Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
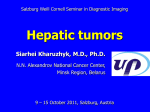
2010 THE AUTHORS; BJU INTERNATIONAL Urological Oncology 2010 BJU INTERNATIONAL INCREASED PROSTATE CANCER DETECTION WITH MULTIPARAMETRIC MRI DELONGCHAMPS ET AL . BJUI Multiparametric magnetic resonance imaging for the detection and localization of prostate cancer: combination of T2-weighted, dynamic contrast-enhanced and diffusionweighted imaging BJU INTERNATIONAL Nicolas Barry Delongchamps*, Mathieu Rouanne*, Thierry Flam*, Frédéric Beuvon†, Mathieu Liberatore‡, Marc Zerbib* and François Cornud‡ Departments of *Urology, †Pathology and ‡Radiology, Cochin Hospital, Paris Descartes University, Paris, France Accepted for publication 25 May 2010 Study Type – Diagnostic (exploratory cohort) Level of Evidence 2b What’s known on the subject? and What does the study add? Dynamic contrast enhanced (DCE) and diffusion weighted (DW) MRI have demonstrated their potential value in distinguishing malignant from benign prostate tissue, but none of them used alone is capable of optimally characterizing tumours in the prostate. The combination of DW, DCE and T2W imaging increased significantly MRI performance for cancer detection in the peripheral zone. OBJECTIVE • To evaluate the combination of multiple magnetic resonance imaging (MRI) techniques, including T2-weighted imaging (T2W), dynamic contrast-enhanced imaging (DCE) and diffusion-weighted imaging (DWI), for the detection and localization of prostate cancer. techniques combined were scored for the likelihood of tumour in each area and results were compared with whole-mount analysis. • The area under the receiver operating characteristic curve (Az) was used to evaluate accuracy for tumour detection. The association between MR accuracy and Gleason score was statistically assessed. • The Az value for T2W + DWI was significantly higher than that for T2W + DCE or for the three sequences combined. • Gleason score was significantly associated with cancer detection in the PZ. CONCLUSIONS PATIENTS AND METHODS RESULTS • In all, 57 patients underwent endorectal MRI at 1.5 T before radical prostatectomy (RP) for localized prostate cancer. • On T2W images and histological wholemount analysis, the peripheral zone (PZ) and transition zone (TZ) were divided into upper and lower glands, as well as left and right halves, thus yielding four quadrants for each zone. • On histological analysis, the total number of tumour foci, their location and larger diameter were recorded. T2W alone, T2W + DWI, T2W + DCE and all three INTRODUCTION With the widespread use of PSA screening, up to 80% of patients diagnosed with prostate cancer are staged T1c. This downward stage migration has led to the identification of © • Of the 456 prostate octants analysed, 145 showed cancer on whole-mount analysis, 120 (83%) of them with a diameter assumed to correspond to a volume >0.2 cm3. Gleason score was ≥7 in 68 (47%) tumours. • In the PZ, the Az value was significantly higher for T2W + DWI, T2W + DCE and all three techniques combined than for T2W alone (P < 0.05). • In the TZ, the Az value was higher for T2W + DWI than for T2W alone, but the difference was not significant. small and well-differentiated cancers at radical prostatectomy (RP). These cancers, designated as ‘clinically insignificant’ [1], should probably not be managed with radical and possibly morbid treatment. Development of active surveillance and, more recently, focal • Adding DWI and DCE to T2W imaging increased MRI performance in cancer detection in the PZ significantly. • However, this multiparametric model failed to improve performance in the TZ. • Gleason score significantly influenced cancer detection in the PZ but not in the TZ. KEYWORDS prostate cancer, detection, localization, dynamic contrast-enhanced MRI, diffusionweighted imaging ablation, has led clinicians to reconsider the management of these patients. However, the disease characteristics require to be better clarified. Staging tools are therefore needed to identify patients who can be managed without radical treatment. 