Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Nuclear medicine wikipedia , lookup
Radiation burn wikipedia , lookup
Proton therapy wikipedia , lookup
Industrial radiography wikipedia , lookup
Medical imaging wikipedia , lookup
Center for Radiological Research wikipedia , lookup
Radiation therapy wikipedia , lookup
Neutron capture therapy of cancer wikipedia , lookup
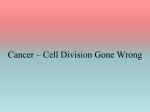
Int. J. Radiation Oncology Biol. Phys., Vol. 59, No. 1, pp. 300 –312, 2004 Copyright © 2004 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/04/$–see front matter doi:10.1016/j.ijrobp.2004.01.026 PHYSICS CONTRIBUTION BRAIN TUMOR TARGET VOLUME DETERMINATION FOR RADIATION TREATMENT PLANNING THROUGH AUTOMATED MRI SEGMENTATION JAMES GLORIA P. MAZZARA, PH.D.,* ROBERT P. VELTHUIZEN, PH.D.,† L. PEARLMAN, M.D.,‡ HARVEY M. GREENBERG, M.D.,‡ AND HENRY WAGNER, M.D.‡ *Department of Radiology and ‡Division of Radiation Oncology, Moffitt Cancer Center, Tampa, FL; †Unilever Research and Development, Edgewater, NJ Purpose: To assess the effectiveness of two automated magnetic resonance imaging (MRI) segmentation methods in determining the gross tumor volume (GTV) of brain tumors for use in radiation therapy treatment planning. Methods and Materials: Two automated MRI tumor segmentation methods (supervised k-nearest neighbors [kNN] and automatic knowledge-guided [KG]) were evaluated for their potential as “cyber colleagues.” This required an initial determination of the accuracy and variability of radiation oncologists engaged in the manual definition of the GTV in MRI registered with computed tomography images for 11 glioma patients. Three sets of contours were defined for each of these patients by three radiation oncologists. These outlines were compared directly to establish inter- and intraoperator variability among the radiation oncologists. A novel, probabilistic measurement of accuracy was introduced to compare the level of agreement among the automated MRI segmentations. The accuracy was determined by comparing the volumes obtained by the automated segmentation methods with the weighted average volumes prepared by the radiation oncologists. Results: Intra- and inter-operator variability in outlining was found to be an average of 20% ⴞ 15% and 28% ⴞ 12%, respectively. Lowest intraoperator variability was found for the physician who spent the most time producing the contours. The average accuracy of the kNN segmentation method was 56% ⴞ 6% for all 11 cases, whereas that of the KG method was 52% ⴞ 7% for 7 of the 11 cases when compared with the physician contours. For the areas of the contours where the oncologists were in substantial agreement (i.e., the center of the tumor volume), the accuracy of kNN and KG was 75% and 72%, respectively. The automated segmentation methods were found to be least accurate in outlining at the edges of the tumor volume. Conclusions: The kNN method was able to segment all cases, whereas the KG method was limited to enhancing tumors and gliomas with clear enhancing edges and no cystic formation. Both methods undersegment the tumor volume when compared with the radiation oncologists and performed within the variability of the contouring performed by experienced radiation oncologists based on the same data. © 2004 Elsevier Inc. Glioma, Tumor volume, Magnetic resonance imaging, Image segmentation, Brain radiation therapy. Treatment protocols for malignant brain tumors known as gliomas generally call for removal through surgical procedures followed by irradiation of the tumor bed. The goal of three-dimensional (3D) conformal radiation therapy is to irradiate the tumor volume while limiting damage to the surrounding normal tissues. Achieving this goal requires accurate determination of 3D treatment volumes. Radiation oncologists traditionally model the brain treatment target through a time-intensive manual procedure involving the outlining of the gross tumor volume (GTV) on numerous two-dimensional imaging “slices” using either computed tomography (CT) or magnetic resonance imaging (MRI) (1). Recently, the search for improvements in target volume definition methodology has concentrated on improved imaging modalities (2, 3). It has been demonstrated that MRI is more sensitive than CT in both lesion detection and in the margin delineation of gliomas (4 –7). However, limitations remain in the delineation of tumor volumes and in the ability of different radiation oncologists to reproduce consistent results (4, 8 –10). Reprint requests to: Gloria P. Mazzara, Ph.D., 2475 Brickell Avenue #2607, Miami, FL 33129. Tel: (305) 858-0266; Fax: (305) 929-1971; E-mail: [email protected] Supported by 1999 RSNA (1) seed grant, entitled “Automatic brain tumor target volume for radiation treatment planning.” Acknowledgments—We would like to thank Computerized Medical Systems and Colin Sims, M.S., product manager, for providing the software and support that made this research possible. Thanks are also due to all the personnel from Moffitt Cancer Center involved in this research, technologists from the Department of Radiology, physicists and dosimetrists from the Department of Radiation Oncology, and specially to Carol Johnson for her assistance in collecting the data. Also, the Department of Computer Science for providing access to their computer workstations; Matt Clark, Ph.D., for helping with the KG data processing; and Hans Christian Beyer for editing the manuscript. Received Jul 22, 2003, and in revised form Dec 19, 2003. Accepted for publication Jan 19, 2004. INTRODUCTION 300 Automated brain tumor volume determination ● G. P. MAZZARA et al. 301 Table 1. Patient demographics Case Age Sex Diagnosis Surgery (days from MRI) MRI type Tumor enhanced RT start (days from MRI) 1 2 3 4 5 6 7 8 9 10 11 65 52 63 69 62 47 52 62 80 47 79 F F F F F M M F M F F AO O GBM GBM GBM GBM AO GBM GBM GBM GBM 3 1 1 3 –89 –24 3 –17 2 –13 –4 Pre Pre Pre Pre Post Post Pre Post Pre Post Post No No Yes Yes Yes Yes Yes Yes Yes Yes Yes 165 70 28 19 16 10 73 6 23 7 7 Abbreviations: MRI ⫽ magnetic resonance imaging; GBM ⫽ glioblastoma multiforme; AO ⫽ astrocytoma; O ⫽ oligodendroglioma; Pre ⫽ presurgery MRI; Post ⫽ postsurgery MRI. Although the technology for conformal radiation treatment planning has developed to a high level of accuracy, the definition of the tumor GTV is still based on time-intensive, highly subjective manual outlining (8, 11, 12). Manual outlining is the type of process that should be an excellent candidate for automation through the development of a computerized segmentation system. At our institution, several techniques of MRI segmentation have been developed and evaluated specifically for use with brain tumors. These methods use the information