Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
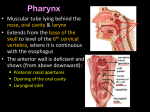
Paulman Test 2 Review 2 Pharynx 6 muscles of the Pharynx 3 Constrictors Superior constrictor Pharyngeal tubercle on skull is proximal attachment levator veli palantini above it, CN 9, and sylopharyngeous come out at this point Middle constrictor hyoid and pharyngeal raphe attachments Superior laryngeal nerve and arter (comes from external carotid artery this is the landmark between middle and inferior constrictor External carotid branches know them Inferior constrictor thyro and crico cartilages and pharyngeal raphe Recurrent laryngeal inserts below… KNOW! And know that slide 3 longitudinal all attach to posterior part of thyroid cartilage Stylopharyngeous 9 (sensory and motor) Salpingopharyngeous superior attachment at turous tuberious (makes hole around internal auditory tube) 9 sensory and 10 motor Palatopharyngeous lateral side of soft palate, shortens pharynx for phonation and swallowing 9 and 10 Lateral and inferior to crico cartilage piriform recess the recurrent laryngeal nerve is in there** Naso, oro, laryngo Pharyngeal recess it is where the pharyngeal tonsil is found (part of Waldeyer’s ring palatine and lingual tonsils complete ringtubal tonsils too) Larynx Muscles named for what they attach to Recurrent laryngeal branch of vagus supplies all moror of laryngeal muscles EXCEPT cricothyroid (innervated by external branch of superior thyroid) Sensory of larynx Internal branch of superior thyroid Thyroarytenoid jt partial synovial posteriorly and acts as pure ligamentous attachment anteriorly Vocal fold medial to lateral Mucosa Vocal ligament Vocalis muscle unique bc it tenses and loosens (deepens pitch) vocal ligament at same time bc of multiple attachments; crycothyroid (gives you really deep pitch) Thyroarytenoid (most lateral and largest) Pharynx surrounds entire larynx Mucosa, submucosa, muscular layer, two layers of fascia Nasal Cavity Palate innervated by Greater and Lesser palatine nerves (hard and soft) Ethmoid ant and posterior from V1 tip of nose***Test question V2 nasopalantine nerve, greater and lesser palatine, and lateral nasal nerves Olfactory epithelium innervated by CN 1! Kisselbach area 90% of nose bleeds happen here at septum because there’s like 4-5 arteries supplying nasal cavity Put pressure on palate to stop Greater palatine artery form bleeding bc it’s the biggest artery there in nose. Concha mucosal underlying bones called turbinates (superior and middle ethmoid bone and inferior its own bone) Meatuses particular things open here Inferior choncha nasal lacrimal duct (corner of eye down nose) Middle meatus BUSY semilunar hiatus (3 sinuses open up here! frontal , maxillary, and anterior ethmoids) There’s a bulge called ethmoid bulla openings that the middle ethmoidal air cells drain Posterior ethmoids Superior meatus Sphenoethmoidal recess the canal before the ostia of sphenoidal sinus Sphenoid sinus important bc it’s surrounds the hypophyseal fossa where cavernous sinus is!!! Sinuses Frontal sits by nasal cavity and between two orbits thin bone Ethmoid sinus sits medial to orbits anterior and medial sit next to lamin parpricia which IS VERY THIN! someone with ethmoid injury tend to be cross-eyed Sphenoid you can die if you have problems here because internal carotid is here cavernouse sinus here (III-VI and II is nearby) Maxillary sinus orbit and teeth issues V2 passes by roof of orbit which is roof of maxillary sinus eye and upper teeth issues Oral Cavity Tongue 8 pairs Intrinsic muscles change shape of the tongue CN XII Extrinsic muscles change position of the tongue most innervated by XII but palatoglossus innervated by CN X Genioglossus mental spine of mandible and distal attachment is none PROTRUDES Hyoglossus hyoid bone XII retracts and depresses tongue Palatoglossus last muscle you use to swallow pulls bolus up and back CN X Styloglossus distal attachments (also attaches to hyoglossus) pulls strait back (significantly ELEVATES) important in licking ice cream? Sensory (somatic and visceral) General sensory to anterior 2/3 CN V3 via lingual nerve Taste to anterior 2/3 CN VII chorda typani Copula comes from arch 2 so it goes through apoptosis and there is only chorda typani Posterior part of tongue CN 9 and 10 CN 10 both sensory and motor 5 nerves with tongue 5, 7, 9, 10, 12 Vertical opening with two openings isthmus of faucial opening from oral cavity to pharynx Space between palatoglossus and palate palatine recess palantine tonsils pharyngeal pouch 2! Arterial supply LINGUAL ARTERY 2nd anterior branch of external carotid artery anterior to mandible medial to hyoglossus muscle gives off