Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
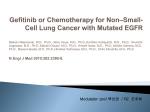
Int J Clin Exp Med 2016;9(9):18360-18366 www.ijcem.com /ISSN:1940-5901/IJCEM0028938 Original Article The efficacy and safety of lcotinib in patients with advanced non-small cell lung cancer: compare with gefitinib Zhe Zhang1, Qiming Wang1, Hong Tang1, Suhua Xia2, Zelai He3, Zhen He1, Lili Wang1, Hui Zhu1, Shaomei Li1, Yufeng Wu1 Department of Internal Medicine, Affiliated Cancer Hospital of Zhengzhou University, Henan Cancer Hospital, Zhengzhou 450008, Henan, PR China; 2Suzhou University, Suzhou 215000, Jiangsu, PR China; 3The 2nd Affiliated Hospital & Yuying Children’s Hospital of Wenzhou Medical University, Wenzhou 325000, Zhejiang, PR China 1 Received March 23, 2016; Accepted August 14, 2016; Epub September 15, 2016; Published September 30, 2016 Abstract: Background: As is known to all, non-small-cell lung cancer (NSCLC) is one of the most lethal malignancies with few effective treatment modalities. Epidermal growth factor receptor tyrosine kinase inhibitors (EGFR-TKIs) are very effective for treating the patients with EGFR mutations. As the first homegrown anticancer drug, icotinib is a novel, orally administered, and reversible EGFR-TKI. This study aimed to compare the efficacy and safety of icotinib with gefitinib to patients with advanced NSCLC. Methods: The retrospective analysis included 219 patients with stage IIIB/IV NSCLC harbouring mutant-type EGFR. The selected patients received either icotinib (125 mg thrice daily, n=126) or gefitinib (250 mg daily, n=93) orally until the disease progression or unacceptable toxicities appeared. Meanwhile, side effects, tumor responses, progression-free survival (PFS) and overall survival time (OS) were recorded for analysis. Results: Compared with gefitinib, it was observed that the overall objective response rate of patients was 46.0% and the disease control rate was 86.5%. The life quality of patients was improved accordingly. The main toxicities of icotinib were skin toxicity (rash) and diarrhea. A total of 4 patients were found with moderate adverse reactions, which was lower than gefitinib. The median PFS was 6.5 months in the icotinib group and 6.3 months in the gefitinib group, and the OS was 20.9 months in the icotinib group and 20.3 months in the gefitinib group. Conclusion: Associated with a lower number of treatment-related adverse cases than gefitinib, icotinib was not inferior to gefitinib in treating advanced NSCLC. In conclusion, China’s homemade EGFR-TKI, icotinib has provided a new choice for NSCLC patients. Keywords: NSCLC, EGFR-TKIs, icotinib, gefitinib, adverse reactions Introduction Featured with better efficacy and lighter adverse reactions, epidermal growth factor receptor tyrosine kinase inhibitors (EGFR-TKIs) have been increasingly applied as maintenance therapy for patients with advanced non-smallcell lung cancer (NSCLC) [1, 2]. EGFR mutations are more common in Asian people (40-50%) than European (10%), especially in a subset of patients like non-smoking Asian women with adenocarcinoma [3]. Therefore, EGFR-TKIs, such as gefitinib and erlotinib, is particularly beneficial for Asian population [4, 5]. As the first homegrown EGFR-TKI drug designed, synthesized, and screened by Zhejiang Beida Pharmaceutical Co. Ltd (Zhejiang, China), icotinib is with independent intellectual property rights [6]. Although the full pharmacokinetic parameter profiles of icotinib have been published [7], further studies are needed to investigate the efficacy and safety of icotinib compared with other EGFR-TKIs like gefitinib. In current study, by analyzing the data of patients with advanced NSCLC who were treated in Henan Cancer Hospital from June 2011 to November 2014, this study evaluated the efficacy and safety of icotinib in patients with advanced NSCLC. Therefore, this study can be of important reference for further clinical medication. The efficacy and safety of icotinib in patients with non-small cell lung cancer Patients