derived from several magnetic resonance contrasts (i.e., multispectral data). A supervised automated segmentation method requires an operator to select regions of interest on each slice of multispectral MRI data, which, in turn, are used to train the automated classifier. One of these methods, the “k-nearest neighbor” (kNN) system, has been shown to perform better than other tested supervised methods and has been used by many researchers for automated brain segmentation (13). Unsupervised techniques of MR segmentation do not require operator input for the processing of each data set. To automate the tumor volume determination, Clark, Hall, and Goldgof encoded knowledge of the pixel intensity and spatial relationships in the images to create a fully automated segmentation system known as the knowledge-guided (KG) method (16, 17). The KG expert system was initially trained to identify slices of MR images of the brain that contain pathology from slices that do not contain pathology. The KG system’s current incarnation is able to identify and measure tumor tissue from glioblastoma multiforme lesions after gadolinium enhancement in the brain (17). Both the kNN and KG segmentation methods have been clinically applied as a technique for more accurately measuring tumor volume variation in the brain (15, 18). This work evaluates the performance of kNN as a representative of operator-assisted semiautomated segmentation and KG as a promising candidate for fully automated GTV determination. Automatic segmentation of MR images offers the potential to accurately define complex treatment volumes, to speed the contouring process in radiation therapy treatment planning, and to provide a standardized reproducible measurement protocol that can be employed by geographically diverse facilities and physicians in treating brain tumors. METHODS AND MATERIALS Subjects Pre-existing MRI and CT data of 11 patients with primary brain cancer (glioma) were used as the basis in this study. The study was approved under the University of South Florida institutional review board #5253 and required no patient informed consent because only existing data were used and were recorded in such a manner that participants could not be identified. The demographics of this patient group are listed in Table 1. Patient selection was based on available cases collected over a period of 1 year with primary brain cancer (glioma) that had a pre- and posttreatment MRI in our clinic and proceeded to have radiation therapy in Moffitt Cancer Center. In conformance with the standard clinical protocol of the treating facility, these patients had brain surgery and were imaged presurgery with MRI and postsurgery with both MRI and CT. Depending on the treatment protocol selected for each individual patient, the MRI images used in connection with this study may have been taken either before or after surgery. This factor was included as a variable in the study. The CT was used for 3D radiation treatment planning. CT scanning The CT images were obtained using a Siemens CT HiQ spiral scanner (Siemens Medical Systems, Erlangen, Germany) with 512 ⫻ 512 pixel images taken at 4-mm spacing from the vertex through the treatment area and 8-mm slice thickness through the thyroid. Patients were immobilized using a customized mask together with a head rest (MedTec, Orange City, IA). The CT treatment planning system includes MergeCom, the precursor to DICOM data communications. 302 I. J. Radiation Oncology ● Biology ● Physics MRI scanning The patients were imaged in either a 1.5 Tesla GE Signa Horizon (General Electric Co., Milwaukee, WI) or a Siemens Magnetom Symphony with fast gradient systems using the standard multielement head coil. The systems include DICOM data communications. The multispectral data set used for MRI segmentation consisted of 5-mm thick axial anatomic slices T1-weighted, proton-density– weighted, and T2-weighted images obtained with a field of view of 220 mm and reconstructed to a 512 ⫻ 512 pixel image. The T1 scans used for this study were obtained after administration of 0.1 mmol/kg body weight of gadolinium (Gd) MRI contrast material (Gd-DTPA) and using a standard spin-echo sequence with a repetition time (TR)/echo time (TE) ⫽ 400/8 or TR/TE ⫽ 525/17 ms. The protondensity images were acquired using a fluid-attenuated inversion recovery sequence with a TR/TE ⫽ 10002/147 ms or TR/TE ⫽ 9000/110 ms. The T2 images were acquired using a TR/TE ⫽ 3000/104 ms or TR/TE ⫽ 4000/96 ms. Radiation oncologists used axial postcontrast T1 images to define GTV for cases of enhancing tumor or precontrast T2 images for cases involving no tumor enhancement. Image registration Both CT and MRI image sets were transferred to Hewlett Packard workstations running Computerized Medical Systems (CMS) 3-D treatment planning FOCUS software version 2.4.0. Each image set was then transferred to a Dell Inspiron 7000 laptop computer equipped with CMS software for image fusion (Focal Fusion, software release version 1.3) and contouring (Focal Ease, software release version 1.3.0). The laptop computer was dedicated to this research. The CT and MRI data were registered using the Focal Fusion software. Registration was required to permit manual physician contouring on the MRI images. The Focal Fusion software uses maximization of mutual information for fully automatic registration without the need to define fiducial or anatomic points (19). The software also incorporates a manual method for pre- or postinteractive adjustment of the registration. The program writes out a file with a transformation matrix to convert MRI data to the CT coordinates. Quantitative accuracy of the mutual information registration algorithm has previously been validated (19, 20). The final MRI image transformation was evaluated and approved by a radiation oncologist who specializes in neurooncology. The transformation matrix that resulted from the image registration was also used for transforming the contours generated by the segmentation methods to the CT coordinate system. Tumor volume definition The reconstructed and registered MR images were used to define the GTV using the CMS Focal Ease software. The guidelines for contouring required the definition of the GTV (enhancing tumor) from which the clinical and planning Volume 59, Number 1, 2004 (PTV) target volumes would be expanded. The GTV was defined by the Gd contrast enhancement in T1 images or changes in the white matter (edema as defined by T2 MRI images). Each radiation oncologist performed 3 different GTV outlines on each image set for each of the 11 patients, resulting in a total of 33 contours. The three different outlining sessions for each physician were separated by approximately 1 month to prevent memory