6.) This location is directly
anterior to the femoral nerve prior to
its division.
A sterile 1/ 4 -inch 21-gauge hypodermic needle with a sterile 10-cc
syringe, filled with an appropriate anesthetic agent, is placed through the skin
wheal. One lead of a commercially
available "peripheral nerve stimulator"
is attached to the needle with a small
"alligator" clip while the second lead
is clipped to an adhesive EKG pad
placed elsewhere on the patient's
body. 25 (Figure 8.)
With the stimulator's output at the
desired level and the frequency set at
one stimulation per second, the needle
is slowly advanced perpendicular to the
skin until involuntary contractions of
the quadriceps muscles are noted in
unison with the stimulator's pulsation.
This will indicate that the needle tip
has reached the level of the posterior
branch of the femoral nerve.
Occasionally, a patient will per.
ceive a paresthesia radiating to the anteriomedial thigh. This indicates that
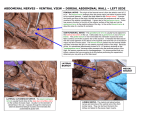
Figure 7.
A cross section at the level of the left inguinal ligament to demonstrate the fascial
"sheath" surrounding the femoral nerve. Note the iliopectineal fascia (unlabeled) and
small portion of the psoas major muscle which separate the femoral nerve and vessels.
-^list\\
i./kL^\1
rMmfw duge
'TI
Obtu
r a.
wame
s V. and a.
Psoes major m.
(Reprinted with permission from the article by Alon P. Winnie, MD, et al, "The Inguinal Paravascular
Technique of Lumbar Plexus Anesthesia," Anesthesia and Analgesia, Vol. 52, Nov-Dec, 1973.)
Journalof the American Association of Nurse Anesthetists
Figure 8.
Demonstration of author's technique for
isolating and blocking the femoral nerve.
Note use of the peripheral nerve stimulator as described in text.
directly at the nerve, and the remaining
7-8 cc of the agent are injected.
The absence of this fade is indicative that the needle tip has been placed
either too shallow or too deep (figure 9).
Figure 9.
When utilizing the peripheral nerve
stimulator for isolating peripheral
nerves, maximum electrical output is
concentrated at the tip of the needle.
(Top to bottom) Needle approaching
nerve; needle at level of nerve; needle
past nerve but still capable of eliciting
response.
the anterior branch of the femoral
nerve has been located. Solicitation of
this paresthesia is not considered essential when utilizing the nerve stimulator technique but will indicate that
the needle is approaching the desired
location. Indeed, nerve damage may
result from overzealous probing for
paresthesias, its cause being either blunt
trauma from the needle or stretching of
nerve fibers from direct intraneural injection of anesthetic agent. 26
The needle is slowly advanced or
withdrawn until maximum contractions
are observed. The syringe is aspirated
to obviate intravascular injection; and
with the stimulator still in use, a test
dose of 2-3 cc of the desired anesthetic
agent is injected. The anesthetist should
observe the anterior thigh (quadriceps)
for immediate (10-15 seconds, depending upon the type and concentration of
agent used) dimunition or "fade" of
muscle contractions. This "fade" is
taken as evidence that the needle is
June/1978
Continued injection at these levels may
hamper further attempts to isolate the
nerve with electrical stimulation. The
needle should be slowly repositioned
until maximal contractions are again
observed. The test-dose/muscle fade sequence is then repeated prior to injecting a final dose.
If the femoral vessels are entered,
as occasionally occurs, the needle is
withdrawn from the patient and compression is applied for 5-10 minutes to
minimize hematoma formation.
Sensory distribution of the femoral
nerve is graphically illustrated in figure
4 and can be clinically evaluated with
an alcohol sponge or needle point. Testing motor function provides a more
reliable and objective indicator of the
onset and completeness of block. As
the femoral nerve provides motor innervation to the quadriceps muscles, the
anesthetist can evaluate the block by
holding the patient's leg as demonstrated in figure 10 and instructing him
to attempt to extend or "straighten" his
lower leg against resistance. The dimunition or inability of the patient to extend
his leg in this fashion is taken as an in
dication of ensuing block.
Depending on the type and concentration of agent(s) employed, onset
of block should be evident in 3-5 minutes, with surgical anesthesia being
present in 15-20 minutes. Duration, of
course, will be dependent upon the
agent, concentration, and presence or
absence of vasoconstrictors.
The use of electrical stimulation to
locate and isolate peripheral nerves has
been described by numerous au-
thors 27
84
but apparently does not enjoy
wide popularity in the practice of regional anesthesia. Since its introduction
by von Perthes, 8 5 in 1912, the technique
has found its primary acceptance by
neurophysiologists for research and
neurologists for diagnostic examinations.
