Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
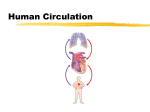
Circulation of Blood • Overview: Two Circuits • Goal: Get Blood to Capillaries • Capillary Beds • Arteries and Veins • Blood Pressure • Control of Circulation and Blood Pressure Larry M. Frolich, Ph.D., Yavapai College Overview—Two circuits • Pulmonary Circuit: Right side of heart pumps blood to lungs to pick up oxygen • Systemic Circuit: Left side of heart pumps blood to rest of body to deliver oxygen • Schematic does not show left/right symmetry for most of circulatory system Goal—get blood to capillaries • Pulmonary circuit—right side of heart pumps blood through pulmonary arteries to capillaries • Oxygen diffuses into blood and RBC’s in lungs at alveoli surrounded by capillaries • Pulmonary veins return blood to left side of heart • • • • Systemic left side of heart pumps blood through systemic arteries to capillaries Oxygen diffuses out of blood and into interstitial fluid around cells making oxygen available for cellular metabolism. This is the grand goal of the circulatory system—where the real action happens Besides oxygen, water, glucose and other nutrients are delivered; CO2, waste products are picked up Systemic veins return blood to right side of heart Action at the capillary beds • Every cell of every tissue of body must be close to a capillary • Capillaries are microscopic—often just one RBC in diameter • Remember—diffusion is the way substances (like oxygen, nutrients) to move in and out of cells and across membranes (like capillary wall) Capillaries form “beds” or networks that connect from artery to vein Capillaries—more realistic views More realistic drawing showing network of capillaries connecting arteries to veins and threading through tissue. Open-ended lymph capillaries pick up excess fluid from tissue and also give immune cells route back into blood circulation Photomicrograph of stained blood vessels of retina showing intricate capillary network Electron micrograph showing arterioles, tiniest of arteries, splitting into virtual sheet of capillary network that brings blood into very close proximity with almost every cell in the tissue. Histology of the capillary wall • • • • Wall of capillary is simple squamous epithelium Basal lamina is thin collagen layer on external surface that gives structure Fenestrated capillaries with pores in the epithelial cells are found where rapid exchange of water or solutes is needed: e.g. absorptive parts of intestines, choroid plexus in ventricles of brain, endocrine glands like hypothalamus, pituitary Smooth muscle sphinchters control flow through capillary bed (somatic or visceral/autonomic or no innervation?) Fluid flow at capillary—from filtration to reabsorption • • • As blood moves through capillary, fluid first diffuses out (filtration), along with dissolved solutes that will fit through spaces between endothelial cells Then, fluid is reabsorbed close to veins This transition will become especially important when we study kidney Arteries and Veins—almost always run together in NAV Artery/Vein differences Arteries (aa.) Direction Blood Away from of flow Heart Pressure Higher Veins (vv.) Blood to Heart Walls Lumen THICKER: Tunica media thicker than tunica externa Smaller THINNER: Tunica externa thicker than tunica media Larger Valves No valves Valves (see next) Lower • William Harvey (1578-1627) • Exercitation Anatomica de Motu Cordis et Sanguinis in Animalibus (An Anatomical Exercise on the Motion of the Heart and Blood in Living Beings) (1628) • Famous veinous flow valve experiment • Easy to repeat—just try it if you’ve got the veins Where’s the blood? Mostly in your veins • • • • • “Venous reserve” is about 20% of blood– pooled in skin, liver, lungs Veins can be constricted to move this blood out and to vital organs like brain, muscles when needed Venous blood is under almost no pressure to move it along Skeletal muscle action moves venous blood ahead of next valve Long periods of inactivity can lead to pooling of blood Heart pushes blood through vessels against resistance • • • Factors that affect blood pressure Heart contracts to push blood into vessels Friction causes resistance of movement of any fluid through a pipe or tube Heart has to pump enough volume to create enough pressure to overcome resistance, but not too much which will cause high blood pressure (hypertension) and can lead to many secondary problems Blood Pressure—overview Blood pressure in arteries is constantly changing to counteract variability in resistance • Gravity alone makes for huge differences in amount of pressure needed to overcome resistance and get blood to organs • Standing up from lying creates an instant need for total change in blood distribution—lat-time leads to dizzy sensation and even fainting. • Exercise also changes the amount of blood (and pressure that blood is under) needed in different parts of the body • What about a giraffe or dinosaur! Online text about Dinosaur Evolution with great images and links, by David Esker Blood Pressure—the body’s fundamental challenge • Vessels provide resistance, heart pumps to overcome resistance • How does body use feedback information to control vessel size and resistance as well as heart output. This is what maintains blood pressure in a normal range • High blood pressure results when size of artery dilation is too small for the volume of blood being pumped (or the volume of blood being pumped is too great for arterial dilation) • So we need to understand two things: – INPUT: How does body “know” what blood circulation needs are – OUTPUT: How does body control response to those needs Input on blood pressure to brain • Chemoreceptors – aortic bodies, carotid bodies – Sense CO2, pH, O2 • Barroreceptors – stretch receptors sense blood pressure pushing on vessel wall – aortic sinus, carotid sinus Bonus A and P I Review: Cranial Nerve that carries aortic receptor input to brain? IX. Vagus Cranial Nerve that carries carotid receptor input to brain? IX. Glossopharyngeal • If CO2 is high, what is needed? – – Response