bias. The laptop computer was brought to each radiation oncologist’s location of choice. The time the radiation oncologists took for the outlining process was measured and recorded as part of this study. All contours, including CT data and MRI transformation files, were copied to a UNIX research network to provide the basis for comparison with the segmentations prepared by the automated expert systems. The expertise of each radiation oncologist is as follows: Physician 1 is a radiation oncologist specializing in neurooncology with 9 years of clinical practice in radiation oncology and involvement with more than 200 glioma brain tumor cases, including brain study trials (21, 22). Physicians 2 and 3 are radiation oncologists, each with more than 20 years of experience in radiation oncology. MRI segmentation. The MRI segmentation methods were run on UNIX workstations (Sun Microsystems, Mountain View, CA) using a network and software environment in which MRI, CT, focus treatment planning systems, the laptop computer, and the image processing laboratory were all integrated to allow for convenient flow of images and other data between platforms. MRI segmentation was performed on the tumor volume data by two different techniques: kNN (13, 14, 23) and the fully automatic knowledge guided system (17, 24). The kNN method requires the user to select training data from each MRI slice. In the present study, a medical physicist selected the training data. Previous research estimated the intra- and interoperator variation arising from training data selection for kNN at 9% and 5%, respectively (14). The KG system requires no user input; therefore, there is no variability in output. The results from the kNN segmentation included scattered tumor-labeled pixels in addition to the main body of pixels identified as “the” tumor. Consistent with the previously reported studies, pixels from the kNN results that were clustered together were selected for tumor classification and the scattered individual pixels were discarded. Final results from both MRI segmentation methods were transformed to the CT coordinate system using the transformation matrix produced by the registration software to allow comparison with the GTV outlines prepared by the radiation oncologists. Analysis strategy All analysis and image data transformation was performed using programs developed with Interactive Data Language software version 5.4 (IDL, Research Systems Inc., Boulder, CO). Intraoperator and interoperator variability. The intraoperator variability was calculated by overlapping the three Automated brain tumor volume determination volumes defined on the same patient by the same radiation oncologist at roughly 1-month intervals. The variability was then calculated as the ratio of the average disagreement; that is, the size of each volume minus the intersection of the three volumes, divided by the average size of the three volumes (see Appendix A). The interoperator variability was calculated using the nine sets of 3D resulting outlines for each of the 11 patients and then calculating the disagreement of each volume outline prepared by each physician for each patient with each volume outline prepared by each of the other two physicians for that same patient. This process was repeated for each patient to provide a data set comprising the average disagreement between the three contours for each patient prepared by one physician with the other six sets of contours prepared by the other two physicians for that same patient (see Appendix A). Accuracy. It is customary for radiation oncologists to delineate the GTV used in radiation therapy. The difference between brain GTV delineation for different physician specialties (radiation oncology, radiologists, neurosurgeons) has been reported by Weltens et al. (10). This research evaluates the automated segmentation methods as possible tools for delineating GTV in connection with treatment planning of brain tumor volumes. For purposes of this study, a probabilistic interpretation of the volumes delineated by the radiation oncologists provided the basis for evaluating the accuracy of both the individual physicians and the automated segmentation systems. Specifically, the probability that a given pixel in an image is properly classified as part of the tumor volume is determined by the number of times that this pixel was included in the nine outlines prepared by the three physicians. Every pixel in the image is labeled with an integer value (0 –9) corresponding to the number of physician contours in which it was included. This pixel label provided the weight for measuring accuracy. Final accuracy for the computer segmentation is then defined as the ratio of the total sum of weights contained within the computer segmentation volume to the total weights generated from the nine volumes produced by the physicians (Appendix B). The same protocol was used to determine the accuracy of each contoured volume produced by each physician. This approach measures the true-positive rate. To estimate the false-positive rate (i.e., the level of agreement between physicians on healthy tissue that was incorrectly characterized as constituting part of the GTV), the study calculated the excluded volume accuracy in an analogous manner (see Appendix B). RESULTS Image registration The CT and MR images were registered using the automatic registration function of the software. The radiation oncologist specializing in neuro-oncology reviewed each case and, if necessary, performed an additional manual adjustment. The same transformation matrix was used for ● G. P. MAZZARA et al. 303 comparing contours generated by the physicians with those produced by the segmentation methods, thereby eliminating any errors arising from the image registration. Operator time The time each radiation oncologist took to outline all 11 patients was recorded. It ranged from 4.0 to 6.5 hours in the aggregate (i.e., an average of approximately 30 min per patient). Physician 1 spent the most time outlining the patient contours, resulting in an average of approximately 30 min, whereas Physician 2 spent the least time, averaging approximately 20 min per patient. The time to perform a kNN segmentation averaged 20 min per patient, with some variation based upon the number of slices evidencing enhanced tumor and the difficulty of selecting the training data for the kNN segmentation algorithm. For the KG system, the only time required was in the preparation of the MRI scans for segmentation, which resulted in approximately 1.5 h of operator time. It is interesting to note that this data preparation task could be substantially automated in the future, further reducing the human operator time required by the KG system. The