It has been shown that motor fibers
are stimulated at a threshold lower
than that necessary to stimulate sensory
fibers. 27 This allows discreet identification of individual peripheral nerves
at electrical voltages which create no
discomfort for the patient. It should be
emphasized, however, that involuntary
contraction and subsequent movement
of a traumatized extremity may cause
considerable pain. Therefore, when
Figure 10.
To evaluate onset and degree of motor loss following block of the femoral nerve the
anesthetist holds the patient's leg in the manner demonstrated. As the femoral nerve
provides motor innervation of the quadriceps muscle group, the patient's inability to
"straighten his leg" (flexion of quadriceps) against resistance is taken as indication of
ensuing block.
Journalof the American Association of Nurse Anesthetists
utilizing this technique, the anesthetist
is advised that the stimulator should be
discontinued as soon as the desired
nerve is isolated and resumed only to
initiate the test-dose/fade sequence.
Early reports 274 8 concerning this
technique described specially prepared
needles which had been coated with insulating materials, leaving only the tip
of the needle exposed. The apparent belief was that this design would maximize the electrical density at the tip
of the needle and prevent "leaking"
current along the shaft from stimulating muscle or nerve fibers causing misinterpretation of results. Montgomery and coworkers 84 showed that a
minimum of 30% of all current passed
into an uninsulated needle will concentrate and exit through the tip. Likewise,
in our clinical practice, we have found
that commercially available uninsulated
hypodermic or spinal needles are satisfactory with this technique.
We presently employ the Peripheral Nerve Stimulator® (BurroughsWellcome) which is a transistorized,
battery powered device. Voltage output
varies linearly with load resistance (20
volts at 1000 ohms). The markings on
the case represent lineal voltage progressions of approximately 10% (that
is, the fourth mark is equal to 8 volts).
No alterations to this unit are required
or recommended.
We have removed the terminal connectors supplied with the electrode
wires and attached small "alligator"
clips (available from any electrical supply house). When in use, one clip is
attached to the shaft of the probing
needle, the other is attached to the
metal snap of a disposable EKG pad. 25
We have found that a setting of 2-6
Figure 11.
Demonstration of involuntary muscle contraction caused by isolation of peripheral
(sciatic) nerve with electronic nerve stimulator as described in text. Immediate diminution ("fade") of this response following injection of 1-3 cc of local anesthetic agent is
evidence of proper needle placement.
June/1978
volts is required to stimulate the major
peripheral nerves and will do so only
when the needle tip is approximately 3
mm from the nerve substance, 84 a distance which is compatible with localizing nerves of this size.
Figure 11 demonstrates the movement noted from involuntary contractions of the extensors of the lower leg
when the sciatic nerve has been isolated
with the electric nerve stimulator.
Utilization of the nerve stimulator
technique, as described, will yield a
higher success rate than those which
rely solely on the presence of a paresthesia. Such success, no doubt, will instill confidence in students and insure
their continued support of regional
anesthesia. In addition, this technique
allows the performance of conduction
anesthesia for heavily sedated, inebriated, comatose, senile, or psychotic patients.
Obturator nerve block
We have noted that the obturator
nerve is best accessible where it enters
the obturator foramen of the pelvis. An
intradermal skin wheal is made approximately 1-inch below the inguinal
ligament and 1-inch lateral to the pubic
symphysis (figure 12). A sterile 32inch 20-gauge (spinal) needle with a
movable depth indicator is placed
through the skin wheal and is slowly
advanced until resistance (the superior
ramus of the pelvis) is encountered. At
this point, the depth indicator is posi-inch from the
tioned approximately
skin, and the needle is withdrawn to the
subcutaneous tissues. The needle is redirected slightly lateral and caudad while
being slowly advanced until either bone
again is encountered or, if no bone is felt,
the depth indicator comes to rest at the
skin level.
Occasionally, a patient will indicate a paresthesia radiating to the medial aspect of the thigh; however, purposeful solicitation of this paresthesia
is not essential to successful performance of this block. At least one author
has advocated the use of electrical stim-
Figure 12.
Anatomical landmarks and technique of injecting the obturator nerve. The needle in
Position 1 rests against the inferior ramus of the pubic bone. In Position 2, it has been
"walked off" the ramus to rest in the upper inner portion of the obturator foramen.
Injection is made at this location.
.Obturc,tor ni. .
