Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
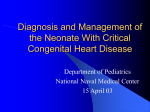
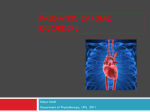
CIRCULATION 402 23. Oyer PE, Stinson EB, Griepp RB, Shumway NE: Valve replacement with the Starr-Edwards and Hancock prostheses: comparative analysis of late morbidity and mortality. Ann Surg 186: 301, 1977 24. Cohn LH, Sanders JH, Collins JJ: Actuarial comparison of VOL 64, No 2, AUGUST 1981 Hancock porcine and prosthetic disc valves for isolated mitral valve replacement. Circulation 54 (suppl III): III-60, 1976 25. Cohn LH, Koster JK, Mee RBB, Collins JJ: Long-term followup of the Hancock bioprosthesis heart valve: a 6-year review. Circulation 60 (suppl I): 1-87, 1979 Atrial Septal Defect in Patients Ages 60 Years or Older: Operative Results and Long-term Postoperative Follow-up MARTIN G. ST. JOHN SUTTON, MB., ABDUL J. TAJIK, M.D., AND DWIGHT C. MCGOON, M.D. Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017 SUMMARY Between 1955 and 1977, 66 patients ages 60 years or older underwent operative closure of secundum atrial septal defect. Of these, 56 (85%) were catheterized preoperatively. The 56 patients were divided into three groups to assess the effects of pulmonary hypertension on operative mortality, symptoms and longevity. The 17 group 1 patients had peak systolic pulmonary artery pressures (PAPs) of less than 40 mm Hg; the 21 group 2 patients had PAPs of 40-60 mm Hg; and the 18 group 3 patients had PAPs of more than 60 mm Hg. Among the three groups, there was no significant difference in Qp/Qs, right or left atrial pressures, right or left ventricular end-diastolic pressures and Qs, although pulmonary vascular resistance was significantly higher (p < 0.01) in group 3 than in group 1. Four patients died, yielding an operative mortality of 6%. All four patients had undergone additional operative procedures. Operative mortality was unrelated to preoperative symptom class, PAP or pulmonary vascular resistance. Forty-seven patients were followed up for 2-20 years (mean 6.6 years), and of these, 41 (87%) improved by at least one functional class. Symptomatic benefit occurred in all groups, regardless of preoperative PAP, pulmonary vascular resistance or functional class. Actuarial survival curves showed that longevity at 5 and 10 years postoperatively was significantly increased (p < 0.01) for patients with atrial septal defect treated surgically compared with that predicted for age-matched patients treated medically. ATRIAL SEPTAL DEFECT is one of the most common forms of congenital heart disease in adults.' The few long-term survival studies of patients with atrial septal defect treated medically have indicated that the average age at death is 39-49 years.2-- Although survival into the eighth and ninth decades has been documented,"-8 there is a yearly attrition rate of 5-10% in patients more than 40 years old who are treated medically.9' 10 Surgical closure of atrial septal defects in children and young adults with large left-toright shunts can be recommended with confidence because surgical mortality is low,'1 the frequent debilitating symptoms that develop in the third to fifth decades of life may be obviated,'1- and life expectanFrom the Division of Cardiovascular Diseases and Internal Medicine, and the Section of Thoracic, Cardiovascular and General Surgery, Mayo Clinic and Mayo Foundation, Rochester, Minnesota. Presented in part at the 28th Annual Scientific Sessions of the American College of Cardiology, Miami, Florida, March 1979. Dr. St. John Sutton's present address: Division of Cardiology, University of Pennsylvania, 3400 Spruce Street, Philadelphia, Pennsylvania. Address for correspondence: A. J. Tajik, M.D., Mayo Clinic, 200 First Street SW, Rochester, Minnesota 55905. Received December 19, 1979; revision accepted November 26, 1980. Circulation 64, No. 2, 1981. cy may return to normal. In contrast, the efficacy of surgical as opposed to medical treatment in elderly patients (60 years of age or older) is still debated. Surgical experience is limited and mortality figures vary and are increased by the higher incidence of pulmonary hypertension and heart failure"'19 and by the necessity of associated atrioventricular valve and coronary artery operations. In addition, the likelihood of long-term symptomatic improvement and the effect on life expectancy after surgery in this age group are unknown. We reviewed a large series of patients with atrial septal defect who were 60 years of age or older. We investigated the effects of preoperative symptam class, preoperative hemodynamics, associated disease, and atrial fibrillation on surgical mortality, postoperative symptom class and longevity. Materials and Methods Between January 1955 and December 1977, 72 patients who were 60 years of age or older had the diagnosis of atrial septal defect established at the Mayo Clinic. The oldest patient was 83 years old. Of the 72 patients, 37 (51%) had the condition diagnosed between 1971 and 1977. The diagnosis of atrial septal defect was established by cardiac catheterization in 62 patients (82%) and by operation in 66 patients (92%). ASD IN THE ELDERLY/St. John Sutton et al. Of the 72 patients, 64 had secundum atrial septal defect and eight had sinus venosus defect associated with partial anomalous pulmonary venous connections. Two patients were considered unsuitable surgical candidates, one because of metastatic carcinoma and the other because of severe pulmonary hypertension, with a pulmonary vascular resistance greater than 20 U*m2. Surgical closure was recommended for 70 patients, but three refused operation and one had an operation at another institution. The 66 other patients (47 females and 19 males, a ratio of 2.5:1), mean age 64.5 years, underwent surgical repair of atrial septal defect at the Mayo Clinic and are the subject of this report. Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017 Clinical Features The correct clinical diagnosis of atrial septal defect before referral for cardiac catheterization or operation was made in 30 of the 66 patients (45%). Primary diagnosis of mitral valve disease with prominent mitral regurgitation presumed on a rheumatic basis was made in 23 patients. Primary diagnosis was considered to be a dilated form of cardiomyopathy in eight patients (12%) and aortic valve disease in three (5%) (only present in one patient). Of the 66 patients, 25 (38%) had atrioventricular valve regurgitation, 14 with mitral regurgitation and 11 with tricuspid regurgitation. The preoperative functional classification of the 66 patients who underwent operation for closure of atrial septal defect was assessed using the New York Heart Association (NYHA) classification. Four patients were in functional class I, 18 were in class II, 20 were in class III and 24 were in class IV. The preoperative roentgenograms of the chest showed that only two patients had normal heart size and that 64 had increased heart size (cardiothoracic ratio . 0.5). Electrocardiograms showed that 30 patients (45%) were in sinus rhythm, 34 (52%) had atrial fibrillation, one (1.5%) had atrial flutter and one (1.5%) had complete atrioventricular block. Thirtyfive percent had right-axis deviation, 56% had complete right bundle branch block and 6% had left ventricular hypertrophy. 403 but six (10.7%). In two of these six patients, the arteriolar resistance was moderately elevated, to 8.1 and 8.5 U*m2, and in the other four patients the arteriolar resistance was markedly elevated to levels greater than 10 U.m2 (10.6, 11.0, 13.2, and 14.3 U.m2). Although mean values for peak systolic PAP were significantly different between groups 1, 2 and 3, there was no statistically significant difference in left atrial pressure, right atrial pressure, Qp/Qs (fig. 1), percent oxygen saturation of systemic arterial blood, right ventricular end-diastolic pressure, left ventricular end-diastolic pressure or systemic index. Pulmonary arteriolar resistance, however, was significantly greater (p < 0.01) in group 3 than in group 1. With increased peak systolic PAP, there was deterioration in functional class: in group 1, 38% of the patients; in group 2, 69%; and in group 3, 76% were in classes III and IV. In addition, there was an increased incidence of atrial fibrillation with increased PAP, shown by the presence of atrial fibrillation in 20% of patients in group 1 and in 67% in each of groups 2 and 3. The remaining 10 patients (15%) were referred for operation without catheterization; the clinical diagnosis was atrial septal defect in four, mitral valve disease in five and pericardial disease in one; in the latter six patients, the diagnosis of atrial septal defect 6. Or. S 4. 0 0 0 0 0) 00 S . 2.0K @00 S0 * *- Results Hemodynamics Fifty-six of the 66 patients (85%) underwent preoperative cardiac catheterization. To investigate the relationship between pulmonary artery pressure (PAP) and functional class and the effects of PAP on surgical mortality and postoperative functional class and survival, patients were arbitrarily divided into three groups. Group 1 consisted of 17 patients with a peak systolic PAP of less than 40 mm Hg; group 2, 21 patients with a PAP of 40-60 mm Hg; and group 3, 18 patients with a PAP of greater than 60 mm Hg (table 1). In 18 (32%) of the 56 patients, PAP was greater than 60 mm Hg, but pulmonary arteriolar resistance was below 7 U_m2 in all [ U aL 3 2 Group 1 I 0 VZ I a 0o 10 I 0 Peak systolic pulmonary artery pressure (mm Hg) FIGURE 1. Relationship ofpulmonary arterysystolic pressure to ratio of the pulmonary-to-systemic flow (Qp/Qs) in 54 patients. CIRCULATION 404 VOL 64, No 2, AUGUST 1981 Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017 TABLE 1. Hemodynamic Data in 56 Catheterized Patients Ages 60 Years or Older with Atrial Septal Defect Group 1 Group 2 Group 3 (n 21) (n =17) (n =18) RAP (mm Hg) 6.5 ± 2.3 8.0 ± 2.9 8.6 ± 3.6 (4 12) (3 -16) (4 12) 7.8 ± 2.5 8.3 ± 2.3 RVEDP (mm Hg) 8.1 ± 3.3 (5 -13) (5 15) (4 -13) 32.7 ± 4.5 47.0 ± 5.4 72.1 ± 11.8 Systolic PAP (mm Hg) (40 - 59) (60 - 94) (24 39) 17.0 ± 4.6 23.9 ± 5.0 12.6 ± 3.4 Diastolic PAP (mm Hg) (6 - 18) (10 - 25) (13 48) Mean PAP (mm Hg) 19.1 ± 3.4 21.4 ± 3.6 43.1 ± 5.6 (22 35) (13 24) (32 63) 8.9 ± 2.9 10.4 ± 3.5 11.3 ± 3.6 PAW or LAP (mm Hg) (6 15) (4 15) (6 15) 2.51 ± 0.63 2.58 ±0.62 2.50 ±0.96 Qp/Qs (1.7 4.2) (1.5 - 3.2) (1.6 3.7) ± ± 2.84 0.80 3.00 ± 0.72 2.61 0.63 Qs (1/min/M2) (1.9 3.7) (1.9 3.6) (1.8 - 4.0) 93.7 ± 3.5 92.8 ± 3.3 94.7 ± 2.6 02 arterial saturation (%) (92 98) (93 - 98) (87 - 97) ± ± ± 28 156 30 156 146 28 SAP Systolic (mm Hg) (110 - 210) (110 210) (103 205) 81 ± 17 Diastolic SAP (mm Hg) 80 ± 13 79 ± 12 (61 97) (59 110) (60 - 114) LVEDP (mm Hg) 11.2 ± 4.4 11.4 ± 2.7 13.3 ± 3.7 (5 -19) (6 -20) (8 -19) (n 9) (n 6) (n 6) 4.10 ± 1.76 2.78 ± 0.92 6.80 ± 5.17 (1.6 - 8.5) (1.2 5.2) (2.8 - 14.3) Values are mean ± SD; ranges are in parentheses. Abbreviations: RAP = right atrial pressure; RVEDP = right ventricular end-diastolic pressure; PAP = pulmonary artery pressure; PAW = pulmonary artery wedge pressure; LAP = left atrial pressure; Qp = pulmonary blood flow; Qs = systemic blood flow; SAP = systemic arterial pressure; LVEDP = left ventricular end-diastolic pressure; Rpa = pulmonary arteriolar resistance. Rpa (U. im2) was made at operation. These 10 patients make up group 4. Systemic hypertension, defined as a resting blood pressure above 150/90 mm Hg, was noted in 25 (38%) of the 66 patients, which was significantly greater (p < 0.01) than in an age-matched normal population. Operation The atrial septal defect was closed by direct suture in 47 of the 66 patients (71%), while in 19 (29%), closure was accomplished using a Dacron patch graft. In eight (12%), patch graft was necessitated by the presence of a sinus venosus defect associated with partial anomalous pulmonary venous connections. In 18 patients (27%), additional surgical procedures were performed: 13 had atrioventricular valve surgery, two aortocoronary bypass grafts, one aortic valve replacement, one partial pericardiectomy and one implantation of a permanent electronic pacing system for chronic complete atrioventricular block preoperatively. The incidence of tricuspid regurgitation necessitating operative correction was not different between the three groups, indicating that severe tricuspid regurgitation varied independently of PAP. Hospital mortality, defined as death within 30 days of surgical closure of atrial septal defect, was 6% (four of 66 patients). The four patients who died had all undergone additional surgical procedures: one aortocoronary bypass graft, two tricuspid valve annuloplasties, and one tricuspid valve replacement. Although the number of deaths was small, there was no statistically significant difference in the mortality rate of patients in functional classes III and IV compared with those in symptom classes I and II, nor was there any difference in mortality rate between patients with mild pulmonary hypertension (group 1) and those with significant pulmonary hypertension (groups 2 and 3). In addition, among the six patients with pulmonary arteriolar resistance (Rpa) greater than 8 U*m2, only ASD IN THE ELDERLY/St. John Sutton et al. 405 1009 one died during operation (Rpa 14.3 Uem2), and this resulted primarily from perioperative myocardial infarction after coronary bypass grafting. Follow-Up Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017 Follow-up information was obtained on all operative survivors. For analysis of long-term results, we elected to include patients who had a minimal followup of 2 years (47 patients). This excluded the patients who underwent permanent ventricular pacing or aortic valve replacement and the survivor with coronary bypass grafts (who were followed up for 9-18 months only). The duration of follow-up was 2-20 years (mean 6.6 years). There were 14 late deaths during follow-up, and these occurred 2.5-17 years (mean 7 years) after operation. Of these 14 deaths, two were in group 1, four in group 2, six in group 3 and two in group 4, a mean of 3, 7, 8 and 6 years, respectively. There was no significant difference in the age at which deaths occurred in the four groups: 67 years in group 1, 73 years in group 2, 70 years in group 3 and 71 years in group 4. Eight patients died of cerebrovascular accidents, six of whom had documented long-standing systemic hypertension. In four of the deaths that involved cerebrovascular accidents, autopsy revealed no intracardiac thrombosis in association with the closure site of the atrial septal defect; the atrial septal defects were completely closed, and in each case, death had resulted from intracerebral hemorrhage and not thromboembolism. None of the four patients was taking oral anticoagulants. Three patients died from congestive heart failure. Two were in functional class IV before operation and remained the same after operation, and one patient deteriorated 5 years after atrial septal defect closure. Three other patients died, one after a mitral valve replacement 4½/2 years later, one of staphylococcal pneumonia and one at home in whom no autopsy was done. Five of the six patients with pulmonary arteriolar resistance greater than 8 U*m2 (range 8.5-14.3 U.m2) were followed up for more than 2 years (mean 5.8 years). One patient died at operation. There was only one late death, which occurred 8 years postoperatively. Survival To assess the yearly attrition rate and the effects of operation on longevity, actuarial survival curves were constructed for patients who survived the operation and were compared with survival curves of an agematched normal population (fig. 2). A survival curve was also constructed using a yearly attrition rate of 7.5%, a figure derived by Campbell9 from the collected long-term follow-up studies of patients who were more than 60 years of age and who were treated medically. These data demonstrated that patients treated surgically lived significantly (p < 0.01) longer than patients treated medically, and this statistical difference first became apparent 4-5 years after operation (fig. 2). Postoperative survival rates in the surgically treated patients at 5 and 10 years were not Years after operation 100O q.) *.. 