automatic segmentation using the KG system required approximately 30 min of computer time for all patients and required no user input. Manual outline variability Reproducibility of the delineation of the GTV on the MRI scans by the same radiation oncologist (intraoperator variability) was assessed producing the results set forth in Fig. 1 and Table 2. The intraoperator variability averaged 20% ⫾ 16% over all 33 contour sets of the 11 patients. The reproducibility of the delineation of target volume was generally better in preoperative cases (18 sets of contours: 15%) than in postoperative cases (15 sets of contours: 27%). The difference among GTVs identified by the three radiation oncologists (interoperator variability) was also assessed resulting in a total average of 28% ⫾ 12% (Fig. 2 and Table 2). The variability in the six preoperative cases was 24%, with a higher average ratio obtained for the postoperative cases (i.e., 32%). From Figs. 1 and 2, a large variation can be observed for Patient 6. This was a difficult case for both physicians and the automated systems. The MRI used was postoperative and the enhancement boundaries were not clear because of cystic formation inside the resected area (Fig. 3). Notice than even though there was a large variation for Patient 6, the median is close to the average and is within the standard deviation (see Table 2). Computer segmentations For the automated segmentation methods, it should be noted that the KG algorithm was not designed to evaluate nonenhancing tumors such as those encountered in connection with Patients 1 and 2. For Patients 3 and 6, the KG method identified tumors in very few of the slices that had physician outlines for tumor. Patient 6 had cystic formation 304 I. J. Radiation Oncology ● Biology ● Physics Volume 59, Number 1, 2004 Fig. 1. Graph of physician intraoperator variability for the 11 patients. inside a partly enhanced area so the margins were not clear (Fig. 3). Patient 3 had dentures and implants that caused artifacts in the images, making the KG automatic segmentation difficult (Fig. 4). In this case, there was also cystic formation inside the enhanced area. For both of these cases the kNN segmentation method performed within the contours produced by the physicians. The KG segmentation method performed poorly for sections of the tumor that were located in the lower part of the brain, which was the case for Patients 4 and 9, in whom the lower axial scans were not identified properly regardless of the enhancing property of the tumor (Fig. 5). For both of these patients, the KG missed the last slice of the enhancing tumor. Accuracy As described in the methods section and Appendix B, the results from the physicians were used as the basis for assessing the accuracy of the radiation oncologists and the MRI segmentation methods to determine GTV for radiation therapy brain 3D treatment planning. The results are tabu- lated in Table 3. The kNN method gave an average accuracy of 59% for preoperative scans compared with the 52% average obtained for postoperative scans. For the KG method, three of the preoperative cases were nonenhancing tumors or had cystic formation (i.e., Patients 1, 2, and 3) and were unable to be segmented. The average accuracy of the three physicians is 85% ⫾ 7%, compared with 56% ⫾ 6% for the kNN method and 52% ⫾ 7% for the KG method, resulting in a difference from the physicians’ contours of 29% and 33% for the kNN and KG method, respectively. Comparing this difference with the average interoperator variability of 28% ⫾ 12% for all 11 cases (with a range of variability between physicians from 17% to 60% [Fig. 2]), the automated segmentation methods are within the variability range of the physicians. It is important to note that the design of this study defined “true” volume by using the GTV generated by the same three radiation oncologists to whom the automated systems were compared; accordingly, it would not be possible within this conceptual framework for the accuracy of the automated systems to have exceeded that of their human Table 2. Intraoperator and interoperator variability* Intraoperator Variability Average Median Interoperator variability Average Median Physician 1 Physician 2 Physician 3 Average Volume (cm3) 13 ⫾ 5 13 26 ⫾ 19 22 22 ⫾ 23 15 20 ⫾ 16 16 63 ⫾ 33 61 Physician 1–2 Physician 1–3 Physician 2–3 Average Volume (cm3) 30 ⫾ 11 26 23 ⫾ 11 21 30 ⫾ 14 27 28 ⫾ 12 23 63 ⫾ 33 61 * Values shown are in percentages of total volume in cm3. Automated brain tumor volume determination ● G. P. MAZZARA et al. 305 Fig. 2. Graph of physician interoperator variability for the 11 patients. counterparts. This limitation of the study is explored further in the Future Work section. The accuracy measure used for this study favors larger volumes because there is no penalty in the measure for “false-positive” pixels. The effect of this false-positive effect is expressed as a ratio based on the volume included by the computer segmentations and excluded by the physicians’ modeling volume; these results are set forth in Table 4. Interestingly, the false-positive rate of the kNN method was 8% ⫾ 11% and of the KG method was 8 ⫾ 8%, whereas the false positive rate of the physicians was 17% ⫾ 11%. Thus the automated segmentation methods have been shown to err on the side of underestimation of tumor volume when compared with the physicians. The two segmentation methods were assessed visually and quantitatively to evaluate where the major volume differences occurred between the contours delineated by the physicians and the automated systems. This analysis should prove useful in suggesting further studies with larger sample sizes, which could significantly improve the accuracy of automated contouring systems for radiation oncology. In general, the largest variations between the contouring of the physicians as a group and those produced by the automated systems were found at superior and inferior edges of tumor. This effect can be seen clearly in Fig. 5, which shows enhancing tumor in the most inferior slice, which was not identified properly by the kNN method and that the KG method completely failed to detect. For slices in the central sections of tumors, both segmentation methods provided contours that were much closer to those created by human experts. Another example of this effects can be seen in Fig. 6, which shows the 3 superior slices for Patient 9 and contours drawn by the physicians in the top slice showing tumor. Images A through C demonstrate that the enhancement on image C has been included mainly because of the physicians’ knowledge that there is tumor in the previous slices at the corresponding locations. The kNN and KG segmentation methods are limited to two-dimensional