2Obturator
f oro re
.5uperior rarnus
n
of pubic, bone,
(Reprinted with permission from the book, Regional Block, 4th Edition, by Daniel C. Moore, MD,
Charles C. Thomas Publisher, Springfield, III., 1965.)
Journalof the American Association of Nurse Anesthetists
80
ulation to isolate the obturator nerve.
We have been unable to reproduce the
results advocated in this article.
Following placement of the needle
as described, a sterile syringe is attached to the needle and aspirated to
obviate intravascular injection, and 10
cc of anesthetic agent is injected. When
properly positioned, the tip of the
needle rests in a semi-closed space,
formed superiorly by the ramus of the
pubis, and inferiorly medially, and laterally by the obturator internus and
externus muscles. These form a "potential space" around the obturator nerve;
therefore, the anesthetist should encounter little or no resistance upon injection. However, if such resistance is
encountered after injection of 1-3 cc,
the tip of the needle is intramuscular
and should be repositioned.
The motor component of the obturator nerve innervates the adductors
of the leg; therefore, the inability of
the patient to adduct his blocked leg
against resistance will indicate the onset
of chemical block. In conducting this
test, the anesthetist is reminded to keep
the patient's foot straight up. If the patient is allowed to externally rotate the
foot, he can accomplish adduction of
the leg with the adductor magnus (in.
nervated by the sciatic nerve), thus
leading to a "false-negative" examina.
tion.
The sensory distribution of the obturator nerve is graphically illustrated
in figure 3 and can be evaluated with
a saturated alcohol sponge or needle
point.
Lumbar plexus block (Inguinal
paravascular "3:1 block")
In an attempt to decrease the number of injections and the time necessary
to perform three separate nerve blocks,
Winnie and coworkers, 8 6 in 1973, introduced a technique whereby all three
major nerves of the lumbar plexus could
be anesthetized with a single injection.
Their technique is based on the
fact that the lumbar plexus forms in
front of the quadratus lumborum mus-
June/1978
cle and behind the psoas major muscle.
(See figure 1.) Therefore, the three
major nerves are sandwiched between
these muscles and thus are invested by
their fasciae.
As the femoral nerve emerges from
the plexus, it descends in a groove
formed between the psoas major and
iliacus muscles. The fasciae of these
muscles, along with the transversalis
fascia, create a fascial compartment or
"sheath" around this nerve which follows it down to the level of the inguinal
ligament. Below the ligament, the fused
ilio-psoas fascia, the fascia lata, and the
thick ilio-pectineal fascia complete this
sheath, which eventually fuses into the
muscles of the anterior thigh. (See
figure 7.)
Since this fascial compartment is
continuous from the thigh to the lumbar
vertebrae, the authors theorized that injection of an anesthetic agent anywhere
along its course would result in block.
As with other "sheath" techniques, 87-89
the level at which the injection is made
and the volume of anesthetic agent injected will affect the distribution of the
block. The technique they subsequently
introduced has become known as the
"inguinal paravascular" lumbar plexus
block.
Isolation of the femoral nerve, as
described previously, is carried out.
With the needle remaining in place or
advanced slightly cephalad, the index
finger is used to hold firm pressure distal to the site of injection. This is done
to prevent retrograde flow and to promote cephalad flow of the agent as it
is injected.
Some 20-25 cc of agent (1/ pt.
height in inches) is injected, and the
needle is removed. Digital pressure is
maintained and the area is massaged in
a cephalad direction to promote flow up
the sheath.
Figure 13 illustrates the distribution obtained with the injection of 20
cc. From this, it can be seen that the
agent will spread up to the level of the
lumbar plexus, thereby blocking the
three major nerves-the lateral femoral
249
Figure 13.
An x-ray taken immediately following the
injection of 20 cc of an anesthetic agent
with contrast material into the fascial
compartment surrounding the femoral
nerve by the "inguinal paravascular technique." 36 Note that the bulk of solution
flows cephalad to the level of L-4, thus
blocking the components of the lumbar
plexus which innervate the lower extremity.
(Reprinted with permission from the article
by Alon P. Winnie, MD, et al, "The Inguinal
Paravascular Technqiue of Lumbar Plexus
Anesthesia," Anesthesia and Analgesia, Vol.
52, Nov-Dec, 1973.)
cutaneous, the obturator, and, of course,
the femoral. On occasion, in exceptionally tall patients, the lateral femoral
cutaneous nerve may be missed, as it
is the first nerve to leave the plexus
and may not be exposed to the agent.
This can be blocked separately or by
simply increasing the volume of the
agent used.
