Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Neuropharmacology wikipedia , lookup
Drug interaction wikipedia , lookup
Cell encapsulation wikipedia , lookup
Theralizumab wikipedia , lookup
Nicholas A. Peppas wikipedia , lookup
Gastrointestinal tract wikipedia , lookup
Oral rehydration therapy wikipedia , lookup
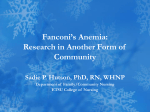
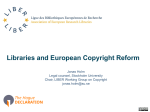
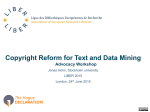
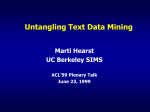
Colonic absorption of salmon calcitonin using tetradecyl maltoside (TDM) as a permeation enhancer Signe Beck Petersena,b, Lisette Gammelgaard Nielsenb, Ulrik Lytt Rahbekb, Mette Guldbrandtb, David J Braydena,* a UCD School of Veterinary Science and UCD Conway Institute, University College Dublin, Belfield, Dublin 4, Ireland; bNovo Nordisk, ADME department, Novo Nordisk park, 2860 Måløv, Denmark *Corresponding author. Tel:. +353 1 7166013; fax: +353 1 7166104 E-mail address: [email protected] 1 Abstract Calcitonin is used as a second line treatment of postmenopausal osteoporosis, but widespread acceptance is somewhat limited by subcutaneous and intranasal routes of delivery. This study attempted to enable intestinal sCT absorption in rats using the mild surfactant, tetradecyl maltoside (TDM) as an intestinal permeation enhancer. Human Caco-2 and HT29-MTX-E12 mucus-covered intestinal epithelial monolayers were used for permeation studies. Rat in situ intestinal instillation studies were conducted to evaluate the absorption of sCT with and without 0.1% w/v TDM in jejunum, ileum and colon. TDM significantly enhanced sCT permeation across intestinal epithelial monolayers, most likely due to combined paracellular and transcellular actions. In situ, TDM caused an increased absolute bioavailability of sCT in rat colon from 1.0% to 4.6%, whereas no enhancement increase was observed in ileal and jejunal instillations. Histological analysis suggested mild perturbation of colonic epithelia in segments instilled with sCT and TDM. These data suggest that the membrane composition of the colon is different to the small intestine and that it is more amenable to permeation enhancement. Thus, formulations designed to release payload in the colon could be advantageous for systemic delivery of poorly permeable molecules. Keywords: salmon calcitonin, oral bioavailability, permeation enhancers, epithelial drug transport, oral peptide delivery, Caco-2 and HT29-MTX-E12 monolayers 2 1. Introduction The 32 amino acid peptide, salmon calcitonin (sCT), is widely used to treat postmenopausal osteoporosis, Paget’s disease, bone associated pain conditions and hypercalcemia (Chesnut, III et al., 2008). Calcitonin is secreted by the parafollicular (C-cells) of the thyroid gland, and in tandem with parathormone (PTH) maintains bone mass by regulating calcium metabolism, through opposing excessive resorption by osteoclasts (Karsdal et al., 2008;de Paula and Rosen, 2010). sCT is currently limited to either parenteral or intranasal administration with interchangeable protection against fracture outcome as a second line treatment in osteoporosis, albeit with 10 fold lower doses required for injection. Intranasal doses of 200IU per day for 12-24 months reduce the risk of new vertebral fractures in postmenopausal woman with osteoporosis (Karsdal et al., 2008; Chesnut, III et al., 2000). Aside from the use in osteoporosis, there is potential for wider use of sCT due to its anti-inflammatory actions and it is being researched as a potential adjunct treatment for osteoarthritis (Maricic, 2012; Nielsen et al., 2011; Manicourt et al., 2006). The oral route would however, be preferred over nasal sCT considering the long-term dosing requirement and potential for nasal irritation, but enzymatic degradation and low intestinal membrane permeability lead to insufficient oral bioavailability in the absence of formulation to address these issues (Lee and Sinko, 2000). Studies examining potential oral delivery of sCT can be found in the literature. An example is the oral formulation with sCT and the Eligen® (Emisphere Corp., USA) carrier, 5-CNAC, which showed greater efficacy in suppression of bone resorption compared to a marketed nasal formulation, but it still failed the primary endpoint in Phase III trial for osteoporosis (Karsdal et al., 2011; Maricic, 2012). An alternative oral formulation is OstoraTM (Unigene/ Tarsa Therapeutics (USA), comprising vesicles of sCT and the peptide-stabilising excipient, citric acid in a pH-dependent Eudragit® L30 D-55 -coated tablet, which completed a Phase III 3 trial (ORACAL) and was superior to nasal sCT and placebo in increasing bone mineral density and reducing bone turnover over 48 weeks; it also appeared to be generally safe and well tolerated despite some intestinal side effects in 50% of subjects (Binkley et al., 2012). Acyl carnitines have been used in Unigene’s oral PTH formulations as permeation