identification protocols (i.e., each individual slice is analyzed for tumor without considering adjacent slices). The drawing of contour edges by human experts is a very subtle and subjective activity blending scientific training with heuristics developed through experience with a variety of tumors contoured over many years. Notice the variations in the contours among the physicians in this study. Interestingly for this case, one physician did not draw any GTV on a slice he marked as containing tumor the next two times he was faced with identical data. Figure 7 shows a 3D reconstruction of the tumor volume drawn by a physician (outer yellow volume) and the GTV estimated by the kNN (Fig. 7a) and the KG (Fig. 7b) systems. It can be seen clearly that the physician volume contains the GTV produced by the segmentation methods and that the segmentation methods fail to identify tumor most frequently in the superior and inferior edges of a tumor. In addition to the differences found at the superior and inferior edges of the tumor volume, the contours prepared by the segmentation systems agree with the physicians more at the center of the tumor than on the outside borders as shown in the example of contours in Fig. 8. Similarly, the areas where the physicians agreed most consistently (i.e., the regions where the pixels were included in at least seven of the nine physician outlines) were located near the center of the tumor. The corresponding accuracy for these areas of 306 I. J. Radiation Oncology ● Biology ● Physics Fig. 3. Magnetic resonance image of Patient 6 showing a gross tumor volume (GTV) contour from (a) Physician 1, (b) Physician 2, (c) Physician 3, and (d) supervised k-nearest neighbors (kNN) segmentation result. Notice the variability between all physician GTV contours and close agreement of kNN segmentation with Physician 1. The kNN performed well for a difficult case involving a cystic formation inside a partly enhanced area. Notice that all three physicians choose an area beyond the contrast enhancing area. This is due to information from previous image slice. The kNN method misses additional tumor volume because it does not use three-dimensional information (i.e., volume information from previous and following images). The magnetic resonance image shown is a T1-weighted axial scan after application of Gd contrast, field of view ⫽ 220, TR/TE ⫽ 400/8 ms, flip angle ⫽ 90. high physician agreement for kNN and KG was 75% and 72%, respectively. Figure 9 shows a section of the receiver operating characteristic (ROC) curves for all three physicians compared with those for the kNN and KG systems. The ROC curve is a plot of the true-positive rate (TP) against the false-positive rate (FP). It shows the tradeoff between sensitivity (portion of accurate TP) and specificity (portion of accurate truenegative) because any increase in sensitivity will be accompanied by a decrease in specificity. The closer a curve follows the left-hand border and top border of the ROC space, the more accurate the test. True tumor (TP) for this study is based on the times a pixel was included in an outline by the physicians. The curves for the segmentation methods must necessarily be below those of the physicians since the latter defined “truth” for purposes of this study. It can be seen that automated segmentation systems tend to fail in sensitivity but have a high degree of specificity as Volume 59, Number 1, 2004 Fig. 4. Magnetic resonance image of Patient 3 showing a small teeth artifact effect next to tumor containing Gd enhancement with nonenhancing cystic necrotic centers. Contours shown are gross tumor volume contours of (a) Physician 1, (b) Physician 2, (c) Physician 3, and (d) supervised k-nearest neighbors (kNN) segmentation method. The kNN method was able to segment this contour and obtain results close to the physicians’ outlines. The magnetic resonance image shown is a T1-weighted axial scan after application of Gd contrast, TR/TE ⫽ 400/8 ms, field of view ⫽ 220, flip angle ⫽ 90. evidenced by the data summarized in Tables 3 and 4 and Figs. 7 and 8. DISCUSSION The present study confirms published findings that variability in tumor contouring by human experts is high. Ten Haken and coworkers ran a simple test to assess the dosimetric consequences of imprecision in the definition of tumor volumes by a team of physicians when defining tumor volume in CT, MRI, and MRI-CT fused images finding that after two iterations of the contouring, the definition of tumor volumes were smaller and averaged just 75% of average physical volumes indicated in the first set of contours (7). Yamamoto and coworkers measured inter- and intraoperator variability that exceeded 10% for CT contoured areas of brain tumors (8). Another study reported very large interobserver variations in brain tumor delineation (range 9 –32%) for different physician specialties performing contours in both CT alone and CT with MRI (10). This error is larger that the setup variations and organ Automated brain tumor volume determination Fig. 5. Series of reconstructed magnetic resonance axial images for Patient 4 showing contours from Physician 1, supervised k-nearest neighbors (kNN), and knowledge-guided (KG) segmentation. Notice the excellent results for the middle slices for both automated segmentation methods and the failure of kNN and KG method for inferior slices where enhancement and tumor volume margins are not as clear and knowledge from previous slices is necessary to identify correct tumor volume. Slices shown are T1-weighted axial scans after application of Gd contrast, field of view ⫽ 220, flip angle ⫽ 90. Slices shown are 4-mm spaced. motions that are traditionally taken into account in radiation therapy planning. All of these results demonstrate the need for a method of contouring that is more consistently reproducible. In this study, it was found that the radiation oncologist who took the most time for outlining achieved the smallest intraoperator variability (i.e., 13% [the average for all of the oncologists was 20%]) and the one who took the least time ● G. P. MAZZARA et al. 307 in outlining produced the largest intraoperator variability, 26%. The variation between different radiation oncologists, or the interoperator variability, ranged from 11% to 69% with an average variability rate of 28%. These results mirror previously published results (8 –10) and show that there is significant uncertainty in target volumes definition even when such volumes are determined by a single radiation oncologist observing the same set of data on multiple occasions. The variability in delineation of GTV was about 10% larger in postoperative cases than in preoperative cases. Similarly, a larger variation was found