Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
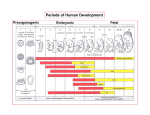
Development of Extraembryonic Membranes and Bilaminar Embryo, 11/5/2010 - Embryo is term used for 1-8 weeks of development, afterwards called fetus (actual fetus on projector) -At the end of 1st 8 weeks, all of the organs have been established, then head into the fetal period where there is growth and maturation physiologic and anatomic maturation occurs of tissues -18 weeks old=size of the hand; 22 weeks are about the same size but these fetuses could be viable, depending on lung maturation; size doesn’t really matter, could be v. small and still survive. -Maturation of the lungs/respiratory function enables baby to survive. -Umbilical cord connects out and attaches to the fetal side of the placenta (in a depression); on the outside is the midterm placenta and other tissue that extends from placenta and completes the chorion sac (outer extraembryonic membrane), part of this becomes the placenta which is the interface btw the mother and fetus. -Amnion (part of the chorion must be removed to show this)—membrane that surrounds the embryo/fetus and contains amnionic fluid (little one develops in this waterbath derived from maternal tissue fluid, diffuses through the chorion and amnion to be within the amnionic cavity; particles from amnionic fluid can also back diffuse back into tissue fluids of endometrium). -When fetus enlarges, there is added amnionic fluid in the form of fetal urine (not like our urine bc kidneys are not concentrating; placenta is used to get rid of fetal waste, diffusing across the placental membrane into maternal blood to be eliminated by maternal kidneys; fetal kidneys are producing fluid that is excreted into amnionic fluid and adds to this). Concurrently with this, embryo begins to swallow around this time, it swallows amnionic fluid which is taken down into stomach and absorbs in proximal small intestine—practice for life outside; this is a secondary balance within the amnionic fluid component, partially derived from maternal tissue fluid. Fetus begins to add to the fluid and then take away from it. -If fetus cannot take away fluid (cannot swallow)- POLYHYDRAMINOUS, fluid builds up. OLIGHYDRAMINOUS- not enough fluid (fetal kidneys do not develop, cannot provide its own fluid). -Amnionic fluid- in contact with the surface of the fetus so that it helps with fetal cells exfoliating; exfoliated cells can be found within the amnionic fluid. Syringe into amnionic cavity this is done to examine DNA and see genetics. Also can examine fetal maturity this way by looking at the chemicals (especially lung fetal maturity). -Amnionic fluid has no nutritive value. Function is to keeps little one hydrated; it is a body temperature waterbath. Before skin maturations, little one loses water through the skin, so it is one with it’s surroundings- fluid moves back and forth. Amnionic fluid= chemical environment for fetus (secreted by the embryo/fetus) to develop in; serves as a cushion, especially for the developing skeleton. Embryo and early fetus is gelatinous (all cellular) and cannot withstand pressure. Chorion grows rapidly, amnion and fetus grow within this. Amnionic cavity filled with it’s fluid provides a buffer for the little one therefore uterine contractions do not hurt fetus. Amnioniic fluid also serves as a hydrallic wedge, when little one wants to get out. Urinary contractions force down on amnion, which pressurizes on fetus, also moving inferiorly into the cervical canal (lower part of uterus which holds little one in place, preventing it from escaping). Cervix has softened in 3rd trimester, cervical canal gets dilated by pressure produced by uterine contractions. Cervix must be widely dilated before membranes rupture and amnionic fluid is released; otherwise the head will produce the wedge with dilates the cervix; molding of head by passage through cervical canal and into vagina. Amnionic membrane is rather fragile (can be durable though, depends on exact dimensions); chorion is tougher. - placental portion of chorion- divided into lobules-Cotelydons (first 2 “leaves” in botony), each is a functional unit of the placenta. Mature placenta- maternal aspect is deep within, away from amnionic cavity containing fetus. Cotelydons (pic on right) have increased in number at this point. As placenta develops, it explands adding more tissue to it, developing into more peripheral cotelydons. See umbilical cord and vessels radiating out. Around egde is amnion and chorion. Middle thin tissue is amnion. Looking at ID twins (monozygotic), embryo divided very early into 2 separate units; can develop within one chorion but each has their own amnionic