dorsal lingual artery deep lingual and sublingual artery Greater and lesser palatine arteries supply palate Facial artery supplies cheek Venous drainage follows artery pattern Gingiva ectoderm meets endoderm (with no mesoderm) Teeth 2- incisors, 1 canine, 2 premolars, 3 molars (# of cusps differentiates molars) Cases 1. Patient comes in with a pen lodged through her mouth. It went into the floor of the right side of mouth. Name everything that passes through. Mucosa Hyoglossus muscle (hypoglossal nerve… maybe lingual), Lingual artery/vein which comes from external carotid Geniohyoid (worry about the C1 because it runs with hypoglossal nerve) C1 worry about infrahyoid muscles Mylohyoid muscle (nerve comes in anteriorly so you will probably miss the nerve) Anterior belly of digastric Suprahyoid and digastic you only use them to open up mouth against resistance Can hit submandibular salivary gland Investing fascia Platysma CN VII Sub Q Skin Can lose a lot of motor innervation on that side 2. Patient who works in a circus as sticking nails up his nose. One day his heart was cold (?) and his head would pound; he felt lethargic. When he pulled nail out, he noticed his blood wasn’t as thick as usual, and then he has clear fluid, and had the worst headache of his life. He is leaking CSF so he penetrated his skull somewhere sella turcia, hypophseal fossa punched hole into PITUITARY GLAND it regulates metabolism so Damage here leads to DEATH 3. 2 year old child who isn’t speaking yet so parents are worried. On examination, you take a laryngoscope, and you look at vocal fords they are intact but there is no bulge on posterior part of vocal cords vocal folds don’t move no matter how much you stimulate them rima glottides stays the same. What pharyngeal arch of neural crest cells is involved? Neural crest are involved in cartilage. Pharyngeal arch 4 no arytenoid cartilages!!! 4. Gunshot wound to RIGHT LATERAL NECK. Bullet passes superior to lamina of thyroid cartiliage, through pharynx, then lodged in LEFT PHARYNGEAL WALL. Is this dangerous? Carotid artery is that level so you can severe this!!! Internal jugular vein that could be hit you would be ok if this is hit Superior thyroid artery can get nicked Superior laryngeal artery and superior laryngeal nerve (so you kill artery supply to larynx and much of pharynx) Lungs 5. Patient who has lymphadenopathy and is complaining of dyspnea. When you listen to lungs, you can hear air; air way is fine. So you decide to do thoracotomy to figure out what is going on. You notice the left lung is dark, spongy fluidy, and the biopsy shows necrotic tissue. What happened? Damaged hilum and compressed bronchial artery which isn’t giving oxygenated tissue to the lung (pulmonary artery is fine but bronchial supplies the lung itself). 6. Patient whom smokes has squamous cell tumor on his lip that has gone through gingiva and gone to molars then into alveolars of mandible and into the root of the tongue. In terms of metastasis, what is the likely route from oral cavity to lung? Floor of mouth goes to superficial lymphatic channels (collar nodes- anterior ones biggest is jugulardigastric node) then jugularomohyoid node left thoracic trunk node thoracic duct superior vena cava then you are in venous system so you go through heart so you can get into the LUNGS either lung 7. Patient has chronic sinusitis. You always give him antihistamine, and last time you gave him Vancomyocin. Now, he complains that his mucosa is slimy then fell off when you look, you can see the right side of the hard palate is bone (mucosa is dead). Patient also says the same thing is happening in his nose, tissue being eaten away at septum. What is your next step? Chronic sinusitis can lead to bone deterioration and abscesses there is lack of blood supply Greater and lesser palatine arteries are destroyed because they are on palate and nasal cavity so do a CT of the head and look for abscess CT shows large abscess from maxillary sinus to posterior part of nasal wall destroyed you greater and lesser palatine nerves graph the arteries If it doesn’t get fixed, he will have bacteremia, septicemia, and a lot of pain. GREATER PALATINE ARTERY main artery supplying Kelselbox area. Lots of EPITAXIS! 8. Patient presents with impacted wisdom tooth that isn’t able to come out. When you take an X-ray, you notice the root of tooth has passed up the lateral wall of maxillary sinus and is imbedded in roof of maxillary sinus. Roof of maxillary is floor of the orbit so you would have connected the two air passes in and out orbit is exposed to bacteria which could lead to blindness (ophthalmic artery and optic nerve) also internal carotid artery there.