for postoperative cases using the automatic segmentation methods. In postoperative cases, the margins of residual tumor are unclear making the identification of the GTV a difficult task for both physicians and automated segmentation systems. Previous studies confirm similar results (8, 9). The purpose of this study was to evaluate KG and kNN as potential cybercolleagues for radiation oncologists in determining tumor volume definition for treatment planning. We proposed a probabilistic measure of accuracy accounting for the inherent variability in operator judgment. It was found that even without any of the system enhancements suggested herein, the automated segmentation methods could qualify as independent experts because they perform within the large range of interoperator variability found among radiation oncologists. Several factors were identified to improve the accuracy of the segmentation methods to be used in radiation treatment planning. The greatest discrepancies between the contours produced by the automated segmentation methods and the physician’s was found at the edges superior or inferior of the tumor volume. For sections corresponding to the middle of the tumor volume, the kNN and KG method performed well (74% average) compared with the physicians. A greater difference at the superior and inferior borders Table 3. Accuracy of physicians and segmentation methods* Patient # 1 2 3 4 5 6 7 8 9 10 11 Average MRI type Pre Pre Pre Pre Post Post Pre Post Pre Post Post Average volume (cm3) Accuracy physician 1 Accuracy physician 2 Accuracy physician 3 Accuracy kNN method Accuracy KG method 28 90 98 40 108 73 100 63 36 17 39 63 ⫾ 33 86 92 92 86 86 71 89 84 74 79 91 84 ⫾ 7 87 82 95 92 90 63 94 88 91 87 89 87 ⫾ 9 89 94 91 89 91 57 88 89 78 88 86 85 ⫾ 10 57 67 62 58 62 52 57 51 52 48 46 56 ⫾ 6 n/a n/a n/a 48 50 n/a 63 54 43 60 48 52 ⫾ 7 * Values shown are in percentages of total volume in cm3. Abbreviations: MRI ⫽ magnetic resonance imaging; kNN ⫽ supervised k-nearest neighbors; KG ⫽ knowledge-guided; pre ⫽ presurgery MRI; post ⫽ postsurgery MRI. 308 I. J. Radiation Oncology ● Biology ● Physics Volume 59, Number 1, 2004 Table 4. Excluded accuracy for physicians and segmentation methods* Patient No. 1 2 3 4 5 6 7 8 9 10 11 Average MRI type Pre Pre Pre Pre Post Post Pre Post Pre Post Post Average volume (cm3) Exc acc physician 1 Exc acc physician 2 Exc acc physician 3 Exc acc kNN method Exc acc KG method 28 90 98 40 108 73 100 63 36 17 39 63 ⫾ 33 8 13 5 5 7 34 6 8 5 6 14 10 ⫾ 9 20 6 18 25 18 58 23 19 62 26 16 26 ⫾ 17 15 19 4 9 15 32 7 17 11 24 8 15 ⫾ 8 7 4 2 3 3 41 1 7 9 12 1 8 ⫾ 11 n/a n/a n/a 4 5 n/a 4 14 3 23 1 8⫾8 * Values shown are in percentages of total volume in cm3. Abbreviations: MRI ⫽ magnetic resonance imaging; exc acc ⫽ excluded accuracy; kNN ⫽ supervised k-nearest neighbors; KG ⫽ knowledge-guided; pre ⫽ presurgery MRI; post ⫽ postsurgery MRI. of the tumor results, at least in part, from the small enhancement found at the edges of the tumor. The drawing of contour edges is very subtle and subjective. The radiation oncologists use a 3D method of contouring; that is, one in which the previous and subsequent two-dimensional slices are used to predict the presence of tumor volume on the slide in question. This knowledge needs to be included in Fig. 6. Series of magnetic resonance axial images for Patient 9. (a), (b), and (c) show the top three slices of tumor, 4-mm spaced. Notice how (c) does not show too much enhancement, but by comparing it to previous images, some tumor volume can be seen. The tumor volume drawn the first time by each physician on the MR slice shown on (c) is shown in images (d), (e), and (f) for Physicians 1, 2, and 3, respectively. There is a large variation of contours between physicians. The segmentation methods did not identify tumor volume on (c). Slices shown are T1-weighted axial scans after application of Gd contrast, field of view ⫽ 220, TR/TE ⫽ 400/8 ms, flip angle ⫽ 90. the segmentation methods to improve accuracy (i.e., a 3D segmentation method is needed that uses knowledge and pixel information of tumor from adjacent two-dimensional slices). Compared with the kNN method, the KG method performed poorly for glioma cases that show Gd enhancement with nonenhancing cystic necrotic centers. The margins of the tumor are not clear for these cases and even the physicians’ contours show a larger intra- and interoperator variability for these cases. A possible solution for these cases is to use more knowledge from the T2 MRI images in the automatic segmentation cases. Additionally, the KG method failed to detect tumor volume located in the lower part of the brain. The KG system performs differently in different areas of the brain because it has rules describing the anatomy at the various levels through the brain. Anatomic structures are simpler in superior areas of the brain and increase in complexity toward inferior sections. The kNN method was able to give better results to these cases because there is some user input in selecting the initial tumor pixels and slices from which the kNN method began its segmentation analysis. The two cases that showed nonenhancing tumor volumes were not segmented by the KG method. It is necessary to incorporate automatic segmentation of nonenhancing brain tumors in the knowledge guided technique. Some promising work has been performed in developing an automatic method that separates nonenhancing brain tumors from healthy tissues in MRI images showing promising results (25). In summary, there is need for more work on the KG method to make it fully compatible for use in radiation therapy; this work would include modifications to permit contouring of partially enhancing tumors, resection cavities, and nonenhancing tumors. The guided kNN method performed better under these special circumstances because of its use of user input for initial selection of training pixel data. Automated brain tumor volume determination ● G. P. MAZZARA et al. 309 Fig. 8. Image shows axial slice with one contouring of Physicians 1, 2, and 3 (outer contours in red, orange, and pink, respectively), and supervised k-nearest neighbors segmentation (inner contour in blue), and knowledge-guidance segmentation (inner contour in light blue). Figure represents general effect encountered of decreasing agreement between the contours produced by the automatic segmentation methods and the physicians as compared from the center of the tumor toward its outside borders. Additionally, it demonstrates that computer segmentations tend to agree with the contours prepared by radiation oncologists when the radiation oncologists agree with each other. Fig. 7. Three-dimensional reconstructed images for Patient 11 showing contours of