The authors of this technique88
state that at least three of the potential
risks associated with separate nerve
block can be avoided. These risks are
intravascular injection, trauma to the
nerve from multiple needle exploration,
and systemic toxic reactions secondary
to an overdose of the anesthetic agent.
Lumbar plexus block
(Psoas sheath block)
It was noted earlier that the lumbar
plexus forms within the substance of
the psoas major muscle. This muscle
arises from the inferior borders of the
transverse process of the lumbar vertebrae and the lateral aspects of the lumbar vertebrae and intervertebral discs.
As this muscle is enclosed by a tough
membranous fascia ("sheath"), injection of local anesthesia agents will provide block of the entire lumbar plexus. 40
With the patient in the lateral position and with the side to be blocked
uppermost and the legs flexed into a
"fetal" position, the spinous process of
the third lumbar (L3) vertebrae is
identified. A skin wheal of local anesthesia is made approximately 3-cm lateral to this spine, on the side to be
blocked. A 3/ 2 -inch 20-gauge (spinal)
needle is placed through the skin wheal,
directed approximately 15-20° in a
cephalad direction, and advanced until
the transverse process (L3) is encountered. As the psoas muscle, which is 2-4
cm thick at this point, lies anterior to
the transverse process, the needle is
withdrawn, redirected slightly caudad,
and advanced an additional .5-1 cm so as
to enter the sheath of the psoas muscle.
This needle technique is graphically illustrated in figure 14. Paresthesias to
the anterior leg are occasionally noted
by some patients but are not considered
essential to the performance of the technique.
A syringe is then attached to the
needle and aspirated to obviate intravascular injection; 30 cc of the desired
anesthetic agent are injected. This volume will inject easily with the patient
frequently demonstrating a sensation of
pressure in his flank radiating to his
hip.
Figure 15 demonstrates the distribution of 30 cc of an anesthetic agent
to which contrast medium has been
added. The outline of the psoas muscle
is well defined.
Onset of block is generally rapid
Journalof the American Association of Nurse Anesthetists
Figure 14.
When performing the "psoas sheath block," 4 0 the needle is introduced so as to encounter the transverse process of L-3. The needle is then withdrawn and redirected so
as to pass slightly caudad to the transverse process and is advanced an additional .5-1 cm
into the sheath of the psoas muscle where injection of 30 cc of anesthetic agent is made.
with sympathectomy (vasodilation and
increased skin warmth) of the upper
leg being the first subjective signs
noted. Motor function tests, as described
for the individual nerve blocks, will
provide a more reliable index of onset
and completeness.
Sensory anesthesia will include the
areas innervated by the lateral femoral
cutaneous, the femoral and the obturator nerves-namely the lateral, anterior,
and medial thigh and the medial aspect
of the lower leg down to the medial
malleolus.
As the posterior thigh, posterior
and lateral calf and foot are innervated
by the sciatic nerve, separate block of
this important nerve combined with the
psoas sheath block will provide complete anesthesia of the lower extremity.
spinal nerves and the first three sacral
nerves. These roots converge towards
the greater sciatic foramen to form the
sciatic nerve. (See figure 16.) The
plexus lies on the posterior wall of the
pelvis between the piriformis and hypogastric muscles.
The sciatic nerve, a continuation of
the sacral plexus, is the largest nerve
in the body and is formed by the combination of two separate nerves, the
common peroneal and tibial, contained
within one sheath. The nerve appears
as a wide, flattened band measuring approximately .3-.5 cm in thickness and
1.5-2 cm in width as it leaves the pelvis.
The nerve trunk leaves the pelvis
through the greater sciatic foramen between the piriformis muscles and descends in a groove between the iscial
tuberosity and greater trochanter of the
Sacral plexus
The sacral plexus is formed by the
roots of the fourth and fifth lumbar
femur.
June/1978
At various points along its course,
the sciatic nerve gives off several ar-
Figure 15.
An x-ray made following the injection of
30 cc of anesthetic agent with contrast
media via the "psoas sheath" technique 40
as described in the text. This technique
places the agent within the sheath of the
psoas major muscle, thus blocking the
components of the lumbar plexus (lateral
femoral cutaneous, femoral, and obturator nerves). Note the outline of the
psoas major muscle and slight extravication of media outside the psoas fascia
made during withdrawal of the needle
prior to completion of injection.
ticular and muscular branches. The articular branches arise from the upper
part of the nerve and supply the hip
joint. The short head of the biceps
femoris is supplied by a branch from
the common peroneal portion, while the
tibial portion gives rise to the muscular
branches innervating the semitendinous
semimembranous and adductor magnus.