2010 THE AUTHORS BJU INTERNATIONAL © 2 0 1 0 B J U I N T E R N A T I O N A L | 1 0 7 , 1 4 11 – 1 4 1 8 | doi:10.1111/j.1464-410X.2010.09808.x 1 4 11 D E L O N G C H A M P S ET AL. The presence of adverse pathological features on biopsy, high PSA level or PSA doubling time, and/or suspicion of extracapsular or seminal vesicle invasion on T2-weighted MRI are clearly predictive of aggressive disease [2]. However, it is far more difficult to determine precisely the number and location of tumour foci within the gland. None of these staging procedures offers an accurate prostate mapping of the disease. Attempts at histological mapping of the prostate have been made with saturation transrectal and transperineal prostate biopsies [3]. However, correlation analyses with whole-mount glands show that even these procedures can miss up to 40% of cancer foci [3]. Prostate MRI has undergone several technical improvements and is showing promise for prostate tumour detection and localization. In addition to morphological information, MRI can analyse the physiological properties of tissues. T2-weighted (T2W) MRI measurement is dependent on free water abundance and macromolecular environment. Diffusionweighted imaging (DWI) is sensitive to restriction of water molecule diffusion [4], and dynamic contrast-enhanced (DCE) MRI is capable of assessing microvascular properties [5]. All these techniques have shown their potential value in distinguishing malignant from benign prostate [4,5]. However, none of them used alone is capable of optimally characterizing tumours in the prostate. Recent studies have showed that their combination could reinforce and/or complement each other [4,6]. On the other hand, combining techniques of different accuracy could also decrease their potential detection value. The optimal combination of large amounts of multiparametric imaging data therefore remains a challenge. The present study aimed to evaluate the combination of multiple MRI techniques, including T2W imaging, DCE and DWI for the detection of prostate cancer. PATIENTS AND METHODS Between November 2008 and April 2009, 57 consecutive patients with biopsy-proven prostate cancer underwent T2W MRI, DCE and DWI before RP in our institution. Magnetic resonance images were obtained with a 1.5 T imager (Avanto, Siemens Medical Systems, Erlangen, Germany) and an integrated endorectal pelvic phased-array coil 1412 (MR Innerva; Medrad, Pittsburgh, PA, USA). The endorectal coil was inserted and inflated to a volume of ≈80–100 mL. The examination started with a short biplane (20 s) localization sequence to check the position of the rectal coil and to ensure that the different sequences would cover the whole prostate, including the seminal vesicles. The threedimensional T2W fast spin-echo sequence was then acquired (repetition time [TR]/echotime [TE], 1300/120; field of view [FOV], 18 cm, matrix, 186 × 256). It provided 224 images (voxel size, 0.8 × 0.8 × 1 mm) covering the whole pelvis up to the aortic bifurcation. DW images (TR/TE, 3700/104; FOV, 18 cm; matrix, 186 × 256; slice thickness, 3.5 mm) were obtained by using single-shot spin-echo echo-planar imaging. Two b values (b0–b800) were used and restriction of diffusion was quantified by the apparent diffusion coefficient (ADC) value. The orientation and location of the images (20 slices) were prescribed identically to the transverse T2W prostate images. The gradient echo DCE data sets (TR/TE/flip angle, 5.11/1.85/10; slice thickness, 3.5 mm; temporal resolution, 8.5 s, 35 phases) were obtained after a bolus injection of gadolinium (0.1 mmol/kg; rate of injection, 3 mL/s, power injector, followed by a 15 mL flush of saline) and transferred to an independent workstation where a pharmacokinetic model derived from the Tofts model (iCAD, Nashua, Park Ridge, IL, USA) was used to convert the variations