and methods Patients The selected patients had histologically confirmed as stage IIIB or stage IV with the American Joint Committee on Cancer [AJCC] 6th edition of tumor-node-metastasis [TNM] staging system. Moreover, they were diagnosed with NSCLC accompanying with EGFR-mutant, and their disease progression was at least one period of platinum-based chemotherapy. Other selection criteria included: age from 18 to 75; Eastern Cooperative Oncology Group (ECOG); performance status (PS) 0-2; at least one measurable lesion by the Response Evaluation Criteria in Solid Tumors version 1.1 (RECIST 1.1); adequate hematologic and biochemical values; and without receiving other antineoplastic therapy during the application of icotinib or gefitinib treatment. In addition, patients would be excluded if they received any previous human EGFR-TKIs or other molecular target drugs or if they had serious or severe hypersensitivity reactions to icotinib hydrochloride or any of its excipients. Other excluded criteria contain: symptomatic brain metastases; malignant tumor within the last five years; severe infection; congestive heart failure; previous treatment with drugs targeting EGFR; and a history of interstitial lung disease. RECIST 1.1, the tumor response assessment was divided into complete response (CR), partial response (PR), stable disease (SD), progressive disease (PD), while the objective response rate (ORR) was defined as the sum of CR and PR, and the disease control rate (DCR) was defined as the sum of CR, PR and SD. Meanwhile, the toxic effects were monitored and graded based on the National Cancer Institute Common Toxicity Criteria for Adverse Events version 3.0 (CTCAE 3.0). Statistical analysis The analysis of this study was performed by SPSS version 17.0 software (SPSS Inc., Chicago, IL, USA). The safety and toxicity was analyzed with a descriptive statistical method in the safety set. Frequency and percentage were used to describe the categorical data. The mean, standard deviation, median, minimum and maximum were utilized to illustrate the measurement data. Besides, χ2 test was applied to compare the total incidence and the major adverse events between different groups. The Kaplan-Meier curve was performed to estimate the median for PFS and OS and draw the survival curves. The threshold of P<0.05 was defined as statistically significant. Results Methods Demographic data Patients in icotinib group received 125 mg oral icotinib in tablet form three times per day while those in gefitinib group received 250 mg gefitinib in tablet form once daily, until they reach the required disease progression or unacceptable toxicity. Side effects and tumor response of the treatment were observed, including clinical symptoms, progression-free survival (PFS) and overall survival time (OS). Between June 2011 and November 2014, a total of 128 patients were enrolled in icotinib group, in which 126 were evaluated for the efficacy and safety analysis (while 2 cases failed to complete the experiment due to severe adverse reactions). A total of 93 patients were in Gefitinib group. Compared with the demographic situation of patients in two groups, the chi-square test indicated that there was no significant difference in gender, age, ECOG PS, smoking history, BMI, pathological typing and clinical staging of the two groups (P>0.05). The specific information of two groups was shown in Table 1. Response evaluation Every enrolled patient must include symptom evaluation one week before enrollment and four weeks after receiving icotinib or gefitinib. The detailed evaluation criteria included ECOG PS, eating and sleeping, choking sensation in chest, pectoralgia, coughing, breathing difficulties, blood in sputum and other symptoms, as well as rash, diarrhea, fatigue, lack of appetite, nausea and other side effects. According to 18361 Symptom and quality of life (QoL) This study evaluated the clinical symptoms and the life quality of the patients. The results suggested that the clinical symptoms of patients