Sciatic nerve block
(Classic technique)
It was noted earlier that the sciatic
nerve is found in a groove between the
iscial tuberosity and the greater tro-
chanter of the femur. These boney
landmarks form the basis of the classic or "posterior" approach for blocking the sciatic nerve. At this point, the
nerve is located posterior to the ischium,
the obturator internus and gemelli, and
quadratus femoris muscles and is located anterior to the gluteus maximus.
The patient is placed in the lateral
(Simms) position with the leg to be
blocked uppermost, with both legs
flexed as much as possible. A skin mark
is made from the greater trochanter of
the femur to the posterior superior iliac
spine. At the mid-point of this line, a
perpendicular line is drawn inferiorly
and medially for approximately 3 cm
(See figure 17.)
At this point, a skin wheal of local
anesthesia is made, and a 3 -inch 20gauge (spinal) needle is placed through
the skin perpendicular to all skin
planes. One lead of a peripheral nerve
stimulator is attached to the hub of
the needle, and the other lead is attached to a disposable ECG pad placed
elsewhere on the patient's body. (See
figure 18.)
The stimulator's output is placed
on the desired setting and the frequency
is set at 1 stimulation per second. The
needle is slowly advanced until maximal
stimulation (contraction) of the muscles innervated by the sciatic nerve, in
particular the extensors of the foot, are
noted. (See figure 11.) Paresthesia radiating to the foot may be elicited during this maneuver but is not considered
essential when utilizing this technique.
A 10-cc syringe, filled with the desired anesthetic agent(s), is attached
and aspirated to obviate intravascular
injection. A test dose of 1-2 cc is injected and the foot is observed for
"fade" as described elsewhere in this
paper. Upon demonstration of this indicator, the remainder of the agent is
injected and the needle is withdrawn. Onset of block, depending on the agent and
concentration used, will be noted in 3-5
minutes with surgical anesthesia being
present in 15-20 minutes.
As prolonged involuntary move-
Journalof the American Association of Nurse Anesthetists
Figure 16.
Origin of the sacral plexus and sciatic nerve.
(Reprinted with permission from the book, Principles of Anesthesia, by Vincent J. Collins, MD, Lea
and Febiger Publisher, Philadelphia, Pa., 1976.)
Figure 17.
The classic (Labat's) technique of sciatic nerve block: a line is drawn from the
greater trochanter of the femur to the posterior superior iliac spine. A second line is
dropped perpendicular at its midpoint. A skin wheal and insertion of the probing
needle are made approximately 3 cm down this line.
Greater
i trochonter
S
for sciatic n.
Rint of injection
Post. sup. iliac spine
/
(Reprinted with permission from the article by Alon P. Winnie, MD, "Plexus Block for Lower
Extremity Surgery," Anesthesiology Review, Vol. 1, 1974.)
June/1978
Figure 18.
Author's technique for sciatic nerve block. Note the classic landmarks and use of the
electronic nerve stimulator to isolate the nerve.
Journal of the American Association of Nurse Anesthetists
Figure 20.
As the sciatic nerve provides motor innervation to the extensors of the leg and foot, the
patient's inability to (A) extend the lower leg or (B) extend the foot against resistance is
taken as evidence of ensuing block.
20-A
20-B
June/1978
ment of the lower extremity may cause
unnecessary discomfort for the patient,
the anesthetist is reminded to discontinue the stimulator as soon as the sciatic nerve is located and resume it for
only a short time to demonstrate the
test-dose/fade sequence.
The sensory innervation of the
sciatic nerve is graphically illustrated
in figure 19 and easily can be tested
with an alcohol sponge or pin point.
The onset of diminished motor function
provides a more objective indicator of
block onset and completeness. As the
sciatic nerve provides motor innervation of the flexors of the lower leg, the
patient's diminished ability to flex his
leg against resistance is considered indicative of impending block. The sciatic
nerve additionally innervates the extensors of the foot. Therefore, the patient's decreased ability to extend the
lower leg (figure 20A) or foot (figure
20B) against resistance is considered
a favorable sign of ensuing block.
Sciatic nerve block
(Alternate methods)
Occasionally, it is impossible or
unduly painful to place the patient in
the lateral position. As a result, several
alternate approaches to the sciatic nerve
have been described, including the anterior approach by Beck, 41 the lateral
approach by Molesworth 42 or Ichiya.
nagi, 48 and a posterior approach with
the patient in the supine position by
Winnie. 44
It is beyond the scope of this article to attempt to present these techniques in detail. The reader is encouraged to consult the original works of
these authors to learn the specifics of
their techniques.
