Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Cardiovascular disease wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Myocardial infarction wikipedia , lookup
Cardiac surgery wikipedia , lookup
Marfan syndrome wikipedia , lookup
Turner syndrome wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Coronary artery disease wikipedia , lookup
Aortic stenosis wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
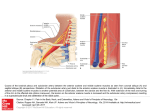
Journal of the association of physicians of india • vol 63 • january, 2015 59 A Rare Cause of Dysphagia Kommerell’s Diverticulum Pathik Parikh*, Mukesh Nasa**, Sandeep Patil*, Jatin Patel*, Prasad Bhate*, Prabha Sawant*** Abstract A right-sided aortic arch with an aneurysm of the aberrant subclavian artery is a rare disease. We report a case of Kommerell’s diverticulum of an aberrant left subclavian artery in a patient with a rightsided aortic arch with associated ventricular septal defect. Fewer than 50 cases have been reported in literature so far. Our patient presented with short duration of dysphagia without any syncope or left subclavian steal syndrome. The major morbidity was caused by Barrett’s oesophagus with reflux and a mixed paraoesophageal and hiatal hernia. There was associated psoriasis. An attempt at repair was not undertaken because of the high operative risk and a small aneurysm. Left thoracotomy for direct repair of Kommerell’s diverticulum is a simple and safe method. Introduction A right-sided aortic arch first described over 200 years ago 1 is an uncommon congenital defect of the aorta. It is usually associated with cardiac anomalies. This anomalous aortic arch remains asymptomatic unless an aneurysmal dilatation of artery develops, leading to compression of surrounding structures and increased risk of arterial rupture.This usually occurs at the level of the take-off of an aberrant left subclavian artery and is known as a Kommerell’s aneurysm. In spite of its rarity, We here report a similar case of right sided aortic arch with Kommerell’s aneurysm. Case Report * Senior Resident, Superspeciality Medical Officer, ***Professor and Head, Department of Gastroenterology, Lokmanya Tilak Municipal Medical College and General Hospital, Sion, Mumbai Received: 23.09.2013; Accepted: 14.10.2013 ** A 56- year-old woman presented to the outpatient department with dysphagia for two months. She had more difficulty swallowing solids than liquids and there was no improvement with any specific posture. She also had history of regurgitation of gastric contents and retrosternal burning for 6 years. Blackish discolouration of dorsal surface of elbows, knee, nape and even groin was noted. She denied history of syncope, claudication-like symptoms, anorexia and weight loss. The blood pressure difference between the two arms was 20 mm of Hg systolic blood pressure. An upper GI endoscopy showed circumferential ulcerations in the lower oesophagus with a 7 cm hiatus hernia with mucosal biopsy showing Barrett’s oesophagus without any dysplasia. A chest X-ray showed of widened superior mediastinum, with a right-sided aortic knuckle and narrowing of trachea and left major bronchus (Figure 1). 2- D echo showed hypertensive heart disease with mild diastolic dysfunction with a small membranous ventricular septal defect without any evidence of valvular defect. A CT scan of the thorax (Figures 2, 3) was suggestive of a right-sided aortic arch and an aberrant subclavian artery with an aneurysmally-dilated Kommerell’s pouch measuring 2.6 x 2.6 cm. The left common carotid was seen arising as the first branch followed by the right common carotid and lastly the two subclavians. The distal aortic arch was located in prevertebral region and caused anterior displacement of the trachea and the oesophagus. The superior and middle 1/3 rd of the oesophagus were located anterolateral to the descending aorta and was compressed at two places, i.e. between the Kommerell’s pouch and the left common carotid artery at the level of D2-D3 intervertebral disc, and between the descending aorta and MPA at D4-D5 vertebral levels. A small periumbilical defect with omental herniation was noted. A high resolution manometry (Figure 4) was done to evaluate 60 Journal of the association of physicians of india • vol 63 • january, 2015 Fig. 3 : The figure shows the diverticulum (Star) with compression of trachea (arrow) and oesophagus (Arrow Head). The patient however, had no respiratory symptoms Fig.1 : Chest Xray showing widened mediastinum with displaced trachea (Star) (A) Fig. 2 : CECT Thorax suggestive of Right sided Aortic arch (Arrow). The aorta lies on the right side of the spine the significance of compression which showed a high pressure area in midoesophagus corresponding to the arterial compression, and a hiatus hernia. A dermatology opinion indicated that the skin lesions were of psoriasis vulgaris. A cardiothoracic surgery opinion was sought. In view of a small aneurysm and high surgical risk conservative management was advised. The dysphagia of the patient has improved with treatment of GORD. Discussion Kommerell 2 in 1936 reported an aberrant right subclavian artery originating from the descending thoracic aorta of a left sided arch and associated with persistence of a remnant of the right dorsal aorta. The latter appeared as a diverticulum from which (B) Fig. 4 : The figure shows the High Resolution Manometry (A) Normal, and (B) our patient with area of vascular compression. The black area shows localised rise in pressure at the level of mid oesophagus corresponding to site of extrinsic compression. The peristaltic wave appears to be normal. There is also Hiatal Hernia (Arrow) Journal of the association of physicians of india • vol 63 • january, 2015 61 the aberrant right subclavian artery originated. The condition as the diverticulum of Kommerell 2 can occur in in association with a left aortic arch with aberrant right subclavian artery (0.5–2.0% of the population), or a right aortic arch with abnormal left subclavian artery (0.05–0.1%). Fifty percent of right-sided aortic arches are associated with an aberrant left subclavian artery. 