of signal intensity into variations of gadolinium concentration. Pharmacokinetic variables were determined, including Ktrans (forward volume transfer constant), Kep (reverse reflux rate constant between extracellular space and plasma), and the area under the gadolinium concentration curve (AUGC) in the first 60 s after injection. MRI PROSTATE MAPPING AND EVALUATION OF DATA Two experienced radiologists (FC, ML) interpreted the MR images by consensus. They were blinded to clinical (rectal examination), biological (PSA value) and pathological results (biopsy and RP specimen findings). The peripheral zone (PZ) and the transition zone (TZ) of the prostate were divided into upper and lower glands, as well as left and right halves, thus yielding four quadrants for each zone and 576 areas for the whole series. The limit between the upper and lower gland was defined as the section running through the widest transverse diameter of the prostate. As detection and localization of prostate cancer by functional MRI was the only goal of the present study, assessment of extracapsular extension was not taken into account. If the focus was detected on more than one sequence, the size of the tumour focus was measured on the sequence showing the largest diameter. On the T2W sequence, the observers assigned a score to each focus using a two-point scale: 0, benign; 1, malignant. In the PZ, mass-like hyposignals were considered as suspicious for cancer, whereas heterogeneous patterns or nonmass-like hyposignals were considered as benign. In the TZ, only homogenous, anteriorly located and lenticular-shaped hyposignals were considered as suspicious for cancer [7]. According to the ADC value, the observers assigned a three-point scale score: 0, benign (ADC > 1500); 1, indeterminate (ADC = 1200–1500); 2, malignant (ADC < 1200). For DCE MRI, the iCAD’s pharmacokinetic analysis software used the whole DCE curve that had 35 phases with 8.5 s temporal resolution and implemented Tofts model. The default Weinmann arterial input function (AIF) was used [8]. Based on the brightness of the colour-coded value of each parameter, the observers assigned a three-point scale score: 0, benign (dark); 1, intermediate (mid-bright); 2, malignant (bright). The scores obtained were added together to obtain a three-point scale for T2W + DWI, a seven-point scale for T2W + DCE, and a nine-point scale for all sequences combined (Figs. 3-5). HISTOLOGICAL EVALUATION Radical prostatectomy specimens were fixed overnight (with 10% neutral-buffered formaldehyde) and coated with India ink. Seminal vesicles were separated from the prostate and processed separately. The glands were cut into 4-mm sections perpendicular to the posterior plane, labelled, embedded in paraffin, and further sectioned to produce 5μm whole-mount sections that were stained with haematoxylin and eosin. A single pathologist (FB) microscopically reviewed all samples. The total number of tumour foci and their location were recorded. An area of carcinoma was considered a separate focus if it was separated by a low-power field diameter (4.5 mm) from the nearest adjacent focus. Each tumour focus was graded according to the modified Gleason grading system [9]. The volume of each tumour focus © BJU INTERNATIONAL © 2010 THE AUTHORS 2010 BJU INTERNATIONAL INCREASED PROSTATE CANCER DETECTION WITH MULTIPARAMETRIC MRI N (%) Rectal examination Normal Suspicious Number of prostate cancer cases Number of prostate areas analysed Number of tumour foci In the PZ In the TZ Gleason score Gleason ≤ 6 Gleason ≥ 7 Tumor diameter (>7 mm) In the PZ In the TZ 43 (76) 14 (24) 57 456 FIG. 1. Comparison of ROC curves between T2W (T2) imaging alone, T2W + DCE (T2_DCE), T2W + DWI (T2_DWI) and all three techniques combined (T2_DWI_DCE) for cancer detection in the PZ. 100 80 Sensitivity TABLE 1 Clinical and pathological characteristics of the 57 prostate cancers 60 40 112 33 20 T2 T2_DWI T2_DCE T2_DWI_DCE 77 (53) 68 (47) 0 91 (81) 29 (91) 