were eased significantly after receiving EGFR- Int J Clin Exp Med 2016;9(9):18360-18366 The efficacy and safety of icotinib in patients with non-small cell lung cancer Table 1. Baseline patient characteristics in Icotinib and Gefitinib groups Icotinib N=126 N (%) Gefitinib N=93 N (%) Gender Male 34 (27.0) 29 (31.2) Female 92 (73.0) 64 (68.8) Age >70 years 41 (32.5) 33 (35.5) ≤70 years 85 (67.5) 60 (64.5) Smoking status Smoker 29 (23.0) 19 (20.4) Non-somker 97 (77.0) 74 (79.6) ECOG PS 0 or 1 107 (84.9) 85 (91.4) ≥2 19 (15.0) 8 (8.6) Stage III B 9 (7.14) 6 (6.5) IV 117 (92.9) 87 (93.5) Histology Adenocarcinoma 118 (93.7) 90 (96.8) Non-Adenocarcinoma 8 (6.3) 3 (3.2) 2 BMI (kg/m ) 23.91 ± 0.3092 24.26 ± 0.3911 χ2 P-value 0.28 0.5979 0.10 0.7559 0.14 0.7088 1.52 0.2175 0.00 0.9438 0.54 0.4635 0.2694 Table 2. Symptoms and QoL Symptoms Chest congestion Ache Cough Eating and sleeping Onset time (day) Remission rate (%) Icotinib Gefitinib 74.2 80.3 43.3 49.1 66.8 65.2 53.5 37.5 7.633 ± 0.2152 8.101 ± 0.3213 χ2 P-value 0.71 0.50 0.02 4.53 0.4008 0.4781 0.8813 0.0333* 0.2694 χ2 0.00 0.13 2.58 0.00 4.55 P-value 0.9601 0.7184 0.1084 0.9925 0.0328* *, P<0.05. Table 3. Response evaluation Response evaluation CR PR SD ORR (CR+PR) DCR (CR+PR+SD) Icotinib N (%) 14 (11.1) 44 (34.9) 51 (40.5) 58 (53.2) 109 (86.5) Gefitinib N (%) 11 (12.3) 31 (33.8) 27 (28.5) 42 (45.2) 69 (74.2) *, P<0.05. TKI. In terms of loosening chest congestion, icotinib group was slightly less effective than gefitinib group (74.2% v.s. 80.3%), but there was no significant difference between the two groups (P=0.4008), and the difference in ache 18362 (43.3% v.s. 49.1%, P=0.4781) and cough (66.8% v.s. 65.2%, P=0.8813) was also not significant in both groups. Nevertheless, the subjective symptoms of eating and sleeping which were easier to be influenced by the subjective feelings of patients were improved better in the icotinib group than gefitinib group (53.5% v.s. 37.5%, P=0.0333) with statistical significance. The onset time of icotinib group was slightly less than that of gefitinib group (7.633 ± 0.2152 v.s. 8.101 ± 0.3213), but there was no significant difference between the two groups (P=0.2694), as shown in the Table 2. Response evaluation CR has no significant difference between icotinib group and gefitinib group (14 of 126 patients v.s. 11 of 93 patients, P=0.9601). Meanwhile, the number of patients in PR, SD and PD also has no significant difference (icotinib group 44, 51, 17 v.s. gefitinib group 31, 27, 24, P> 0.05). In this regard, the ORR of icotinib was no better than gefitinib (53.2% v.s. 45.2%, P=0.9925). However, this study found that the DCR of icotinib group was much higher than that of Gefitniib group (86.5% v.s. 74.2%, P=0.0328), as shown in the Table 3. Adverse reactions As shown in Table 4, 112 patients in the icotinib group presented the grade 1-3 rashes on their skin 10-20 days later after taking icotinib; 11 patients suffered the grade 1-3 diarrhea; and 3 patients showed the grade 1-2 liver damage. In gefitinib group, 85 patients presented the grade 1-3 rashes on their skin Int J Clin Exp Med 2016;9(9):18360-18366 The efficacy and safety of icotinib in patients with non-small cell lung cancer Table 4. Adverse reactions Adverse reactions Rash Diarrhea Liver damage Icotinib 1-2 (%) 3 (%) 109 (86.5) 3 (2.4) 10 (7.9) 1 (0.8) 3 (2.4) 0 (0) 4 (%) 0 (0) 0 (0) 0 (0) Gefitinib 1-2 (%) 3 (%) 82 (88.2) 3 (3.1) 6 (6.5) 1 (1.1) 1 (1.1) 0 (0) 4 (%) 0 (0) 0 (0) 0 (0) χ2 P-value 2.09 0.01 0.04 0.1487 0.9429 0.8393 Figure 1. The PFS and OS of icotinib group and gefitinib group. A. The PFS of icotinib group and gefitinib group. B. The OS of icotinib group and gefitinib group. after receiving getitinib; 7 patients suffered the grade 1-3 diarrhea, and 1 patient showed the grade 1-2 liver damage. Therefore, it can be concluded that the patients in two groups show mild adverse reactions, and the symptoms have been controlled after giving the antidiarrheic and hepatoprotective therapy. Only two patients presented the grade 