enhancers since much higher oral bioavailability will be needed for such peptides compared to sCT (Stern and Gilligan, 1999), while the medium chain fatty acids, sodium caprate and caprylate have been used as enhancers in recent oral peptides delivery clinical trials by others (Maher and Brayden, 2012). Aegis Therapeutics (USA) has developed a delivery system (Intravail®) containing the alkyl maltosides, tetradecyl maltoside (TDM) and/or dodecylmaltoside (DDM) as permeation enhancers that has reached Phase I nasal delivery trials for sCT, parathyroid hormone 1-34, and diazepam (Maggio and Pillion, 2012). In preclinical studies, TDM improved nasal, pulmonary and ocular delivery of insulin and calcitonin (Ahsan et al., 2001; Ahsan et al., 2003). In initial assessments of its potential for use in oral delivery, it enhanced low molecular weight heparin bioavailability following oral gavage in rats (Yang et al., 2005), while studies in mice also showed increased oral delivery of a leptin analogue (Lee et al., 2010) and octreotide (Maggio and Grasso, 2011). Recent mechanistic evaluation of TDM as an intestinal permeation enhancer in rat intestinal mucosae mounted in Ussing chambers by our group found that TDM increased colonic mucosae permeation to flux markers, mannitol and FITC-dextran 4kDa, in the absence of histological damage, whereas remarkably, there was no increase across jejunal mucosae (Petersen et al., 2012). Paracellular and transcellular paths across colonic epithelia were exploited by TDM, as evidenced from in vitro high content analysis and tissue histopathology, in keeping with TDM’s designation as a mild nonionic surfactant. The aim of the current study was, therefore, was to replace flux markers with 4 a peptide, sCT, and to examine regional intestinal absorption in the presence of TDM using rat in situ instillations of jejunal, ileal and colonic regions as well as in two different types of human intestinal epithelial monolayer systems. In doing so, we attempted to study in vitro-in vivo relationships of the effects of TDM and to assess its mechanism of action in detail in separate bioassay systems. Human Caco-2 and mucus-covered HT29-MTX-E12 (E12) monolayers were used to assess whether TDM could increase the permeability of sCT in vitro. Furthermore, the impact of the mucus layer on permeation of sCT and 3H-mannitol were tested in E12 monolayers incubated with the mucolytic, n-Acetyl Cysteine (NAC). In situ instillation experiments elucidated whether TDM was an effective intestinal absorption enhancer for sCT absorption in different segments of the rat intestine; jejunum, ileum and colon. To assess whether TDM causes damage to intestinal epithelia in vitro, TDM was evaluated by lactate dehydrogenase (LDH) assay in Caco-2 and E12 monolayers. Furthermore, tissues from the in situ experiments were assessed histologically in order to seek any relationship between permeability increases and potential cytotoxicity. The hypothesis therefore was that TDM may have potential as a non-toxic colonic permeation enhancer for poorly permeable peptides and that it can eventually be converted from nasal formulations in the clinic to controlled release oral ones. 2. Materials and methods 2.1 Cell culture Human intestinal epithelial Caco-2 cells (p31-48) and E12 cells (p51-55) were grown in DMEM with L-glutamine (2mM) (Lonza, Switzerland), 1%v/v nonessential amino acids (Gibco, Denmark), penicillin (100U)/streptomycin (100g/mL) (Lonza) and 10%v/v fetal 5 bovine serum (Gibco) on 75 cm2 tissue culture flasks at 95% O2/ 5% CO2 at 37C in a humidified environment and split when 80-90% confluence was reached. Caco-2 cells were seeded at a density of 1x105 cells/well on 12 mm Transwells® (polycarbonate, pore size 0.4m) (Corning Costar Corp., USA) and grown for 21 days in DMEM with media change every second day (Hubatsch et al., 2007). E12 cells were seeded at a density of 1 x105 cells/well and cultivated for 14-16 days (Behrens et al., 2001). TEER was measured before experiment start and at the conclusion of the 60 min sCT transport studies using a Millicell®ERS-2 Epithelial Volt-Ohm Meter (Millipore, USA). 2.2 Permeability of 3H-mannitol and sCT across monolayers Permeability of sCT (ChemPrep Inc., FL, USA) and 3H-mannitol (Perkin Elmer, USA) were measured on Caco-2 and E12 monolayers. The donor-side apical concentration of sCT used was 25µM and contained TDM concentrations; 0.01, 0.05 and 0.1% w/v. The apical concentration of 3H-mannitol was 0.8 Ci/mL. Transport experiments on E12 cells were carried out in the presence and absence of 10mM NAC (Sigma-Aldrich, Denmark) added 15 min prior to sCT (Keely et al., 2005) in order to evaluate the influence of the mucous layer on TDM’s enhancing abilities. Transport buffer consisted of HBSS (Gibco), 25mM HEPES (Gibco) and 0.1% w/v BSA (Sigma-Aldrich). BSA was added to prevent sCT adhesion to plastic (Torres-Lugo et al., 2002). Before