0 TABLE 2 Sensitivity and specificity of MRI for the detection of prostate cancer, when using the optimal score thresholds Sensitivity, % (95% CI) Specificity, % (95% CI) T2W alone T2W + DCE (>4/7) T2W + DWI (>1/3) T2W + DCE + DWI (>5/9) 63 (53–73) 79* (69–87) 81* (72–88) 80* (70–87) 98 (97–100) 92 (86–96) 93 (87–97) 97 (93–99) T2W alone T2W + DCE (>6/7) T2W + DWI (>2/3) T2W + DCE + DWI (>6/9) 71 (52–85) 47* (30–65) 71 (52–85) 53* (30–65) 98 (95–100) 77* (71–83) 98 (95–100) 83* (77–88) PZ TZ *P < 0.05 vs T2W alone (McNemar test). was estimated according to its larger diameter. A diameter >7 mm was considered to correspond to a tumour volume >0.2 cm3 [10]. MEASUREMENTS AND STATISTICAL ANALYSIS Each pathological whole-mount section was matched to a corresponding MR image on the basis of the location of the ejaculatory ducts, the diameter of the prostate and the approximate distance from the base or apex. A correlation analysis between the MRI and pathological findings was then performed in each of the eight previously defined prostatic regions. Only tumours with diameter >7 mm © Az: 0.81; 95%CI: 0.75–0.86 Az: 0.92; 95%CI: 0.88–0.96 Az: 0.91; 95%CI: 0.86–0.94 Az: 0.92; 95%CI: 0.88–0.95 were considered for the correlation analysis. Receiver operating characteristic (ROC) curves and the corresponding areas under the ROCs (Az) were estimated non-parametrically for the detection of cancer with T2W alone, T2W + DWI, T2W + DCE, and a combination of the MRI sequences. These Az values were compared using a pairwise comparison of ROC curves. Sensitivity and specificity of each MRI combination were calculated and compared using the McNemar test. The chisquared test, which accounts for qualitative variables, was used to compare Gleason score (Gleason <7 vs ≥7) between tumours detected and missed by MRI. All statistical tests were two-sided, and P values <0.05 were considered to indicate statistical significance. 20 40 60 100-Specificity 80 100 Statistical analyses were performed using MedCalc® software, version 11.0.0.0. RESULTS The 57 patients included in the analysis had a median (range) age of 63 (54–76) years and a median (range) PSA level of 7 (2.8–28) ng/mL. Their clinical and pathological characteristics are summarized in Table 1. Of the 145 cancer foci identified on wholemount analysis, 120 (83%) had a diameter >7 mm, corresponding to an estimated volume >0.2 cm3. Gleason score was ≥7 in 53% (53/112) of PZ tumours vs 27% (nine of33) of TZ tumours (P = 0.01). MRI PERFORMANCE FOR CANCER DETECTION IN THE PZ The Az values (Fig. 1) for T2W + DWI, T2W + DCE and all three sequences combined were significantly higher than that for T2W alone (Table 1, P = 0.003, 0.03 and 0.009, respectively). Although T2W + DWI performed better than T2W + DCE, the difference was not significant (P = 0.8). When using the optimal thresholds for determining the presence of cancer, the three MR sequences combined had the highest sensitivity (80%) and specificity (97%) for cancer detection in the PZ (Table 2). A Gleason score ≥7 was associated with greater MRI performance with all the sequence combinations (P < 0.001). 2010 THE AUTHORS BJU INTERNATIONAL © 2010 BJU INTERNATIONAL 1413 D E L O N G C H A M P S ET AL. MRI PERFORMANCE FOR CANCER DETECTION IN THE TZ 80 Sensitivity The Az for T2W + DWI was higher than that for T2W alone, but the difference was not significant (Fig. 2, P = 0.4). Interestingly, T2W alone performed significantly better than T2W + DCE (P = 0.002) as well as all three sequences combined (P = 0.03). As a result, the combination of either T2W + DCE or all three MR sequences significantly decreased sensitivity and specificity (Table 2). Gleason score did not influence MR performance for any of the sequence combinations (P > 0.1). FIG. 2. Comparison of ROC curves between T2W (T2) imaging alone, T2 + DCE (T2_DCE), T2 + DWI (T2_DWI) and all three techniques combined (T2_DWI_DCE) for cancer detection in the TZ. 100 60 40 20 T2 T2_DW T2_DCE