8 10 12 14 16 18 20 Years after operation FIGURE 2. Survival of patients with atrial septal defect treated surgically compared to survival of age-matched normal population (expected curve) and to survival of patients with atrial septal defect treated medically (unoperated curve). (top) Observed curve represents patients who survived operation. (bottom) Observed curve represents all patients, including operative deaths. significantly different from those of an age-matched normal population; but at 15 years, the sample size of postoperative patients was too small for meaningful statistical comparison with normal subjects or patients treated medically. Postoperative Symptoms Comparison of the preoperative and postoperative symptom classes (fig. 3) in patients followed up for more than 2 years showed that 41 of 47 (87%) were improved by at least one functional class and six were unchanged; of these six patients, two were in class I preoperatively. No patient deteriorated, although one patient developed congestive heart failure 5 years after atrial septal defect closure. Two patients remained in functional class IV postoperatively, and both subsequently died of congestive heart failure 2½/2 years later. CIRCULATION 406 Group Synnptom C 'loss Pre op 1 ~ ~ lI Post-op 0 im X3 (25) No Catheterization Pre-op 2 7 (58) (20) 2 (17) 0 2 2 2 (17) 2 (VT) Totol Group 4 Group 3 7 7 mE Group 2 VOL 64, No 2, AUGUST 1981 (20) 3 3 Post-op 2 (4) 12 15 (32) 4 14 24 (80) (30) (5) 0 (60) .3t 0 (8) FIGURE 3. New York Heart Association functional classification of patients with atrial septal defect. Forty-seven patients werefollowed upfor 2 years or more after operation. Numbers within parentheses are percentages. Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017 Eight patients, who all died suddenly from cerebrovascular accident, had maintained their postoperative symptomatic improvement before death. Improvement in symptoms varied independently of preoperative PAP, right and left atrial pressures, right and left ventricular end-diastolic pressures, Qp/Qs, pulmonary vascular resistance, and preoperative functional class. Postoperatively, functional classes I and II contained 75% of the patients in group 1, 85% in group 2, and 83% in group 3, whereas preoperatively, these classes contained 58% of the patients in group 1, 31% in group 2, and 24% in group 3 (fig. 3). These data indicated that patients in all three groups had symptomatic improvement and that improvement was not confined to group 1 but occurred as frequently in patients with significant pulmonary hypertension (group 3). Furthermore, all five postoperative survivors (preoperative arteriolar resistance more than 8 U m2) experienced good-to-excellent relief of symptoms (three class II and two class I). One patient, after initial improvement, had symptomatic deterioration 5 years later and died 8 years postoperatively. Discussion The controversy regarding the efficacy of the surgical (compared with medical) treatment of patients with secundum atrial septal defect who are 60 years of age or older has remained unresolved because of the small and varied surgical experiences, the scarcity of data regarding the natural history of patients treated medically, and the lack of detailed, long-term followup studies in a large number of patients who have undergone operation. Formerly, pulmonary hypertension, large left-to-right shunts, high right atrial pressure, atrial fibrillation, congestive heart failure, and other cardiac or pulmonary diseases were regarded as contraindications to surgical intervention because of the high mortality and morbidity rates and the small likelihood of either symptomatic benefit or prolongation of life.17' 18 Thus, these strict criteria discouraged surgical repair of atrial septal defect in many symptomatic elderly patients. Although occasionally, a patient with atrial septal defect may remain asymptomatic into the eighth and ninth decades,20 21 in our study, as in other studies,9'-", 16 18 most patients had disabling symptoms long before that age, with two-thirds in functional classes III and IV. The few studies on the natural history of patients with atrial septal defect treated medically indicated that symptoms became progressively more severe with age,2' 4 and this was believed to result from left ventricular dysfunction,22-25 recurrent pulmonary emboli, or repeated pulmonary infection.26 However, left ventricular dysfunction in patients with atrial septal defect in our experience27 was only rarely encountered. The severity of preoperative symptoms in patients 60 years of age or older tended to vary directly with peak systolic PAP, but was independent of right and left atrial pressures, right