Combined lumbosacral plexus
block
In 1974, Winnie and coworkers 44
introduced a technique by which both
the lumbar and sacral plexus could be
anesthetized with a single injection.
Figure 21.
Anatomical landmarks described by Winnie et al44 for performing the "combined
lumbosacral plexus block." See text for details of this technique.
Ili
ac
c re s t
Pbst sup.
iliac spine
.
Spinous process
(Reprinted with permission from the article by Alon P. Winnie, MD, "Plexus Block for Lower
Extremity Surgery," Anesthesiology Review, Vol. 1, 1974.)
256
Journal of the American Association of Nurse Anesthetists
This is possible as both the plexus are
sandwiched between the quadratus lumborum and psoas major muscle and
thus are enclosed by the fasciae of these
muscles. The concept then is to inject
a volume of drug into this space which
is adequate to spread caudad and cephalad sufficiently to be exposed to both
plexus. Their work suggests that 40 cc
is an appropriate volume.
The patient is placed in the lateral
(Simms) position with the leg to be
blocked uppermost and the knees flexed
towards the chest. A skin line is drawn
between the iliac crests. This line will
pass through the L 4-5 vertebral interspace.
Figure 22.
An x-ray taken following the injection of
30 cc of an anesthetic agent and contrast
media via the technique of "lumbosacral
plexus block" as described in the text.
This technique places the agent in the
fascial space between the psoas major
muscle (anterior) and the quadratus
lumborum and iliacus muscles (posterior),
thus blocking both the lumbar and sacral
plexus.
A second line is made, on the side
to be blocked, parallel to the spine
through the posterior superior iliac
spine (figure 21.) A skin wheal of local
anesthesia is made at the intersection
of these lines. A 31/2-inch 20-gauge
(spinal) needle is placed through the
skin wheal and is advanced slowly in
a mesiad direction until the transverse
process of L-4 is encountered. The
needle is withdrawn to the subcutaneous
tissues and redirected slightly caudad.
It is then advanced (approximately 5-6
cm) until a paresthesia radiating to the
leg is obtained. On occasion, the use of
a nerve stimulator, as described earlier,
has elicited good results.
When the nerve plexus is isolated,
40-cc of the desired anesthetic agent is
injected. Figure 22 illustrates the spread
of this volume within the "lumbosacral
sheath." The patient is then placed in
the supine position; and evaluation of
motor function, as previously described,
is carried out. Depending on the agent
and its concentration, motor loss will be
evident in 3-5 minutes, with surgical
anesthesia complete in 15-20 minutes.
DeKrey 4 0 and Chayen 45 have described similar single injection lumbosacral plexus techniques. The reader is
encouraged to consult their original
works for specifics of their techniques.
Discussion
It is acknowledged that the clinician cannot master the skills of conduction anesthesia simply from published
materials. Indeed, the reader is advised
against unsupervised attempts at these
techniques. The purpose then, of this
and a companion article 46 in the June,
1977 issue of the AANA Journal has
been to chronicle the historical, anatomical, and technical developments which
have lead to the descriptions of various
techniques for providing conduction
anesthesia of the human extremities. In
addition, the author's modifications of
some techniques have been described.
June/1978
REFERENCES
(1) Little, David M. Jr., 1972. Classical File,
Survey of Anesthesiology. 16:278.
(2) Ibid, 279.
(3) Lundy, J. S. 1942. Clinical Anesthesia,
W. B. Saunders Co., Philadelphia, Pa. p. 707.
(4) Bartholow, R. 1873. Manual of Hypodermic Medication, 2nd Edition, Philadelphia, Pa.,
J. B. Lippincott Co.
(5) Wood, A. 1855. New Method of Treating
Neuralgia by the Direct Application of Opiates
to the Painful Parts, Edinburgh M.&S. Quart.
J. 82:265.
(6) Braun, H. 1914. Local Anesthesia, Lea and
Febiger, Philadelphia, Pa.
(7) Koller, C. 1884. The Use of Local Anesthesia on the Eye. Preliminary Report. Rostock,
Universitiits-Buchdruckereivon Adler's Erben,
pp 60-63, Translation in Foundations of Anesthesiology by Faulconer and Keys, pp 773-775,
Volume 2.
(8) Burke, W. C. Jr. 1884. Hydrochlorate of
Cocaine in Minor Surgery, New York Medical
Journal, 40:616-617 (Nov. 29).