T2_DW_DCE Az: 0.84; 95%CI: 0.79–0.89 Az: 0.88; 95%CI: 0.83–0.92 Az: 0.70; 95%CI: 0.63–0.76 Az: 0.75; 95%CI: 0.69–0.80 0 0 DISCUSSION Even if T2-weighted MRI shows a high sensitivity for large-volume tumours [11,12], its accuracy for detection of smaller foci is less well established [13]. In patients with palpable cancer, sensitivity has been reported to be as high as 96% [11]. The real issue, however, is how to detect small confined tumours albeit of substantial volume (>0.2– 0.5 mL). Patients with palpable cancer, high PSA level and adverse biopsy results do not present any challenging staging problem to clinicians. In comparison, patients free of any adverse prognostic factor are potential candidates for focal ablation or active surveillance and need further staging to ensure the absence of large-volume or multifocal disease. For these patients, T2W imaging sensitivity for cancer detection in the PZ may not exceed 20% [13,14]. In this setting, T2W imaging might only be helpful in detecting extracapsular extension, seminal vesicle invasion or large intracapsular tumours close to the capsule. As a result, small, albeit significant, tumours, possibly multifocal and high-grade, could remain under-staged. In the TZ, T2W imaging accuracy for cancer detection was reported to be even worse. Although TZ tumours tend to be less aggressive [15], they can account for up to 30% of cancers. One large series of anterior gland cancers showed that MRI missed 78 of 79 tumours with a volume >0.5 mL [16]. However, more recent reports showed a higher accuracy in the TZ. Using validated criteria for T2W imaging cancer detection in the TZ (anterior homogeneous hyposignal, ill-marginated, lenticular shape) [7], different authors [10,17–19] subsequently reported sensitivities and specificities 1414 20 40 60 100-Specificity ranging between 24–68% and 91–99.9%, respectively. To improve the limited accuracy of T2W imaging, other MR techniques have been developed, including DCE and DWI. In the PZ, DCE MR imaging demonstrated high accuracy for the detection of tumour foci >0.5 cm3 [18,20–22]. However, most of the smaller foci remain undetected [17,23]. In the TZ, limitations of DCE MRI are even higher because of the similar kinetics of gadolinium enhancement in BPH and prostate cancer [24]. More recently, several studies have also suggested the potential benefit of DWI in detecting prostate tumours. The ADC values, which measure the restriction of water molecule diffusion within tissues, were reported to be significantly lowered in malignant vs benign tissue in the PZ [4]. In the TZ, however, ADC values of BPH are in the range of those of prostate cancer [4,24], making DWI of poor diagnostic value in this prostatic area. Owing to the limitations of functional sequences used separately, several authors [6,24–27] suggested that a multiparametric assessment of prostatic tissue, including T2W, DW and DCE imaging, could improve the overall MRI sensitivity and/or specificity. This combination, however, is challenging. The main difficulty lies in how to take into account the different data provided by each of the MR techniques. In particular, if the results of the different techniques disagree 80 100 with each other, which should be given more credit? Should data provided by each technique be balanced according to the assumed accuracy of each technique taken separately? In our study, all variables combined were balanced equally for the interpretation of results: T2W, ADC, Ktrans, Kep and AUGC values had the same impact with regard to data interpretation. This methodology might not provide the optimal results, however, and highlights the difficulties presented by a multiparametric model. This issue was recently assessed by Langer et al. [6]. Using a stepwise regression model, they tested and compared four MRI quantitatively measured variables, including T2W-relaxation time, ADC value, Ktrans and Kep to evaluate which of them provided the best performance for