and left ventricular end-diastolic pressures, Qp/Qs, and the presence of atrial fibrillation. The correlation between functional class and peak systolic PAP was illustrated by the large proportion of patients (58%) in group 1 who were in functional classes I and II compared with the significantly (p < 0.01) smaller percentage (24%) of patients in symptom classes I and II in group 3. However, this relationship between functional class and pulmonary pressure was complicated, because 42% of the patients in group 1 were in functional classes III and IV and the severity of their symptoms could not be explained on the basis of the presence of mitral or tricuspid regurgitation. Similarly, one-fourth of the patients in group 3 were in functional class II, indicating that PAP per se did not necessarily dictate the presence of functional limitation. The chest roentgenogram was of limited value in predicting the severity of the hemodynamic abnormality in any given patient because all but two patients had cardiomegaly, and these two patients had pulmonary artery pressures of less than 40 mm Hg. Electrocardiograms showed a higher incidence of atrial fibrillation with pulmonary hypertension and not, as previously reported,'8 with the magnitude of Qp/Qs, which was not significantly different in patients with sinus rhythm and atrial fibrillation. Electrocardio- ASD IN THE ELDERLY/St. John Sutton et al. Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017 graphic evidence of left ventricular hypertrophy indicated the presence of additional abnormalities systemic hypertension, mitral regurgitation and, in one patient, severe aortic stenosis. Atrioventricular valve regurgitation occurred in 25 (38%) of the 66 patients, 14 of whom had mitral regurgitation and 11 triscuspid regurgitation. In eight of the patients, mitral regurgitation was caused by mitral valve prolapse, an association demonstrated both angiocardiographically28' 29 and echocardiographically30 to be more prevalent in patients with atrial septal defect than in the normal popuiation. Mitral regurgitation, however, was only severe enough to warrant operative repair or replacement in four of the 14 patients. Tricuspid regurgitation was no more frequent in patients with significant pulmonary hypertension (group 3) than in patients with mildly elevated PAP (group 1). Although the incidence of tricuspid regurgitation was less than that of mitral regurgitation, it was repaired more often at operation. The correct preoperative or precatheterization diagnosis of atrial septal defect was made by the referring physician in relatively few cases, probably because atrial septal defect is usually not suspected clinically in the elderly. Diagnostic difficulties arise because of the unobtrusive auscultatory signs of atrial septal defect and the confusion with rheumatic mitral valve disease.21' 81, 32 This confusion occurs because the coexistence of atrial fibrillation, systolic murmurs of tricuspid and mitral regurgitation and diastolic murmurs resulting from increased flow across the tricuspid valve simulates the auscultatory findings of mixed mitral valve disease. The larger number of patients 60 years of age or older with atrial septal defect diagnosed during the more recent years (37 patients, 1971-1977), compared with the earlier decades (35 patients, 1955-1970), does not reflect an increased incidence of atrial septal defect, but rather, greater clinical awareness and the introduction of echocardiography into routine cardiologic practice, which has facilitated the noninvasive recognition of right ventricular volume overload. Pulmonary pressures in patients ages 60 years or older varied widely, but despite the high incidence of pulmonary hypertension, most of the patients still had large left-to-right shunts.18 The size of the left-to-right shunt varied independently of PAP and atrial fibrillation. Prolonged exposure of the pulmonary vascular bed to increased pulmonary blood flow does not invariably result in pulmonary vascular disease, and this was demonstrated by the small proportion10-2' (10.2%) of these patients with pulmonary arteriolar resistance greater than 8 U.m2. This low incidence of pulmonary vascular disease in elderly patients with atrial septal defect may be a spurious finding overall, because patients with atrial septal defect and associated severe pulmonary vascular disease may not survive into the seventh decade. Pulmonary vascular obstructive disease may develop in patients with atrial septal defect in any decade of life, and one cannot predict if this will occur."' 