3 An aberrant right subclavian artery with a left sided aortic arch is the most common of the anomalies involving the subclavian artery. with relief of symptoms. Simple ligation, however, can lead to ischaemic symptoms, 11 which can be prevented by re-establishment of the blood flow by reimplanting the aberrant vessel to the ascending aorta. 12 Reconstruction of the left subclavian artery should be done in all patients as in young individuals this may prevent arm claudication, and in older patients may avoid the possibility of a subclavian steal syndrome. 5 Subclavian-to-carotid artery transposition or a Dacron graft may be used to revascularise the upper extremity. 13,14 Endoaneurysmorrhaphy is ideal for small Kommerell’s aneurysms with a normal descending thoracic aorta. The adult aortic arch is formed from the fourth primitive left aortic arch while the right fourth arch generally disappears. If the left fourth arch disappears and the right persists, a right aortic arch develops. If both arches persist, they form a double aortic arch or a vascular ring encircling the trachea and oesophagus. There are three main types of right-sided aortic arch: 4 type I, with mirror-image branching of the major arteries; type II, with an aberrant subclavian artery; and type III, with isolation of the subclavian artery where the subclavian artery is connected to the pulmonary artery through the ductus arteriosus. Type I is the most common representing 59% of all right aortic arches, type II 39.5%, and type III 0.8%. 4 Congenital heart anomalies are seen with these anomalies namely, tetralogy of Fallot, pulmonary stenosis with ventricular septal defects, tricuspid atresia, and truncus arteriosus. They are present in 75% to 85% of type I and type III 5.A right aortic arch with tetralogy of Fallot is known as Corvisart’s disease. Tetralogy of Fallot is the most common heart anomaly in type I (93%). 5 A deletion in chromosome 22q11 is known to be associated with a 24% incidence of isolated anomalies of laterality of branching of the aortic arch. 6 A right-sided aortic arch may be asymptomatic. In infancy, symptoms are related to congenital heart anomalies or to compression of mediastinal structures. In adulthood, symptoms are more often the result in early atherosclerotic changes of the anomalous vessels, arterial dissection, or aneurysmal dilatation of arteries with compression of surrounding structures causing dysphagia (dysphagia lusoria), dyspnoea, stridor, wheezing, cough, choking spells, recurrent pneumonia, obstructive emphysema, or chest pain. 7-9 An aberrant subclavian artery may be located behind the oesophagus (80%), between the oesophagus and the trachea (15%), or in front of the trachea (5%). 10 The condition is reported to be associated with 19% risk of rupture of aneurysm, with 100% mortality. Dissection of aorta was a more common feature in another study. Elective surgery for an operative mortality for Kommerell’s aneurysm carries mortality of 16.6%. 15 This aggressive treatment is indicated for aneurysms of 3 cm or greater in diameter. Division of the artery alone is often associated Conclusion Kommerell’s diverticulum is a rare abnormality associated with abnormal origin of subclavian artery. The condition may be asymptomatic and mainly presents with compression of surrounding structures. The mortality with the complicated ruptured aneurysm being high, surgical option should be considered. Acknowledgements We are thankful to the Dean, Staff Research Society and our colleagues for the whole-hearted support. References 1. Fioratti F, Aglietti F. A case of human right aorta. Anatom Rec 1763;45:365. 2. Kommerell B. Verlagerung des Oesophagus durcheine abnorm verlaufende Arteria subclavia dextra (Arteria Lusoria). Fortschr Geb Roentgenstr 1936;54:590-5. 3. Cruz IA, Cantez T. Right-sided aorta. Part 1: Occurring of right aortic arch in various types of congenital heart disease. Br Heart J 1966;28:722-5. 4. Edwards JE. Anomalies of the derivatives of the aortic arch system. Med Clin N Am 1948;32:925-48. 5. CS Cina. Kommerell’s diverticulum and right-sided aortic arch: A cohort study and review of the literature. J of Vascular Surgery 2004;39:131-9. 6. McElhinney DB, Clark BJ III, Weinberg PM, Kenton ML, McDonald McGinn D, Driscoll DA, Zackai EH, Goldmuntz E. Association of chromosome 22q11 deletion with isolated anomalies of aortic arch laterality and branching. J Am Coll Cardiol 2001;37:2114-9. 7. Felson B, Palayew MJ. The two types of right aortic arch. Radiology 1963;81:745. 8. Donatelli F, Pelenghi S, Pocar M, Moneta A, Grossi A. Combined carotid and cardiac procedures: improved results and surgical approach. Cardiovasc Surg 1998;6:506-10. 9. Drucker MH, Symbas PN. Right aortic arch with aberrant left subclavian artery: symptomatic in adulthood. Am J Surg 1980;139:432-5. 10. Gomes MM, Bernatz PE, Forth RJ. Arteriosclerotic aneurysm of an aberrant right subclavian artery. Dis Chest 1968;54:549-52. 11. Hallman GL, Cooley DA. Congenital aortic vascular ring: surgical considerations. Arch Surg 1964;88:666-75. 12. Bailey CP, Hirose T, Alba J. Re-establishment of the continuity of the 62 Journal of the association of physicians of india • vol 63 • january, 2015 anomalous right subclavian artery after operation for dysphagia lusoria. Angiology 1965;16:509-13. 13. Orvald TO, Scheerer R, Jude JR. A single cervical approach to aberrant right subclavian artery. Surgery 1972;71:227-30. 14. Campbell CF. Repair of an aneurysm of an aberrant retroesophageal right subclavian artery arising from Kommerell’s diverticulum. J Thorac Cardiovasc Surg 1971;62:330-4 15. Austin EH, Wolfe GW. Aneurysm of aberrant subclavian artery with a review of the literature. J Vasc Surg 1985;2:571-7.