to chemoreceptor (aortic, carotid bodies) input: (Physiology is common sense—think it through) • If O2 is low, what is needed? – – • Arteries: constrict or dilate? Heart output: more or less? Arteries: constrict or dilate? Heart output: more or less? Is this sympathetic or parasympathetic response? • If blood pressure rises, what is needed? – – Response to Baroreceptor (aortic, carotid sinus) input: • (Physiology is common sense—think it through) • Arteries: constrict or dilate? Heart output: more or less? If blood pressure falls, what is needed? – – Arteries: constrict or dilate? Heart output: more or less? Which response is sympathetic (NE); which is parasympathetic (ACH)? Reflexive output: heart rate • Baro- and chemo-receptor input arrives to medulla oblongata (A and P I review!) • Autonomic motor output (A and P I review) to AV node of heart – Sympathetic will speed heart rate (where do sympathetic neurons originate? What is path to heart? – Parasympathetic will slow heart (where do parasympathetic neurons originate? What is path to heart?) • Bonus (common sense physiology!): Will blood vessels constrict or dilate with sympathetic response? A and P I Review Sympathetic = “fight or flight” = NE (norepinephrine) Parasympathetic = calming = ACH (acetylcholine) Reflexive output: vessel dilation and constriction • Baro- and chemo-receptor input arrives to medulla oblongata (A and P I review!) • Autonomic motor output (A and P I review) directly to blood vessel smooth muscle and capillary sphincters? • Autonomic output to stimulate secretion of adrenalin (E, NE) • Adrenalin will cause vessel constriction – Physiolog common sense: – Does this increase or decrease blood pressure? – Does this work with increase or decrease in heart rate? So, what causes high blood pressure? • • • • • • • Too much heart volume output or too much fluid/blood in system? Vessels are too constricted? Easy case: High blood sugars in diabetes damages small blood vessels leading to increased resistance—thus hypertension frequently accompanies diabetes Most of the time, root cause is difficult to determine. Control is much more complex than just general input from chemo- and baro-receptors and generalized reflexive output response. Local input and response is very important. Remember capillary sphincters… Regulating fluid and salt levels is crucial—why? (common sense physiology…think it through) Site of action of medications to control high blood pressure Holistic approaches to hypertension which are scientifically proven to work. • • • • • • • • • Reduction is salt intake. This reduces the circulating fluid. Therefore blood pressure falls. Proof: Take a lot of salt, you will drink plenty and your blood pressure will increase because your circulatory system has too much fluid. You can reverse this process and see the results for yourself. You do not need to be a scientist. Regular activity. Doing exercises (or physical activity as part of your daily routine) will lower your blood pressure. The reasons are two fold. First, the heart becomes stronger and beats more efficiently and secondly the blood vessels become more elastic and therefore have more recoil (elasticity). Proof: Stop exercising for two months and you will loose all the benefits of your exercises. Healthy Diet: Reduce cholesterol and red meat intake. The elasticity of your blood vessels will improve. There will be minimal or no plaque deposits in your blood vessels. This is important because the plaque decreases available space for your blood to travel around the body. Zero Cigarettes: The vasoconstriction brought about by cigarettes increases blood pressure. Coffee and other vasoconstrictors should be avoided. Stress, job related or not, must be reduced. Relaxation has a BP reducing effect on the body. Watch what medications you are taking. Many non-steroidal anti-inflammatory drugs, diet pills, steroids, antidepressants and monoamine oxidase inhibitors are known to be major causes of hypertension. Weight. If you weigh too much your heart has to supply oxygenated blood to all the fat you are carrying. So it has to produce a higher blood pressure, otherwise the oxygenated blood will not reach all the fatty and not so fatty tissues. Alcohol. Research shows that consuming more than 3 to 4 ounces of 80-proof alcohol per day will result in hypertension. One to two drinks per day is considered satisfactory. Question your holistic practitioner’s motives. Does he get a commission on his sale to you. Is there a professional body to verify what he/she is telling you is correct. If in doubt, move on. BRAINSTORM: How should increased activity level or exercise affect blood pressure readings? (do exercise physiology lab to find out!) Guyenet Nature Reviews Neuroscience 7, 335–346 (May 2006) | doi:10.1038/nrn1902 Numerous factors cause rises in blood pressure (BP), for example, pain and physical exercise. Increases in BP are brought about predominantly through three mechanisms. One involves the stimulation of glutamatergic rostral ventrolateral medulla (RVLM) barosensitive neurons via spinoreticular afferents (pain and muscle receptors) or inputs from more rostral structures (central command) 1). A second mechanism is a reduction of the baroreceptor feedback due to a biasing of the transmission between baroreceptor afferents and second-order neurons in the nucleus of the solitary tract (NTS) (2). The mechanism relies on pre- and postsynaptic inhibition mediated by GABA ( -aminobutyric acid) and other substances such as vasopressin (not represented). Last, the baroreflex is also under humoral control (3). Circulating angiotensin II (Ang II), for example, also reduces transmission between baroreceptor afferents and second-order neurons. The mechanism of angiotensin II control of the baroreflex involves the production of nitric oxide (NO) by the capillary endothelium, and this mechanism could have a role in neurogenic hypertension 75. CVLM, caudal ventrolateral medulla; Glu, glutamate; SGN, sympathetic ganglionic neuron; SPGN, sympathetic preganglionic neuron.