Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
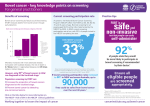
201 Avoca Street Randwick NSW 2031 TE:: (02) 9398 9546 [email protected] I: www.gutfoundation.com.au President: Prof TD Bolin THE OPTIONS FOR IMPROVING THE SUCCESS OF THE NATIONAL BOWEL CANCER SCREENING PROGRAMME. Bowel Cancer is the commonest internal malignancy in Australia, which has one of the highest rates of bowel cancer in the world. There are an estimated 14,234 new cases of bowel cancer and from that 4,047 deaths. This results in 40 new cases diagnosed every day of whom 11 will die because the diagnosis is made too late. The current National Bowel Cancer Screening Program begins at the age of 50 and continues at 5 yearly intervals thereafter. This program has shown that 11.2% of patients aged 40 to 49 with a positive test (patients over 70 excluded) alerts us to the need for screening at an earlier age with the prospect of prevention. Cancer and large polyps bleed though not obviously and the bleeding can be detected by an immunochemical test. The cancers and polyps do not bleed all the time and testing should therefore be done annually. Polyps grow slowly over 5 - 15 years. The screening options for bowel cancer prevention and diagnosis are faecal occult blood testing or colonoscopy. The acceptance rate by patients in the NBCSP declines each year (currently 35%). To improve this rate of acceptance, having screening done through general practitioners has attractions because they already manage other screening programmes. We therefore carried out a screening program in Wagga during 2013 through general practice with no age exclusions. ABN 14 084 315 380 (Incorporated in NSW) In Wagga the rates of positive tests was 14.4% and the age group 40-49 accounted for 25% of all positive tests. Of the 51 patients aged 40-49 in Wagga, 2 had early cancers, 4 large polyps and 4 multiple polyps – all likely to become cancer. Their removal is therefore the key to PREVENTION. We have carried out a cost effectiveness study between the ages of 40 to 70 and comparing annual, biennual FOBT with colonoscopy at the age of 40, 50 and then 5 yearly thereafter. The results indicate that annual FOBT is the most cost effective (costing 149.8 million dollars) with a net benefit of 2.6 billion dollars. This was largely accounted for by trebling of better survival with annual FOBT for (40.9 versus 139.5), fewer deaths with screening (102 versus 309) and a cost effectiveness ratio ($15,719 versus $27,620) See attached table We believe that incorporating colorectal cancer screening through general practice together with screening for breast cancer, diabetes, prostate cancer, hypertension and hyperlipidaemia is a sensible approach. We can predict that there is an increased risk of bowel cancer in only 1 in 5 cancers, this increase being due to family history of polyps or cancer. The other 4 out of 5 have no obvious risk factor with lifestyle factors which include physical inactivity, cigarette smoking, obesity, low fibre intake and low vegetable and fruit intake together with alcohol have significant impact. There is therefore a case to be made for improving dietary advice through general practice which will benefit not only colorectal cancer but also cardiovascular issues. We plan to begin a further study in Port Macquarie under the auspices of the New South Wales Rural Clinical Health School and local general practice to evaluate the success of such an approach. Reducing the screening age to 40 years, has the potential to save 600 lives per year. Professor Terry Bolin The Gut Foundation March 2014 ABN 14 084 315 380 (Incorporated in NSW)