16 The overall operative mortality for atrial septal 407 defect repair compared favorably with that in other studies of older patients (older than 40 years).'6' 18 In this study, no patients died who had closure of atrial septal defect alone. Operative mortality was unaffected by the presence of pulmonary hypertension (group 3), congestive heart failure (functional class IV), the magnitude of the left-to-right shunt, or atrial fibrillation. All the above factors have been regarded as adversely affecting the surgical outcome of atrial septal defect closure as a result of studies of patients operated on by the atrial-well technique.'7 The only factor influencing mortality in this study was associated operative procedures, which were necessary in 27% of patients. Thus, surgical repair of atrial septal defect in the elderly can be performed at an acceptable risk and therefore is recommended even in patients with significant pulmonary hypertension (pulmonary arteriolar resistance greater than 8 U.m2), as demonstrated by the five patients who survived more than 2 years and in whom resistance varied from 8.1-13.2 U*m2. Two of the major aims of this study were to determine the long-term effects of operation on symptoms and longevity. Of the 47 postoperative survivors followed up for a minimum of 2 years, 41 (87%) were symptomatically improved by at least one functional class and six (13%) were unchanged, although one patient who was initially improved deteriorated again 5 years after atrial septal defect closure. Postoperative symptomatic improvement was not confined to patients in group 1; it occurred as frequently in group 3. Most patients experience a large decrease in PAP after closure of atrial septal defect."' 18, 33-35 However, elderly patients, unlike younger patients, have little or no decrease in pulmonary vascular resistance.'6 Thus, the postoperative symptomatic benefit probably results from restoration of the Qp/Qs to unity, and hence a decrease in PAP and right ventricular work, rather than being due to any change in pulmonary vascular resistance. The operation also may improve lung compliance, which had been reduced by the hypertensive, hyperkinetic pulmonary circulation.36 Eight of the 14 late deaths were due to cerebrovascular accidents and involved patients in whom the postoperative symptomatic improvement had been maintained. Thromboembolism causing cerebrovascular accidents is a recognized complication after closure of atrial septal defect and is unrelated to the type of closure;37 that is, patch graft or direct suture. Thromboembolism is reportedly more frequent in patients with atrial fibrillation and severe pulmonary hypertension.37 Although six of the eight patients with cerebrovascular accidents had atrial fibrillation and three had pulmonary hypertension, these six also had long-standing systemic hypertension. Of four patients who died after cerebrovascular accident and on whom an autopsy was performed, three had systemic hypertension and death resulted from intracerebral hemorrhage, not from thromboembolism. No patient had intracardiac thrombosis, and the atrial septal defects were completely closed. In patients with atrial septal CIRCULATION 408 Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017 defect in this age group, cerebrovascular accidents may have resulted from hemorrhage secondary to systemic hypertension rather than from thromboembolism, as previously reported.37 Actuarial survival curves were constructed for patients followed up for more than 2 years to assess the merits of operative closure of atrial septal defect. These data demonstrated that longevity was significantly (p <0.01) increased in patients who were 60 years of age or older who underwent operation, compared with that predicted from survival statistics for patients of the same age with atrial septal defect who were treated medically.9 In addition, the postoperative 5- and 10-year survival rates of patients with atrial septal defect were the same as those for the normal population. Our data, which represent the first long-term follow-up study of a large number of patients 60 years of age or older who underwent operative closure of atrial septal defect, indicate that (1) atrial septal defect in the elderly is not rare and must be considered in a patient with congestive heart failure and associated atrioventricular valve regurgitation; (2) most patients (67%) have disabling symptoms (functional classes III and IV); (3) the severity of symptoms increases with increase in PAP and right ventricular work; (4) most patients are symptomatically improved on a long-term basis by operation; (5) surgical closure can be performed, with a low risk of mortality; (6) operative mortality is not increased by the presence of congestive heart failure or pulmonary hypertension; (7) operation significantly increases longevity and restores the patients' subsequent survival to normal; and (8) operative closure of atrial septal defect can be recommended for all patients 60 years old or older, except for those with the most severe pulmonary vascular obstructive disease and those with associated debilitating medical illnesses that result in shortened survival. Acknowledgment We are grateful to Peter C. O'Brien, Ph.D., for his help with the statistical analysis. Addendum Between January 1978 and December 1980, 18 additional patients ages 60 years or older had operative closure of atrial septal defect (secundum type in 17 patients, sinus venosus in one patient). The mean age was 69 years (range 60-82 years). Atrial septal defect was closed with direct suture in 12 patients (67%) and with patch grafting in six (33%). Associated procedures were performed in eight of the 18 patients (coronary artery bypass grafting in three, mitral valve replacement for severe mitral regurgitation in two, mitral an- nuloplasty in one and tricuspid valve