cavity. Fraternal twins (dizygotic twins) developing from separate oocytes being fertilized have own separate chorion and own separate amnion, but developing within uterus at same time. Sometimes twins share circulation back and forth (in humans, dangerous in animals btw male and female animals bc male hormones will negatively affect female body); one placenta may be larger than the other. Placenta is about size of paper plate and about 2 inches thick. - MRI of mother (who was having pain, about mid pregnancy; though she may have had appendicitis), do not do CTs or Xrays on pregnant woman (MRI’s are safe, but don’t use unless you have to). See little one in normal position, head down; it can move around. Can see deformation of body wall or feel baby moving on mom who is moderately pregnant, would not see this early on. Amnionic fluid appears white, fetus has grown enough to fill chorion. Mid pregnancy and on mom goes to the bathroom a lot because baby pushes on bladder. Can see umbilical chord coming out of the little one going into the placenta. Anterior wall is thicker than the posterior wall in uterus because this is where placenta is. Usual place for implantation is rather high on the posterior wall within the uterine cavity. Little one fills space within amnionic cavity and uterus; under other circumstances that area would be filled with intestinal tract this is squished over and moved to side. Mature fetuses (just before birth) occupy entire space of uterine cavity; there is some fluid there. Menses= beginning of cycle, endometrium from previous cycle is lost; lasts 3-4 days. Follicles within ovary develop during this time and releases estrogen which cause the endometrium (lining of uterus) to proliferate/regenerate. At mid cycle, one follicle in humans usually ruptures (ovulates) releaseing a 2ndary oocyte and other materials; 2ndary oocyte is picked up by uterine tube to travels to uterine cavity. If it is fertilized, development will begin within distal portion of uterine tube. Zygote will transit down uterine tube (1 week), These developing cells are surrounded by zona pellucida (acellular substance; produced partially by oocyte and partially by cells surrounding it known as corona radiata As cells divide by mitosis this increases # but cells become smaller units, so DNA is replicating (can’t enlarge bc of ZP surrounds and confines it.). Functions of ZP: 1) 2) somewhat controls/monitors the env. that oocyte is developing in; aids sperm in fertilizing oocyte 3) helps hold early cells together 4) prevents implantation until conceptus is old enough to implant properly and then it disappers. Cells are organizing themselves. Cavity develops within the developing mitotic cells= blastocele (blast= formative structure; this particular one is cystic in nature) blastocyst= the whole thing, space within is blastocele (“cele”= body cavity). As it enters uterine cavity, ZP dissolves. Conceptus now comes in contact with the lining of the uterine cavity and begins to burrow in/implant. ** Important: 2 weeks after ovulation the ovarian structure that remains (corpus luteum,) degenerates and it’s fxn ends. This is what has been producing progesterone which maintains endometrium. Estrogens produced by developing follicle causes regeneration of the endometrium. Progesterone in maternal system ripens endometrium so it is ready for implantation and maintains it. CL under normal circumstances has effects of producing progesterone only last for 14 days after ovulation. Loss of progesterone (14 days after ovulation), and the endometrium begins to degenerate, which shifts into menstrual period and gets ready for next ovarian cycle. Uniform/constant time period occurs between the time of ovulation and the onset of the next menstrual period. Variable time is btw onset of menstruation and ovulation. Little one puts out hormones/substances as moving through uterine tube and implanting to notify the mother that it is present and mother’s body needs to prepare for the little one to have a place to live (early pregnancy factors) to maintain CL, maintain progesterone and maintain endometrium.. Conceptus= products of fertilization; includes embryo proper (becomes new individual) and the extraembryonic tissue; there may be intraembryonic or extraembryonic portions; BVs may be intra or extraembryonic Mesoderm= can be intra or extraembryonic Corona radiata are follicular cells, ovulated with the oocyte, make oveulated mass easier for the uterine tube be able to handle and transport more easily; surrounded by ZP and inside is oocyte. Initially oocyte is right up against ZP. Sperm that make it through the cervical canal into the uterine tubes (traveled 8-10 inches), they approach the