(9) Halstead, W. S. 1885. Practical Comments
on the Use and Abuse of Cocaine; Suggested
by Its Invariably Successful Employment in
More Than A Thousand Minor Surgical Operations, New York Medical Journal, 42:294-295
(Sept. 12).
(10) Schleich, K. L. 1895. A New Method of
Local Anaesthesia (Infiltration Anaesthesia),
International Clinics (5th series), 2:177-192
(July).
(11) Braun, H. 1903. The Addition of Epinephrine to Cocaine for Local Anesthesia Archiv
fur klinische Chirurgie 69:541-591, Translated
in Foundations of Anesthesiology by Faulconer
and Keys, Volume 2, pp 834-842.
(12) Einhorn, A. 1899. On the Chemistry of
Local Anesthetics, Muncher medicinische
Wochenschrift, 46:1218-1220 (Sept. 12), Translated in Faulconer and Keys, pp 801-807.
(13) Braun, H. 1905. Several New Local Anesthetic Agents, Deutsche medizinishe Wochenschrift, 2:1667-1671 (Oct. 19), Translated in
Faulconer and Keys, pp 842-847.
(14) Bier, A. K. G. 1899. Experiments in Cocainization of the Spinal Cord. Deutsche Zeitschcift fur Chirurgie, 51:361-369 (April),
Translated in Faulconer and Keys, pp 850-858.
(15) Sicard, J. A. 1901. The Extradural Injection of Agents by the Sacrococcygeal Route,
Comptes rendus hebdomadaires des seances et
memoires de la Societe, 53:396-398 (April 20),
Translated in Faulconer and Keys, pp 921-923.
(16) Pages, F. 1921. Metameric Anesthesia,
Rirista de la sanidad militar, Madrid, s.3, 11:
351-365, pp 385-396. Translated in Faulconer
and Keys, pp 927-945.
(17) Southworth, J. L.; Hingson, R. A. (eds).
1953. Pitkin's Conduction Anesthesia, J. B.
Lippincott Co., Philadelphia, Pa.
(18) Labat, G. 1923. Regional Anesthesia, Its
258
Technic and Clinical Application, Second Edition, W. B. Saunders Co., Philadelphia, Pa.
(19) Cray, H. 1973. Anatomy of the Human
Body, 29th American edition, Edited by Charles
Mayo Goss, Lea and Febiger, Philadelphia, Pa.
(20) K.iser, R. A. 1949. Obturator neurectomy
for
anatomic study of obturator and
accessory obturator nerves, Journalof Bone and
Joint Surgery (31 (A) :815.
(21) Labat, loc. cit.
(22) Eriksson, E. 1969. Illustrated Handbook
in Local Anesthesia, Year Book Publishers,
Chicago, Ill. p. 102.
(23) Bridenbaugh, I. D. 1963. Lower Extremity Nerve Blocks, International Anesthesia Clinics, 1:745-753.
(24) Moore, D. C. 1965. Regional Block, 4th
edition, Charles C. Thomas Co., Springfield,
Ill. p. 295.
(25) Pue, A. 1976. Disposable EKG Pads for
Peripheral Nerve Stimulation, Anesthesiology,
(Correspondence) 45(1) :107-108.
(26) Liifstrom, B., Wennberg, A. & Widen,
L. 1966. Late disturbances in nerve function
after block with local anesthetic agents-An
electroneurographic study. Acta anaesthesiologica Scandinavica, 10:111.
(27) Sarnoff, S. J., Sarnoff, L. C. 1951. Prolonged peripheral nerve block by means of
indwelling plastic catheter. Treatment of Hiccup (Note on the electrical localization of
peripheral nerve), Anesthesiology, 12:270-275.
(28) Pearson, R. B. 1955. Nerve Block in
Rehabilitation: A Technic of Needle Local.
ization, Archives of Physical Medicine and
Rehabilitation, 36:631-633.
(29) Greenblatt, G. M., Denson, J. S. 1962.
Needle nerve stimulator-locator: nerve block
with a new instrument for locating nerves,
Anesthesia and Analgesia, 41:599-602.
(30) Magora, E., Rozin, R., Ben-Menachem,
Y., et al. 1969. Obturator nerve block-an
evaluation of technique, British Journal of
Anaesthesia, 41:695-698.
(31) Wright, B. D. 1969. A new use for the
Block-Aid Monitor,® Anesthesiology, 30:236237.