annuloplasty for severe tricuspid regurgitation in three). Severe pulmonary hypertension (peak pulmonary artery pressure 80 mm Hg, pulmonary arteriolar resistance 11 U.m2) was noted in only one of 14 patients (7%) in whom preoperative cardiac catheterization was performed. This patient had an uneventful postoperative course and is symptomatically improved. There was one death (operative mortality 6%). The patient was an 82-year-old woman who underwent associated aortocoronary bypass graft surgery and tricuspid valve annuloplasty. She was dismissed on the twelfth postoperative day but had a cerebrovascular accident on the twentieth postoperative day and VOL 64, No 2, AUGUST 1981 died 8 days later. Autopsy revealed evidence of recent cerebral and myocardial infarctions. The atrial septal repair was intact and no in- tracardiac thrombus was seen. References E, 1. Braunwald Gorlin R: Cooperative Study on Cardiac Catheterization: total population studied, procedures employed, and incidence of complications. Circulation 37 (supplII): 111-8, 1968 2. Campbell M, Neill C, Suzman The prognosis of atrial septal defect. Br Med J 1: 1375, 1957 3. Cosby RS, Griffith GC: Interatrial septal defect. Am Heart J 38: 80, 1949 4. Markman P, Howitt G, Wade EG: Atrial septal defect in the middle-aged and elderly. Q J Med 34: 409, 1965 5. Colmers RA: Atrial septal defects in elderly patients: report of three patients aged 68, 72 and 78. AmJ Cardiol 1: 768, 1958 6. Rodstein M, Zeman FD, Gerber IE: Atrial septal defect in the aged. Circulation 23: 665, 1961 7. Ellis RF, Greaves M, HH: Congenital heart disease in old age: interauricular septal defect with mitral and tricuspid valvulitis. Am Heart J 40: 154, 1950 8. Fontana RS, Edwards JE: Congenital Cardiac Disease: A Review of 357 Cases Studied Pathologically. Philadelphia, WB Saunders, 1962 9. Campbell M: Natural history of atrial septal defect. Br HeartJ 32: 820, 1970 10. Robb GH: Management of atrial septal defect in middle age. Am HeartJ 85: 837, 1973 11. Rahimtoola SH, Kirklin Burchell HB: Atrial septal defect. Circulation 38 (suppl V): V-2, 1968 12. Dalen JE, Haynes FW, Dexter L: Life expectancy with atrial septal defect: influence of complicating pulmonary vascular disease. JAMA 200: 442, 1967 13. Daicoff GR, Brandenburg RO, Kirklin JW: Results of operation for atrial septal defect in patients forty-five years of age and older. Circulation 35 (suppl I): 1-143, 1967 14. Craig RJ, Selzer A: Natural history and prognosis of atrial septal defect. Circulation 37: 805, 1968 15. Ellis Jr, Brandenburg RO, Swan HJC: Defect of the atrial septum in the elderly: report of successful surgical correction in five patients sixty years of age or older. N Engl J Med 262: 219, 1960 16. Gault Morrow AG, Gay WA Ross Jr: Atrial septal defect in patients over the age of forty years: clinical and hemodynamic studies and the effects of operation. Circulation 37: 261, 1968 17. McGoon DC, Swan HJC, Brandenburg RO, Connolly DC, Kirklin JW: Atrial septal defect: factors affecting the surgical mortality rate. Circulation 19: 195, 1959 18. Nasrallah AT, Hall Garcia E, Leachman RD, Cooley DA: Surgical repair of atrial septal defect in patients over 60 years of age: long-term results. Circulation 53: 329, 1976 19. Wolf PS, Vogel SG Jr: Atrial septal Pryor R, defect in patients over 45 years of age: merits of surgical versus medical therapy. Br Heart J 30: 115, 1968 20. Kelly Jr, Lyons HA: Atrial septal defect in the aged. Ann Intern Med 48: 267, 1958 21. Fisher JM, Wilson WR, Theilen Recognition of congenital heart disease in the fifth to eighth decades of life: diagnostic criteria and natural history. Circulation 25: 821, 1962 22. Flamm MD, Cohn KE, Hancock EW: Ventricular function in atrial septal defect. Am J Med 48: 286, 1970 23. Popio KA, Gorlin R, Teichholz LE, Cohn PF, Bechtel D, Herman MV: Abnormalities of left ventricular function and geometry in adults with an atrial septal defect: ventriculographic, hemodynamic, and echocardiographic studies. Am J Cardiol 36: 302, 1975 24. Tikoff G, Schmidt AM, Kuida H, Hecht Heart failure in atrial septal defect. Am J Med 39: 533, 1965 25. Dexter L: Atrial septal defect. Br Heart 18: 209, 1956 26. Mark H: Natural history of atrial septal defect with criteria for selection for surgery. Am Cardiol 12: 66, 1963 S: Hecht JW, FH Jr, JH, J RJ, Blount JHK, JJ EO: HH: J J SERUM DIGOXIN/Eraker and Sasse 27. St John Sutton MG, Tajik AJ, Mercier LA, Seward JB, Giuliani ER, Ritman EL: Assessment of left ventricular function in secundum atrial septal defect by computer analysis of the M-mode echocardiogram. Circulation 60: 1082, 1979 28. Betriu A, Wigle ED, Felderhof CH, McLoughin MJ: Prolapse of the posterior leaflet of the mitral valve associated with secundum atrial septal defect. Am J Cardiol 35: 363, 1975 29. Leachman RD, Cokkinos DV, Cooley DA: Association of ostium secundum atrial septal defects with mitral valve prolapse. Am J Cardiol 38: 167, 1976 30. Lieppe W, Scallion R, Behar VS, Kisslo JA: Two-dimensional echocardiographic findings in atrial septal defect. Circulation 56: 447, 1977 31. Kuzman WJ, Yuskis AS: Atrial septal defects in the older patient simulating acquired valvular heart disease. Am J Cardiol 15: 303, 1965 