ovulated mass which generates chemical signaling into fluid in uterine tube for the sperm to come to it (also peristaltic activity moves oocyte downward); Sperm that reach sperm release acrosomal enzymes from their head, to break down CR. This allows other sperm to be able to make contact with ZP, which has chemical receptors on it allowing sperm to dock which then release more enzymes creating a path through ZP. 1 Sperm gets in; fuses with oocytic membrane that is in contact with ZP; membranes fuse, nuclear material and mitochondria move into the cytoplasm of oocyte. This triggers a cortical reaction, enzymes in storage vesicles around outside periphery of ooctye are released causing a chemicals change within ZP so that further sperm cannot digest there way through, oocyte then retracts a bit from the ZP (a gap is created btw ZP and outercell membrane of ooctyte), this is good bc it takes time for chemical changes to take place, so that sperm cannot get in to reach the oocyte even if it has pushed through ZP. In some cases 2-3 sperms can come in contact with oocyte producing a multiple fertilization (“ployspernia”), these conceptuses are typically not viable and die very quickly. **Recap: ZP is docking site for sperms helping them in fertilization process, impedes sperm to a degree because they need to digest their way through, undergoes a chemical change to prevent further sperm from moving in. Excess nuclear material is discarded in form of polar bodies ZP then surrounds cells undergoing mitosis, keeping them corralled; at day 5-6 conceptus moves into uterine cavity, it hatches from ZP which then breaks down allowing conceptus to move out and swell and enlarge, blastocyst hatches, blastocele forms and gets bigger (there is an outercell mass and an innercell mass, these have begin to differenciate, no longer multipotential); at day 6-7 it begins to make contact with endometrium, begins implantation process. Morula= “mulberry”; loose connection of cells before the cavity develops, cells have microvilli extending from surfaces; are joined together with jxnal complexes so that they can share info back and forth. Early on can take cells from blastocyst (in animals), mix them up and let them reaggregate and they go on and continue proper development; once there is an outer and inner cell mass these cells have partially differentiated. Inner cell mass becomes embryo proper, outer cell mass becomes supportive tissues for developing embryo. Endometrium- mucosal lining of uterus; consists of epithelium, stroma (connective tissue), maternal BVs (endometrium is a very glandular and vascular tissue). Myometrium- muscular wall of uterus -Implantation of blastocyst: implanatation= growing into another structure; in this case it is movements of conceptus from uterine cavity into stroma of edometrium; humans have interstitial implantation, conceptus invades and migrates into stroma of endometrium (implantation occurs in interstitial, intercellular space of endometrium, losing contact with uterine cavity), while breaking through epithelial lining (becoming invasive); different animals have different types of implantation, some not as intimate as in humans (sometimes conceptus remains in the uterine cavity). There are pros and cons to each. What’s happening on the outside (establishes what implants into maternal body)- Blastocyst (stage at which inner cell and outer cell mass exist) looks for an attachment point on endometrium. Implantation is not a one way street: Endometrium releases substances that attract conceptus, and conceptus releases substances that move it towards endometrium - (handshake relationship, reciprocal; if coordinated appropriately then a successful implantation will take place); birthcontrol interferes with this! Decidua= altered endometrial stroma (to fall away); during implantation, as conceptus invades, stroma is stimulated to change its nature (this is normal); at birth most of decidua comes off. 3 types/portions of decidua: - - 1. Decidua Basalis= btw conceptus and myometrium, 2. Decidua Capsularis- btw conceptus and uterine cavity; makes a capsule over conceptus at implantation site (temporary layer), as conceptus enlarges blood supply to Decidua capilaris is compromised and perfusion drops, tissue degenerates 3. Decidua Parietalis- everything else, wall of uterine cavity. Eventually all of endometrium undergoes decidual reaction Eventually there is a drop of perfusion and the decidua capsilaris degenerates, everything is well anchored into deciduas basalis by then, so not in danger of dislodging. BLASTOCYST-- Group of cells on inside= inner cell mass (embryoblast will give rise to embryo proper), on outside= outercell mass (trophoblast) Embryoblast is divided into an epiblast (gives rise to embryo proper…ectoderm, mesoderm ( inside embryo), endoderm) and a hypoblast (temporary, will give rise to extraembryonic mesoderm= this mesoderm is outside embryo!) Trophoblast (= “to feed or support”) differenciates into 2 different types of tissue: 1) Cytotrophoblast- will be discrete cells, individualized, these tend to be reserve cells meaning that they will develop into something else and will be reduced in number as development proceeds, their cytoplasm will grow into syncytiotrophoblast and merge to give rise to more syncytiotrophoblast). (Syncytium= “multinucleated cytoplasmic mass” ). Cytotrophoblast comes in contact with maternal tissue but not maternal blood. 2) Synctitiotrophoblast (within trophoblast, within placenta)- differentiated, specialized tissue, this gives rise to hormones and make contact will maternal blood. Cytotophoblast cells continue to migrate through syncyctiotrophoblast and migrates into desidua; increases amount of synctytiotrophoblasts, as cytotrophoblast cell membranes break down and they fuse to form syncyctiotrophoblast. Synctyctiotrophoblast comes in contact with maternal tissue and blood. As implantation continues, there is more and more synctyciotrophoblast Lacuna= (“space”) membrane bound spaces within the syncytiotrophoblast; will become the intervillous space within the placenta; these membrane bound spaces will ultimately contain the maternal blood, when it comes in contact. Membrane bound spaces will coalesce to form larger spaces. See fig 4.15 in powerpoint Maternal Blood reaching Lacunae: When trophoblast comes in contact with the decidua (or with the endometrium), the cytotrphoblastic cells begin to proliferate, these will break down and join together to form syncytiotrophoblast located on outside of outercell mass in contact with maternal tissue. Syncytiotrophoblast grows into endometrium and decidual reaction occurs. Syncytiotrophoblast comes in contact with small maternal BVs (hopefully, so that pressure is low and it doesn’t cause hemmorage) within endometrium ; eats its way into maternal vessels, which releases maternal blood into lacunae. Chorionic villus has several stages of development, chorionic villi hang into the blood-filled intervillus space; in mature state they contain fetal BVs Primary chorionic villi- cyto and synctitiotrophoblast Secondary chorionic villi- (developmental stage)syncytiotrophoblast, cytotrophoblast, and extraembryonic mesoderm that’s grown in from hypoblastic cells; no BVs Tertiary chorionic villi- has core extraembryonic mesoderm and embryonic fetal BVs derived from this extraembryonic mesodermal core which is surrounded by the 2 trophoblastic layers ** Overall Process, review: Blastula is freed from ZP, comes in contact with maternal tissue (endometrial wall); wants a blood supply; cytotrophoblast proliferate and develop syncytiotrophoblast which invades endometrium; syncytiotrophoblast develops on outside of outer mass where it meets endometrium. Hypoblastic cells proliferate and migrate down on inside of cytotrophoblast (on inside of outercell mass), forming a second lining now, giving rise to extraembryonic mesoderm which develops btw inner cell mass and 1st layer of hypoblastic cells (hypoblast is temporary layer and eventually becomes extraembryonic mesoderm or a structural lining). As implantation continues, cytotrophoblasts proliferate and grow into synctitiotrophoblast (there are no discrete cellular boundaries here) enabling this to grow further into endometrium. Concurrently, extraembryonic mesoderm also follows the cytotophoblasts responsible for syncytiotrophoblast growth, forming extraembryonic mesodermal cores and extraembryonic BVs develop within extraembryonic mesoderm giving rise to vessels on the placenta. Finally, extraembryonic BVs develop within the extraembryonic mesoderm, which will link up with circulatory system developing within the embryo proper. Once we have invaded all the way in, endometrial epithelium closes over. Cytotrophoblastic shell- before this develops, endometrium has changed into deciduas, which is unable to recognize foreign substances, therefore it does not attack the developing embryo. Extraembryonic mesoderm gives rise to BVs on the placenta, this will go all the way around conceptus. Hypoblast eventually becomes extraembryonic mesoderm Thin membrane btw maternal and fetal blood; fetal BVs come in direct contact from basal lamina with basal lamina of syncytiotrophoblast, and eventually there is a barrier btw maternal and fetal blood, and this barrier is not very selective. Nutrition is picked up from diffusion of particles via maternal blood, nourishing the embryoblast