cancer detection in the PZ. The optimal multiparametric model consisted of combining ADC, T2W and Ktrans. However, they also found that ADC was the bestperforming single variable. Although the three variables combined tended to be better than ADC alone, the difference was not statistically significant (P = 0.09). These findings could suggest that the ADC value should be given more power if included in a multiparametric model. The results of the present study suggest that DW and DCE imaging, when combined with an equally balanced power to T2 imaging, add significant accuracy in the PZ compared with T2 alone. Using all three techniques © BJU INTERNATIONAL © 2010 THE AUTHORS 2010 BJU INTERNATIONAL INCREASED PROSTATE CANCER DETECTION WITH MULTIPARAMETRIC MRI FIG. 3. Hypovascular TZ cancer. T2W MRI (top panels): anterior lenticular hyposignal, ill-marginated, anteriorly located in the transition zone. DWI (middle panels): low ADC value in the same area (arrows). DCE MRI (bottom panels): low value of the dynamic variables on a qualitative visual assessment. Histological examination: Gleason score 6 carcinoma (Ca) (arrows). making their detection more difficult with DCE imaging. In the present study, most of the TZ tumours had a low Gleason score, which may explain the poor sensitivity of DCE. In the present study, we excluded small tumour foci (diameter <7 mm) from analysis because they are probably not a clinical issue. Usually considered as ‘clinically insignificant’, they are missed by all MRI sequences, used either alone or in combination. ‘Inapparent tumours’ on MRI are characterized histologically by sparse and low-grade tumour cells intermixed with healthy tissue [30]. The ratio of tumour cells to healthy tissue in these foci may not reach 60% [30]. These histological considerations might be of great interest if tumour cell density appeared to be correlated with cancer progression, which to our knowledge has not yet been reported. If so, MRI could become a strong predictor of either the absence of cancer or the presence of non-aggressive inapparent tumours. combined, we reached a sensitivity of 80% and a specificity of 97% for the detection of tumour foci >0.2 mL. DW imaging seemed to add more performance to our multiparametric model than DCE, as has been suggested before [6]. In the TZ, combined MR sequences failed to improve cancer detection. Interestingly, DCE imaging decreased accuracy significantly, and, as a result, the performance of all three techniques combined. Although DWI added © accuracy to T2W alone, the difference was not significant. These results are consistent with those of Haider et al. [4] and suggest that morphological criteria described on T2W imaging are still the gold standard for the detection of TZ cancer. Although the low accuracy of DCE in the TZ is an established finding [17,18,28], it may not alone explain why the combination of DCE + T2W reached so low a sensitivity (47%). As suggested by one study [29], low-grade tumours have less vascular density than high-grade tumours, The present study had several limitations, one of them being the population studied. For the correlation analysis, we did not select exclusively low-risk patients according to PSA level, rectal examination and biopsy results. These low-risk patients are considered as the potential candidates for focal tumour ablation or active surveillance, for which MRI combination techniques would be of staging value. Additionally, we did not include MR spectroscopic imaging in our multiparametric model, although it does not improve, at 1.5 T, the accuracy of T2W imaging for cancer detection in the PZ (Az, 0.60 vs 0.58, respectively; P > 0.05) [31]. Nevertheless, spectroscopy with high-field 3 T magnets is currently being investigated and might show promise in detection of prostate cancer. Finally, whole-mount analysis of RP specimens focused on tumour foci alone, therefore excluding other lesions, such as prostatitis infiltrates, that