32. Sommer LS, Voudoukis IJ: Atrial septal defect in older age groups: with special reference to atypical clinical and electro- 409 cardiographic manifestations. Am J Cardiol 8: 198, 1961 33. Braunwald NS, Braunwald E, Morrow AG: The effects of surgical abolition of left-to-right shunts on the pulmonary vascular dynamics of patients with pulmonary hypertension. Circulation 26: 1270, 1962 34. Kirklin JW, Weidman WH, Burroughs JT, Burchell HB, Wood EH: The hemodynamic results of surgical correction of atrial septal defects: a report of thirty-three cases. Circulation 13: 825, 1956 35. Beck W, Swan HJC, Burchell HB, Kirklin JW: Pulmonary vascular resistance after repair of atrial septal defects in patients with pulmonary hypertension. Circulation 22: 938, 1960 36. Davies H, Gazetopoulos N: Lung function in patients with leftto-right shunts. Br Heart J 29: 317, 1967 37. Hawe A, Rastelli GC, Brandenburg RO, McGoon DC: Embolic complications following repair of atrial septal defects. Circulation 39 (suppl I): 1-185, 1969 Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017 The Serum Digoxin Test and Digoxin Toxicity: A Bayesian Approach to Decision Making STEPHEN A. ERAKER, M.D., M.P.H., AND LEWIS SASSE, M.D. SUMMARY The clinician may often be uncertain about the presence of digoxin toxicity. This uncertainty is particularly important when the clinician must make initial thrapeutic decisions about continuing or discontinuing digoxin. We describe a method that helps to clarify the role of the serum digoxin test in decreasing the uncertainty surrounding the diagnosis and treatment of toxicity. The relation between the test and toxicity was first determined in our patient population. An approach to the interpretation of the test based on the likelihood ratio was then developed by combining our data with selected data from the literature. The relation between the pretest risk of toxicity (the estimated risk of toxicity in the population under investigation before the test result is known) and the predictive value of the test was established. This relation was also used to analyze the importance of the degree of elevation of the test. The appropriate threshold probability for institution of treatment of toxicity was then determined by an interview technique. The test was able to make the patient's probability of toxicity cross the threshold probability for treatment of toxicity for an intermediate range of pretest risk. Our analysis suggests that the serum digoxin test may have a critical effect on therapeutic decisions and can be best considered as contributing to the spectrum of risk. THE DILEMMA of the diagnosis and treatment of digoxin toxicity is faced by many clinicians. No diagnostic test can definitely confirm the presence of toxicity. Given this uncertainty, discontinuing digoxin is beneficial when toxicity is present but may be harmful if toxicity is absent; failing to discontinue digoxin may be disastrous when toxicity is present. The value of the serum digoxin test in resolving this dilemma has been questioned.' The magnitude of the problem is indicated by studies that report a prevalence of toxicity on admission to the hospital of From the Division of Clinical Pharmacology, Department of Medicine, Stanford University Medical Center, Stanford, and the Department of Internal Medicine, Kaiser-Permanente Medical Center, Los Angeles, California. Supported in part by a grant from the Southern California Permanente Medical Group and NIH Clinical Pharmacology training grant GM07065. Address for correspondence: Stephen A. Eraker, M.D., M.P.H., Department of Medicine, Veterans Administration Medical Center, 2215 Fuller Road, Ann Arbor, Michigan 48105. Received November 14, 1979; revision accepted November 26, 1980. Circulation 64, No. 2, 1981. up to 20%, with significant morbidity and mortality.2 6 This study was designed to clarify the role of the test in decreasing the uncertainty surrounding the diagnosis and treatment of toxicity.7 The premise of this analysis is that the value of a laboratory result is determined by its ability to influence the diagnostic or therapeutic decision making process. The serum digoxin test can sometimes critically influence this process. The test result is best viewed as part of a spectrum of risk for toxicity. Methods The charts of all patients who had a serum digoxin test ordered at Kaiser Foundation Hospital, Los Angeles, California, from April 1 to April 21, 1977 were requested for review. All patients had received Lanoxin (Burroughs-Wellcome). During the 3-week study period, 1 10 tests on 66 patients were evaluated. Electrocardiographic Data All ECGs or rhythm strips obtained subsequent to the day before the initial test were interpreted by one of the investigators. The ECGs were divided into the Atrial septal defect in patients ages 60 years or older: operative results and long-term postoperative follow-up. M G John Sutton, A J Tajik and D C McGoon Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017 Circulation. 1981;64:402-409 doi: 10.1161/01.CIR.64.2.402 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1981 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/64/2/402 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/