(32) Koons, R. A. 1969. The use of the
Block-Aid Monitor,® and plastic intravenous
cannulas for nerve blocks, Anesthesiology,
31:290-291.
(33) Chapman, G. M. 1972. Regional nerve
block with the aid of a nerve stimulator,
Anaesthesia, 27(2) :185-193.
(34) Montgomery, M. B., et. al. 1973. The
use of the nerve stimulator with standard unsheathed needles in nerve blockade, Anesthesia and Analgesia, 52(5):827-831.
(35) Perthes von, G. 1912. Uker leitung.
saniisthesie unter zuhilfenahme elektrischer
reiqung, Med WVschr, 47:2545-2548.
(36) Winnie, A. P., Ramamurthy, D. Z. 1973.
The Inguinal Paravascular Technique of Lumbar Plexus Anesthesia: The "3-in-1 Block,"
Anesthesia and Analgesia, 52(6) :989-996.
coxalgia;
Journalof the American Association of Nurse Anesthetists
(37) DeJong, R. H. 1961. Axillary Block of
the Brachial Plexus Anesthesiology, 22:215.
(38) Winnie, A. P., Collins, V. J. 1964. The
Subclavian Perivascular Technique of Brachial Plexus Anesthesia, Anesthesiology, 25:
353-363.
(39) Winnie, A. P., 1970. Interscalene Brachial Plexus Block, Anesthesia and Analgesia,
49:455-466.
(40) DeKrey, J. A. 1973. Unpublished manuscript. Presented at the 47th Congress of the
International Anesthesia Research Society,
March 11-15, 1973, Bal Harbour, Fla.
(41) Beck, G. P. 1963. Anterior Approach to
Sciatic Nerve Block, Anesthesiology, 24(2) :
222-224.
(42) Molesworth, H. W. L. 1944. Regional
Analgesia, H. K. Lewis Co, London, Eng. p.
40.
(43) Ichiyanagi, K. 1959. Sciatic Nerve
Block: Lateral Approach with the Patient
Supine, Anesthesiology, 20(5) :601-604.
(44) Winnie, A. P., Ramamurthy, S., Durrani, Z., et. al. 1974. Plexus Block for Lower
Extremity Surgery, Anesthesiology Review,
1:11-16.
(45) Chayen, D., Nathan, H., Chayen, M.
1976. The Psoas Compartment Block, Anesthesiology, 45(1) :95-99.
(46) Reese, C. A. 1977. "Conduction Anesthesia of the Upper Extremity-A Literature
and Technique Review," AANA Journal,
45(3) :267-278.
ADDITIONAL READING
(1) Faulconer, Albert Jr. and Keys, Thomas
E. 1965. Foundations of Anesthesiology Volume 2, Charles C. Thomas Co., Springfield,
Ill.
ACKNOWLEDGEMENT
The author wishes to acknowledge the
kind professional assistance given to him by
Captain Clyde W. Jones, MC, USN, Chair.
man, Department of Anesthesiology and Captain John A. DeKrey, MC, USNR, Assistant
Chairman, Naval Regional Medical Center, San
Diego, California.
June/1978
AUTHOR
Charles A. Reese, PhD, CRNA, earned
his BS in Nursing from the University of
Oklahoma, Norman, Oklahoma; his BS in
Nursing Anesthesia from the George Wash.
ington University, Washington, D.C.; his
MBA in Health Services Management from
National University, San Diego, California;
and his PhD in Health Services Administration from California Pacific University, San
Diego.
Dr. Reese is presently a Lieutenant Commander in the U.S. Navy Nurse Corps and
serves as Clinical Coordinator of the Navy
Nurse Corps Anesthesia School at the Naval
Regional Medical Center, Portsmouth, Va.
This paper was prepared while Dr. Reese
was Clinical Coordinator of the Nurse Corps
Anesthesia School at the Naval Regional
Medical Center, San Diego, California. This
material, along with that which appeared in
his earlier article, "Conduction Anesthesia
of the Upper Extremity-A Literature and
Technique Review" (AANA Journal, June,
1977, Vol. 45 pp. 267-278) are taken from Dr.
Reese's presentation on "Conduction Anesthesia for the Extremities" which he gave at
the 44th AANA Annual Meeting and Professional Sessions in August, 1977 in Hollywood,
Florida.
The author wishes to state that the opinions or assertions contained in this article
are his private views and are not to be construed as official and or reflecting the views
of the Department of Anesthesiology, Naval
Regional Medical Center, San Diego; the
Navy Nurse Corps; the Department of the
Navy; or Department of Defense.