Physician 1 (outer volume in yellow) and supervised k-nearest neighbors (kNN) (inner red volume in (a)) and KG (inner red volume in (b)). The kNN and KG methods have a larger agreement with the physician toward the center of the tumor compared with the superior and inferior borders. The physician volume contains the segmented gross tumor volume (GTV). It can be noticed that the segmentation methods undersegment the GTV volume compared with that the radiation oncologist. Future work should concentrate on optimizing the segmentation techniques to improve the accuracy of their results, especially with respect to the definition of the inferior and superior borders of the tumor volume. Note that different glioma types were included in this research to generate the basis of possible future applications of brain segmentation methods. It would be of interest to perform more in-depth analysis on the variability of segmentation methods based on the type of brain tumors by selecting a specific type of tumor patients (glioblastoma, astrocytoma, or oligodendrogliomas) and study its tumor-specific segmentations results. Both segmentation methods considered herein should also be enhanced to allow them to identify edema and structures at risk. This would permit future incarnations of these automated systems to provide outlines for such structures and to assist physicians in automatic clinical target volume and PTV delineation. Additionally, the effects of creating radiation therapy treatment plans using PTV expanded volumes from computer-segmented GTV would provide valuable data for possible applications of these methods in actual clinical radiation therapy treatment. Additional research should also be performed that analyzes the results of the automated segmentation methods in a way that does not favor the physicians involved in the comparison. It was previously noted that the contours from the radiation oncologists used for comparison were also used to define the “true” volume. This posed a limitation in that the accuracy of the computer segmentation methods 310 I. J. Radiation Oncology ● Biology ● Physics Volume 59, Number 1, 2004 Fig. 9. Receiver operating characteristic curves for all three physicians compared with supervised k-nearest neighbors and knowledge-guidance. Computer segmentations fail in sensitivity but have a high rate of specificity; that is, most pixels identified are within the tumor volume defined by the physicians. would always fall below that of the physicians. A recent study recommends cooperation with a radiologist or neurosurgeon to reduce the variability in tumor volume definition (10). Incorporating a second group of physicians (preferably radiation oncologists, neurosurgeons, and radiologists) as experts working together to define “true” GTV based on their mutual consensus would allow subsequent studies to fairly compare the accuracy of automated segmentation systems with that of radiation oncologists evaluating the same data. CONCLUSIONS Radiation therapy treatment planning requires radiation oncologists to expend substantial time and effort contouring tumor target volumes for treatment. This study investigated the application of state-of-the-art automated tumor segmentation methods for brain MRI as a tool for tumor volume definition in radiation therapy treatment planning. Starting with the assumption that true target volume is found through the consensus of expert radiation oncologists, the study assessed the viability of computer segmentation methods as “cyber colleagues” of the human experts by measuring the accuracy and consistency of the automated system’s contouring. The results of this study demonstrate that the kNN and KG methods undersegment the tumor volume compared with the radiation oncologists but are within the variability of the contouring performed by experienced radiation oncologists based on the same data. At this time, the level of sophistication of the automated systems is insufficient for them to perform comparably to radiation oncologists. As automated systems improve, it is likely that their accuracy will approach that of human experts. Even in their current incarnation, the automated systems evaluated herein produced more consistent, though not more accurate, results than the physicians. Automatic tumor outlining has the potential to speed the contouring process in radiation treatment planning, produce a reproducible baseline for use by multiple physicians, and aid in multicenter trials because it would prevent physician- and centerbias that can affect trial outcomes. REFERENCES 1. Morris DE, Bourland JD, Rosenman JG, et al. Three-dimensional conformal radiation treatment planning and delivery for low- and intermediate-grade gliomas. Semin Radiat Oncol 2001;11:124–137. 2. Henkelman RM. New imaging technologies: Prospects for target definition. Int J Radiat Oncol Bio Phys 1991;22:251– 257. 3. Jansen EP, Dewit LG, Van Herk M, et al. Target volumes in radiotherapy for high-grade malignant glioma of the brain. Int J Radiat Oncol Biol Phys 2000;56:151–156. 4. Caudrelier JM, Vial S, Gibon D, et al. MRI definition of target volumes using fuzzy logic method for three-dimensional conformal radiation therapy. Int J Radiat Oncol Bio Phys 2003; 55:223–233. 5. Halperin EC, Bentel G, Heinz ER, et al. Radiation therapy treatment planning in supratentorial glioblastoma multiforme: an analysis based on post mortem topographic anatomy with CT correlations. Int J Radiat Oncol Biol Phys 1989;17:1347– 1350. 6. Seither RB, Jose B, Paris KJ, et al. Results of irradiation in patients with high-grade gliomas evaluated by magnetic resonance imaging. Am J Clin Oncol 1995;18:297–299. Automated brain tumor volume determination 7. TenHaken RK, Thornton AF, Sandler HM, et al. A quantitative assessment of the addition of MRI to CT-based, 3-D treatment planning of brain tumors. Radiother Oncol 1992;25: 121–133. 8. Yamamoto M, Nagata Y, Okajima K. Differences in target outline from CT scans of brain tumours using different methods and different observers. Radiother Oncol 1999;50:151– 156. 9. Khoo VS, Adams EJ, Saran F, et al. A comparison of clinical target volumes determined by CT and MRI for the radiotherapy planning of base of skull meningiomas. Int J Radiat Oncol Biol Phys 2000;46:1309–1317. 10. Weltens C, Menten J, Feron M, et al. Interobserver variations in gross tumor volume delineation of brain tumors on computed tomography and impact of magnetic resonance imaging. Radiother Oncol 2001;60:49–59. 11. Pitkanen MA, Holli KA, Ojala AT, et al. Quality assurance in radiotherapy of breast cancer—variability in planning target volume delineation. Acta Oncol 2001;40:50–55. 12. Van den Berge DL, De Ridder M, Storme G. Imaging in radiotherapy. Eur J Radiol 2000;34:41–48. 