can simulate cancer on MRI. Consequently, we were unable to analyse the nature of false-positive images identified on MRI examination. In conclusion, adding DWI and DCE to T2W imaging significantly increased MR performance for cancer detection in the PZ. However, this multiparametric model failed to improve performance in the TZ. Gleason score significantly influenced cancer detection in the PZ but not in the TZ. 2010 THE AUTHORS BJU INTERNATIONAL © 2010 BJU INTERNATIONAL 1415 D E L O N G C H A M P S ET AL. FIG. 4. Prostate cancer originating in the PZ. Bilateral hyposignal on the T2W image (arrows, T2) with a low value of the ADC (arrows, ADC), high K trans (vascular permeability, Ktrans) and Kep (washout, Kep) values, but low AUGC value (arrows, AUGC). FIG. 5 Anterior cancer originating in the TZ. Homogenous and anteriorly located TZ hyposignal on the T2W sequence (arrow, T2), with low ADC value and high values of dynamic variables (Ktrans, AUGC and Kep). 1416 © BJU INTERNATIONAL © 2010 THE AUTHORS 2010 BJU INTERNATIONAL INCREASED PROSTATE CANCER DETECTION WITH MULTIPARAMETRIC MRI CONFLICT OF INTEREST None declared. REFERENCES Stamey TA, Freiha FS, McNeal JE, Redwine EA, Whittemore AS, Schmid HP. Localized prostate cancer. Relationship of tumour volume to clinical significance for treatment of prostate cancer. Cancer 1993; 71: 933–8 2 Montironi R, Vela-Navarrete R, LopezBeltran A, Mazzucchelli R, Bono A. 2005 update on pathology of prostate biopsies with cancer. Eur Urol 2006; 49: 441–7 3 Delongchamps NB, de la Roza G, Jones R, Jumbelic M, Haas GP. Saturation biopsies on autopsied prostates for detecting and characterizing prostate cancer. BJU Int 2009; 103: 49–54 4 Haider MA, van der Kwast TH, Tanguay J et al. Combined T2-weighted and diffusion-weighted MRI for localization of prostate cancer. Am J Roentgenol 2007; 189: 323–8 5 Engelbrecht MR, Huisman HJ, Laheij RJ et al. Discrimination of prostate cancer from normal peripheral zone and central gland tissue by using dynamic contrastenhanced MR imaging. Radiology 2003; 229: 248–54 6 Langer DL, van der Kwast TH, Evans AJ, Trachtenberg J, Wilson BC, Haider MA. Prostate cancer detection with multiparametric MRI: logistic regression analysis of quantitative T2, diffusionweighted imaging, and dynamic contrastenhanced MRI. J Magn Reson Imaging 2009; 30: 327–34 7 Akin O, Sala E, Moskowitz CS et al. Transition zone prostate cancers: features, detection, localization, and staging at endorectal MR imaging. Radiology 2006; 239: 784–92 8 Weinmann H-J, Laniado M, Mutzel W. Pharmacokinetics of GdDTPA/ dimeglumine after intravenous injection into healthy volunteers. Physiol Chem Phys Med NMR 1984; 16: 167–72 9 Epstein JI, Allsbrook WC Jr, Amin MB, Egevad LL. The 2005 International Society of Urological Pathology (ISUP) Concensus Conference on Gleason Grading of Prostatic Carcinoma. Am J Surg Pathol 2005; 29: 1228–42 10 Villers A, Puech P, Mouton D, Leroy X, 1 © 11 12 13 14 15 16 17 18 19 20 Ballereau C, Lemaitre L. Dynamic contrast enhanced, pelvic phased array magnetic resonance imaging of localized prostate cancer for predicting tumour volume: correlation with radical prostatectomy findings. J Urol 2006; 176: 2432–7 Carter HB, Brem RF, Tempany CM et al. Non palpable prostate cancer: detection with MR imaging. Radiology 1991; 178: 523–5 Graser A, Heuck A, Sommer B et al. Per-sextant localization and staging of prostate cancer: correlation of imaging findings with whole-mount step section histopathology. AJR Am J Roentgenol 2007; 188: 84–90 Nogueira L, Wang L, Fine SW et al. Focal treatment or observation of prostate cancer: pretreatment accuracy of transrectal ultrasound biopsy and T2-weighted MRI. Urology 2010; 75: 472–7 Ikonen S, Karkkainen P, Kivisaari L et al. Magnetic resonance imaging of clinically localized prostatic cancer. J Urol 1998; 159: 915–9 Noguchi M, Stamey TA, Neal JE, Yemoto CE. An analysis of 148 consecutive transition zone cancers: clinical and histological