3 adverse reactions. They were allowed to stop taking icotinib for a while, and to take drugs for the treatment of adverse reactions until the symptom was controlled. No more moderate adverse reactions occurred after continuing the application of icotinib. According to the Kaplan-Meier analysis, the PFS and the OS did not significantly differ between the two treatment groups. The median PFS was 6.5 months in the icotinib group and 6.3 months in the gefitinib group (Figure 1A), and the OS was 20.9 months in the icotinib group and 20.3 months in the gefitinib group (Figure 1B). The PFS and OS had no significant difference in the two groups (P>0.05). Discussion As a leading cause of the cancer-related mortality both in China and abroad, lung cancer is a 18363 serious threat to the health of most people [8-10]. Unfortunately, more than 80% of NSCLC cases are diagnosed in advanced stage (IIIB or IV). At that stage, the systemic chemotherapy remains the standard care but provides marginal improvement in survival, resulting in poor prognosis with a median survival of only 10 months or so [6, 11]. The targeted therapy is one of the main treatments for patients with NSCLC [12]. As a novel, orally administered, and reversible EGFR-TKI, icotinib is the first homegrown anticancer drug [13]. As the previous studies mainly focused on prolonging the survival time [14], few researchers analyzed the life quality of patients. Icotinib was not inferior to gefitinib in terms of progression free survival and overall survival [15]. This study aimed to compare the efficacy and safety of icotinib with gefitinib on patients with advanced nonsmall cell lung cancer. Hence, this study provides reference and basis for clinical application for patients with advanced NSCLC. The abnormal activity of EGFR was mainly caused by the mutation. According to the state of EGFR, the NSCLC was divided into mutant type and wild type [8, 16]. It was observed that the binding capacity of ATP was decreased after EGFR mutation, but the affinity of gefitinib Int J Clin Exp Med 2016;9(9):18360-18366 The efficacy and safety of icotinib in patients with non-small cell lung cancer was enhanced. It indicated that EGFR-TKIs could competitively inhibit the ATP’s binding to the intracellular areas of EGFR and block its signaling pathway so as to achieve the antitumor effect [17, 18]. Considering that the wildtype EGFR has a high affinity with ATP and a low affinity with EGFR-TKIs, it will not affect the function of the wild type EGFR or produce the anti-tumor effect [16, 19]. According to recent analysis, about 35% of patients in East Asia were diagnosed as nonsmall cell lung cancer with EGFR mutations [20]. As the first EGFR TKIs, gefitinib and eriotinib were introduced for clinical application. As patients with EGFR activating mutations are notably sensitive to EGFR-TKIs, gefitinib and eriotinib show great curative effects in the treatment of EGFR-mutated NSCLC. Moreover, they not only improve the survival time of patients, but also greatly improve their quality of life [21, 22]. Icotinib is the first EGFR-TKI with proprietary intellectual property rights in China and the third commercially available EGFR-TKI in the globe [23, 24]. As a randomized, double-blind, head to head, and phase III trial, ICOGEN is designed to determine whether icotinib is similar to gefitinib in patients with locally advanced or metastatic NSCLC. This study proves that icotinib is not inferior to gefitinib in terms of efficacy and it shows a better safety profile when compared to gefitinb [6, 7]. Made in China, icotinib has an obvious price advantage compared with the imported drugs, which can further reduce the treatment-related costs while promoting the development of Chinese pharmaceutical industry. Therefore, Icotinib has the potential to become a standard treatment for NSCLC population with EGFR mutations. The most frequent treatment-related adverse reactions were rash and diarrhea. Most adverse reactions were mild to moderate (grade 1/2), and