13. Clarke LP, Velthuizen RP, Camacho MA, et al. MRI segmentation: Methods and applications. Magn Reson Imaging 1995; 13:343–368. 14. Vaidyanathan M, Clarke LP, Velthuizen RP, et al. Comparison of supervised MRI segmentation methods for tumor volume determination during therapy. Magn Reson Imaging 1995;13:719–728. 15. Vaidyanathan M, Clarke LP, Hall LO, et al. Monitoring brain tumor response to therapy using MRI segmentation. Magn Reson Imaging 1997;15:323–334. 16. Li C, Goldgof DB, Hall LO. Automatic segmentation and tissue labeling of MR images. IEEE Trans Med Imaging 1993;12:740–750. ● G. P. MAZZARA et al. 311 17. Clark MC, Hall LO, Goldgof DB, et al. Automatic tumor segmentation using knowledge-based techniques. IEEE Trans Med Imaging 1998;17:187–201. 18. Velthuizen RP, Clarke LP, Phuphanich S, et al. Unsupervised measurement of brain tumor volume on MR images. J Magn Reson Imaging 1995;5:594–605. 19. Meyer CR, Boes JL, Kim B, et al. Demonstration of accuracy and clinical versatility of mutual information for automatic multimodality image fusion using affine and thin-plate spline warped geometric deformations. Med Image Anal 1997;1: 195–206. 20. Maes F, Vandermeulen D, Suetens P. Comparative evaluation of multiresolution optimization strategies for multimodality image registration by maximixation of mutual information. Med Image Anal 1999;3:373–386. 21. Grossman SA, O’Neill A, Grunnet M, et al. Phase III study comparing three cycles of infusional carmustine and cisplatin followed by radiation therapy with radiation therapy and concurrent carmustine in patients with newly diagnosed supratentorial glioblastoma multiforme: Eastern Cooperative Oncology Group Trial 2394. J Clin Oncol 2003;21:1485–1491. 22. Kleinberg L, Grossman SA, Carson K, et al. Survival of patients with newly diagnosed glioblastoma multiforme treated with RSR13 and radiotherapy: Results of a phase II new approaches to brain tumor therapy CNS consortium safety and efficacy study. J Clin Oncol 2002;20:3149–3155. 23. Clarke LP, Velthuizen RP, Phuphanich S, et al. MRI: Stability of three supervised segmentation techniques. Magn Reson Imaging 1993;11:95–106. 24. Clarke LP, Velthuizen RP, Clark MC, et al. MRI measurement of brain tumor response: Comparison of visual metric and automatic segmentation. Magn Reson Imaging 1998;16:271– 279. 25. Fletcher-Heath LM, Hall LO, Goldgof DB, et al. Automatic segmentation of non-enhancing brain tumors in magnetic resonance image. Artif Intell Med 2001;21:43–63. APPENDIX A Intraoperator and interoperator variability The intraoperator variability was calculated as the ratio of the average disagreement; that is, the size of each volume minus the intersection of the three volumes, divided by the average size of the three volumes. For example, if a radiation oncologist had identified the same target volume in the three sets of contours prepared for any single patient, then the variability for that patient would have been zero. The definition of intraoperator variability is represented in Fig. A: Vi1, Vi2, and Vi3 indicate tumor volume delineated by the radiation oncologist i three times and shaded area Vi(int) represents the intersection of all three volumes. This results in the following formula to calculate the intraoperator variability: 冘 3 COV intra i ⫽ 1 共V ⫺ V i共int兲兲 3 j⫽1 ij 冘 3 *100% 1 V 3 j⫽1 ij Fig. A. The interoperator variability was calculated using the nine sets of outlines for each of the 11 patients and then calculating the disagreement from the outline prepared by each physician for each patient with the corresponding outline prepared by each of the other two physicians for that same patient. Figure B shows the disagreement of one volume of one physician i (Vi1) with one volume of another physician j (Vj1): 312 I. J. Radiation Oncology ● Biology ● Physics Volume 59, Number 1, 2004 COV Fig. B. The final intraoperator variability is the average of the comparison of all volumes of one physician with all the volumes of the other physician as shown in the following formula: inter ij 1 ⫽ 9 冘 冘 VV 3 3 m⫽1 n⫽1 ⫺ V jn *100% im ⫹ V jn im This is done for each of the three physicians, resulting in the average variability between the three contours for each patient prepared by one physician with the other six sets of contours prepared by the other two physicians for that same patient. The greater the difference between the contours of different physicians, the larger this ratio becomes. APPENDIX B Calculation of accuracy Accuracy was calculated by assuming that the probability that a region is part of the definition of gross tumor volume is reflected by the number of times that region is included in any of the nine outline volumes produced by the three radiation oncologists. Every pixel in the image volume is labeled with an integer value corresponding to the number of physician contours in which it was included (e.g., if a pixel was never included in any physician outline, its corresponding value would be zero, whereas a pixel included in every physician outline would have a value of nine). The resulting composite physician GTV comprises pixels labeled with values from zero to nine that define the probability of finding tumor volume. The pixel label provided the weight for measuring accuracy. This analysis was done on a pixel-by-pixel basis. Thus the degree of accuracy associated with a failure to classify a pixel as being part of a tumor volume would decrease in proportion to the weight associated with that pixel. For example, the failure to include a pixel that was assigned a label of nine would reduce accuracy more than missing a pixel that was assigned a level of one (i.e., a pixel selected only once by the physicians). Figure C shows a single volume of either physician (Vij) or segmentation (Vk) compared with three (out of the nine) physician volumes. An area of higher pixel label weight is represented by level of gray in the figure (i.e., the area where the single volume being evaluated intersects more physician contours): Final accuracy or true-positive is then expressed as the ratio of the total sum of pixel weights that was included by the physician or segmentation volume (Vij or Vk, showed as shaded areas in previous figure) to the total sum of pixel weights of the nine volumes produced by the physicians (represented by all area enclosed by the three volumes Vi1, Vi2, and Vi3 in Fig. C): 冘 Accuracy 共Vij or Vk兲 ⫽ image pixels 1 9 i⫽1 3 ij j⫽1 *100% 冘 冘冘 3 3 1 V ij 9 image pixels i⫽1 j⫽1 Similarly, excluded accuracy or false-positive is expressed as: Exc. Accuracy 共Vij or Vk兲 冘 ⫽ Fig. C. 冘 冘V 3 共V ij or V k兲* 冉 冘冘 3 3 冊 1 共V ij or V k兲* 1 ⫺ V ij 9 image pixels i⫽1 j⫽1 冉 冘 冘冘 3 3 冊 1 1⫺ V ij 9 image pixels i⫽1 j⫽1 *100%