characteristics. J Urol 2000; 163: 1751–5 Ellis JH, Tempany C, Sarin MS, Gatsonis C, Rifkin MD, McNeil BJ. MR imaging and sonography of early prostatic cancer: pathologic and imaging features that influence identification and diagnosis. AJR Am J Roentgenol 1994; 162: 865– 72 Cornud F, Beuvon F, Thevenin F et al. [Quantitative dynamic MRI and localisation of non-palpable prostate cancer]. Prog Urol 2009; 19: 401–13 Girouin N, Mege-Lechevallier F, Tonina Senes A et al. Prostate dynamic contrastenhanced MRI with simple visual diagnostic criteria: is it reasonable? Eur Radiol 2007; 17: 1498–509 Li H, Sugimura K, Kaji Y et al. Conventional MRI capabilities in the diagnosis of prostate cancer in the transition zone. AJR Am J Roentgenol 2006; 186: 729–42 Puech P, Potiron E, Lemaitre L et al. Dynamic contrast-enhanced-magnetic resonance imaging evaluation of intraprostatic prostate cancer: correlation with radical prostatectomy specimens. Urology 2009; 74: 1094–9 21 Ocak I, Bernardo M, Metzger G et al. Dynamic contrast-enhanced MRI of prostate cancer at 3 T: a study of pharmacokinetic parameters. Am J Roentgenol 2007; 189: 849 22 Zelhof B, Lowry M, Rodrigues G, Kraus S, Turnbull L. Description of magnetic resonance imaging-derived enhancement variables in pathologically confirmed prostate cancer and normal peripheral zone regions. BJU Int 2009; 104: 621–7 23 Nakashima J, Tanimoto A, Imai Y et al. Endorectal MRI for prediction of tumour site, tumour size, and local extension of prostate cancer. Urology 2004; 64: 101–5 24 Noworolski SM, Vigneron DB, Chen AP, Kurhanewicz J. Dynamic contrastenhanced MRI and MR diffusion imaging to distinguish between glandular and stromal prostatic tissues. Magn Reson Imaging 2008; 26: 1071–80 25 Kozlowski P, Chang SD, Jones EC, Berean KW, Chen H, Goldenberg SL. Combined diffusion-weighted and dynamic contrast-enhanced MRI for prostate cancer diagnosis – correlation with biopsy and histopathology. J Magn Reson Imaging 2006; 24: 108–13 26 Tanimoto A, Nakashima J, Kohno H, Shinmoto H, Kuribayashi S. Prostate cancer screening: the clinical value of diffusion-weighted imaging and dynamic MR imaging in combination with T2weighted imaging. J Magn Reson Imaging 2007; 25: 146–52 27 Yoshizako T, Wada A, Hayashi T et al. Usefulness of diffusion-weighted imaging and dynamic contrast-enhanced magnetic resonance imaging in the diagnosis of prostate transition-zone cancer. Acta Radiol 2008; 49: 1207–13 28 Schlemmer HP, Merkle J, Grobholz R et al. Can pre-operative contrastenhanced dynamic MR imaging for prostate cancer predict microvessel density in prostatectomy specimens? Eur Radiol 2004; 14: 309–17 29 Josefsson A, Wikstrom P, Granfors T et al. Tumour size, vascular density and proliferation as prognostic markers in GS 6 and GS 7 prostate tumours in patients with long follow-up and noncurative treatment. Eur Urol 2005; 48: 577–83 30 Langer DL, van der Kwast TH, Evans AJ et al. Intermixed normal tissue within prostate cancer: effect on MR imaging measurements of apparent diffusion 2010 THE AUTHORS BJU INTERNATIONAL © 2010 BJU INTERNATIONAL 1417 D E L O N G C H A M P S ET AL. coefficient and T2 – sparse versus dense cancers. Radiology 2008; 249: 900– 8 31 Weinreb JC, Blume JD, Coakley FV et al. Prostate cancer: sextant localization at MR imaging and MR spectroscopic imaging before prostatectomy. Results of ACRIN prospective multi-institutional 1418 clinicopathologic study. Radiology 2009; 251: 122–33 Correspondence: Nicolas Barry Delongchamps, Department of Urology, Hôpital Cochin, 27 rue du Faubourg Saint Jacques, 75014 Paris. e-mail: [email protected] Abbreviations: ADC, apparent diffusion coefficient; AUGC, area under the gadolinium concentration curve; DCE, dynamic contrastenhanced imaging; DWI, diffusion-weighted imaging; PZ, peripheral zone; ROC, receiver operating characteristic; RP, radical prostatectomy; T2W, T2-weighted imaging; TZ, transition zone. © BJU INTERNATIONAL © 2010 THE AUTHORS 2010 BJU INTERNATIONAL