very few patients suffered serious adverse reactions [15, 21]. Hence, this study further confirmed that there was no difference in terms of safety between icotinib and gefitinib. As a retrospective study, this study has several limitations. First of all, the sample size is too small, with only 126 patients. A higher proportion of patients and more clinical trials are needed in the future. To sum up, icotinib is one of effective EGFR-TKIs for pretreating NSCLC population with favorable antitumor activity. Furthe- 18364 rmore, this study further confirmed that it was clinically equivalent to gefitinib in previously treated patients with NSCLC. Featured with superior tolerability, safety and efficacy on patients with NSCLC, icotinib is of great significance in improving the survival time and life quality of patients. Hence, it is worthwhile to spread icotinib in clinical therapy. Acknowledgements This work was partly supported by Doctoral Program Foundation of Henan Cancer Hospital awarded to Yufeng Wu (No. 201511004). Disclosure of conflict of interest None. Address correspondence to: Dr. Yufeng Wu, Department of Internal Medicine, Henan Cancer Hospital, No. 127 Dongming Road, Zhengzhou 450008, PR China. Tel: (86)18695829280; Fax: (86)0371-65588134; E-mail: [email protected] References [1] [2] [3] [4] Shi Y, Sun Y, Ding C, Wang Z, Wang C, Wang Z, Bai C, Bai C, Feng J, Liu X, Li F, Yang Y, Shu Y, Wu M, He J, Zhang Y, Zhang S, Chen G, Luo H, Luo R, Zhou C, Zhou Y, Pang Q, Zhao H, Zhao Q, Gu A, Ling Y, Huang C, Han B, Jiao S and Jiao H. China experts consensus on icotinib for nonsmall cell lung cancer treatment (2015 version). Ann Transl Med 2015; 3: 260. Feng S, Wang Y, Cai K, Wu H, Xiong G, Wang H and Zhang Z. Randomized Adjuvant Chemotherapy of EGFR-Mutated Non-Small Cell Lung Cancer Patients with or without Icotinib Consolidation Therapy. PLoS One 2015; 10: e0140794. Shi Y, Zhang L, Liu X, Zhou C, Zhang L, Zhang S, Wang D, Li Q, Qin S, Hu C, Zhang Y, Chen J, Cheng Y, Feng J, Zhang H, Song Y, Wu YL, Xu N, Zhou J, Luo R, Bai C, Jin Y, Liu W, Wei Z, Tan F, Wang Y, Ding L, Dai H, Jiao S, Wang J, Liang L, Zhang W and Sun Y. Icotinib versus gefitinib in previously treated advanced non-small-cell lung cancer (ICOGEN): a randomised, doubleblind phase 3 non-inferiority trial. Lancet Oncol 2013; 14: 953-961. Janne PA, Gurubhagavatula S, Yeap BY, Lucca J, Ostler P, Skarin AT, Fidias P, Lynch TJ and Johnson BE. Outcomes of patients with advanced non-small cell lung cancer treated with gefitinib (ZD1839, “Iressa”) on an expanded access study. Lung Cancer 2004; 44: 221230. Int J Clin Exp Med 2016;9(9):18360-18366 The efficacy and safety of icotinib in patients with non-small cell lung cancer [5] [6] [7] [8] [9] [10] [11] [12] [13] Zhou Q, Cheng Y, Yang JJ, Zhao MF, Zhang L, Zhang XC, Chen ZH, Yan HH, Song Y, Chen JH, Feng WN, Xu CR, Wang Z, Chen HJ, Zhong WZ, Liu YP and Wu YL. Pemetrexed versus gefitinib as a second-line treatment in advanced nonsquamous nonsmall-cell lung cancer patients harboring wild-type EGFR (CTONG0806): a multicenter randomized trial. Ann Oncol 2014; 25: 2385-2391. Rosell R, Hu X, Zhang L, Shi Y, Zhou C, Liu X, Wang D, Song Y, Li Q, Feng J, Qin S, Xv N, Zhou J, Zhang L, Hu C, Zhang S, Luo R, Wang J, Tan F, Wang Y, Ding L and Sun Y. The Efficacy and Safety of Icotinib in Patients with Advanced Non-Small Cell Lung Cancer Previously Treated with Chemotherapy: A Single-Arm, Multi-Center, Prospective Study. PLoS One 2015; 10: e0142500. Ni J, Liu DY, Hu B, Li C, Jiang J, Wang HP and Zhang L. Relationship between icotinib hydrochloride exposure and clinical outcome in Chinese patients with advanced non-small cell lung cancer. Cancer 2015; 121 Suppl 17: 3146-3156. Yu Y, Liu H, Zheng S, Ding Z, Chen Z, Jin W, Wang L, Wang Z, Fei Y, Zhang S, Ying K and Zhang R. Gender susceptibility for cigarette smoking-attributable lung cancer: a systematic review and meta-analysis. Lung Cancer 2014; 85: 351-360. Kubota K, Kawahara M, Ogawara M, Nishiwaki Y, Komuta K, Minato K, Fujita Y, Teramukai S, Fukushima M and Furuse K. Vinorelbine plus gemcitabine followed by docetaxel versus carboplatin plus paclitaxel in patients with advanced non-small-cell lung cancer: a randomised, open-label, phase III study. Lancet Oncol 2008; 9: 1135-1142. Siegel R, Naishadham D and Jemal A. Cancer statistics, 2012. CA Cancer J Clin 2012; 62: 10-29. Macedo-Perez EO, Morales-Oyarvide V, Mendoza-Garcia VO, Dorantes-Gallareta Y, Flores-Estrada D and Arrieta O. Long progression-free survival with first-line paclitaxel plus platinum is associated with improved response and progression-free survival with second-line docetaxel in advanced non-small-cell lung cancer. Cancer Chemother Pharmacol 2014; 74: 681690. Zhang Y, Sheng J, Yang Y, Fang W, Kang S, He Y, Hong S, Zhan J, Zhao Y, Xue C, Ma Y, Zhou T, Ma S, Gao F, Qin T, Hu Z, Tian Y, Hou X, Huang Y, Zhou N, Zhao H and Zhang L. Optimized selection of three major EGFR-TKIs in advanced EGFR-positive non-small cell lung cancer: a network metaanalysis. Oncotarget 2016; 7: 20093-108. Shi B, Zhang XB, Xu J and Huang XE. Systematic Analysis of Icotinib Treatment for Patients 18365 [14] [15] [16] [17] [18] [19] [20] [21] [22] [23] with Non-Small Cell Lung Cancer. Asian Pac J Cancer Prev 2015; 16: 5521-5524. Lin JJ, Cardarella S, Lydon CA, Dahlberg SE, Jackman DM, Janne PA and Johnson BE. FiveYear Survival in EGFR-Mutant Metastatic Lung Adenocarcinoma Treated with EGFR-TKIs. J Thorac Oncol 2016; 11: 556-65. Liang W, Wu X, Fang W, Zhao Y, Yang Y, Hu Z, Xue C, Zhang J, Zhang J, Ma Y, Zhou T, Yan Y, Hou X, Qin T, Dinglin X, Tian Y, Huang P, Huang Y, Zhao H and Zhang L. Network meta-analysis of erlotinib, gefitinib, afatinib and icotinib in patients with advanced non-small-cell lung cancer harboring EGFR mutations. PLoS One 2014; 9: e85245. Paez JG, Janne PA, Lee JC, Tracy S, Greulich H, Gabriel S, Herman P, Kaye FJ, Lindeman N, Boggon TJ, Naoki K, Sasaki H, Fujii Y, Eck MJ, Sellers WR, Johnson BE and Meyerson M. EGFR mutations in lung cancer: correlation with clinical response to gefitinib therapy. Science 2004; 304: 1497-1500. Sirotnak FM, Zakowski MF, Miller VA, Scher HI and Kris MG. Efficacy of cytotoxic agents against human tumor xenografts is markedly enhanced by coadministration of ZD1839 (Iressa), an inhibitor of EGFR tyrosine kinase. Clin Cancer Res 2000; 6: 4885-4892. De Rosa V, Iommelli F, Monti M, Fonti R, Votta G, Stoppelli MP and Del Vecchio S. Reversal of Warburg Effect and Reactivation of Oxidative Phosphorylation by Differential Inhibition of EGFR Signaling Pathways in Non-Small Cell Lung Cancer. Clin Cancer Res 2015; 21: 51105120. Zhang HX, Xiong HX and Li LW. Investigation on the protein-binding properties of icotinib by spectroscopic and molecular modeling method. Spectrochim Acta A Mol Biomol Spectrosc 2016; 161: 88-94. Kim YS, Cho EK, Woo HS, Hong J, Ahn HK, Park I, Sym SJ, Kyung SY, Kang SM, Park JW, Jeong SH, Park J, Lee JH and Shin DB. Randomized Phase II Study of Pemetrexed Versus Gefitinib in Previously Treated Patients with Advanced Non-small Cell Lung Cancer. Cancer Res Treat 2016; 48: 80-7. Ni J and Zhang L. Evaluation of Three Small Molecular Drugs for Targeted Therapy to Treat Nonsmall Cell Lung Cancer. Chin Med J (Engl) 2016; 129: 332-340. Singh D, Attri BK, Gill RK and Bariwal J. Review on EGFR inhibitors: critical updates. Mini Rev Med Chem 2016; 16: 1134-66. Li X, Qin N, Wang J, Yang X, Zhang X, Lv J, Wu Y, Zhang H, Nong J, Zhang Q and Zhang S. Clinical Observation of Icotinib Hydrochloride for Advanced Non-small Cell Lung Cancer Patients with EGFR Status Identified. Zhongguo Fei Ai Za Zhi 2015; 18: 734-739. Int J Clin Exp Med 2016;9(9):18360-18366 The efficacy and safety of icotinib in patients with non-small cell lung cancer [24] Yao S, Qian K, Wang R, Li Y and Zhang Y. Comparison of the Efficacy and Safety of Icotinib with Standard Second-line Chemotherapy in 18366 Previously Treated Advanced Non-small Cell Lung Cancer. Zhongguo Fei Ai Za Zhi 2015; 18: 369-373. Int J Clin Exp Med 2016;9(9):18360-18366