transport experiments, DMEM media was changed to HBSS (0.4 mL apical side; 1 mL basolateral) and left to equilibrate for 60 min before test solution was added. Basolateral samples of 200L were taken every 15 min over 60 min, while an apical sample of 10L was taken at time zero. 50L of the basolateral sample was used for sCT EIA analysis and 50L was used for 3H-mannitol analysis. The apical sample was diluted 20000 and 50 times before sCT and 3H-mannitol analysis, respectively. Apical and basolateral samples containing 3H-mannitol was mixed with 100µL scintillation fluid 6 and read in scintillation counter (Packard TopCount NTX). Papp values for sCT and 3Hmannitol were calculated according to the following equation: Papp= (dQ/dt) (1/A*C0) where dQ/dt is the flux, A is the surface area exposed (1.12 cm2) and C0 is the starting concentration of sCT or 3H-mannitol. Papp was expressed as diffusion of solutes per second (cm/s). N numbers in Transwell® experiments refer to independent replicates from separate studies. For in vitro sCT permeation, apical and basolateral samples were analysed using an sCT EIA (Phoenix Pharmaceuticals, Inc., CA, USA). Standards were made from the sCT test solutions in the used HBSS transport buffer with the following concentrations; 25000, 10000, 4000, 1600, 640, 256, 102 and 0 pM. The standard curve was used to calculate the sCT concentration in the apical and basolateral compartments. 2.3 Monolayer LDH release Apical samples (50µL) from sCT transport studies on Caco-2 and E12 monolayers were withdrawn after 60 min to test for LDH release. LDH assay was performed in accordance with manufacturer’s guide, where positive controls were created by adding lysis buffer from the kit to a set of control wells and incubating for 20 min (CytoTox-ONETM Homogeneous Membrane Integrity Assay, Promega, USA). 2.4 In vivo rat intestinal instillation 2.4.1 Animals Experimental protocols using the in situ instillation rat model were approved by the University College Dublin (UCD) Animal Research Ethics Committee and carried out at 7 UCD Biomedical Facility under a license obtained from the Irish Department of Health and Children. Additional studies were carried out at Novo Nordisk animal facility under a protocol approved by the Animal Experiments Inspectorate, Ministry of Justice, Denmark. Adult male Wistar rats (approx. 300-400g) were purchased from either Charles River Labs, UK or Taconic, Europe, and housed under controlled environmental conditions regarding humidity and temperature with a 12:12 h light/dark cycle. The rats received tap water and standard laboratory chow ad lib. All studies were carried out in adherence with the “Principles of Laboratory Animal Care,” (NIH Publication #85-23, revised in 1985). 2.4.2 Rat intravenous injection of sCT Rats were anaesthetised by the sub-cutaneous route (s.c) with a Hypnorm®-Dormicum® 1:1 mixture (2ml/kg). Anaesthesia was maintained at a dose of 1ml/kg s.c every 30-40 min during catheter surgery and the 4 h experiment. Separate catheters were inserted 2-3cm into right jugular vein and left carotid artery and rats were placed on a heating pad to maintain body temperature. Following i.v. dosing of sCT (20µg/kg, ChemPrep Inc., FL, USA), 200-400µL aliquots of blood were retrieved via the arterial catheter at 0, 5, 15, 30, 60, 120, 180 and 240 min. Blood samples were centrifuged at 6000 rpm for 5 min at 4C, and serum was aliquoted for sCT analysis and stored at -20C until assayed. Rats were subsequently euthanized with CO2. 2.4.3 Rat intestinal instillation Intestinal instillations with sCT and TDM (0.1% w/v) were modified from an in situ closeloop instillation protocol (Sugita et al., 2007). Rats were given 5% glucose water for 2 days before experiments start and fasted for 18 hours. They were anaesthetised by intraperitoneal (i.p.) injection of ketamine (75mg/kg) and xylazine (10mg/kg) and placed on a heating pad to 8 maintain body temperature. Anaesthesia was maintained by inhalation of isoflurane (1-2%) vaporised in oxygen and administered at a flow rate of 1L/min. sCT was dissolved in PBS with or without 0.1% w/v of TDM. Following a midline laparotomy, sCT (400g/kg)containing solutions were injected using a 30G micro-syringe into the surgically-exposed proximal jejunum, ileum (the 2-3 cm before cecum) or distal colon. Following instillation, blood 200-400L was sampled from the orbital vein at 0, 5, 15, 30, 60, 120, 180 and 240 min. Serum samples were prepared for analysis as described above. Rats were euthanized by injecting 0.5mL Euthatal® into either the heart or the tail vein. Following euthanasia, the intestinal segments were excised and placed in 10% (v/v) buffered formalin for histology. 2.5 sCT and calcium analysis Serum samples were analysed for sCT using EIA kits from Bachem Corp. and Phoenix Phamarceuticals (USA). Both EIA’s were performed as recommended in the manufacturer’s guides, but with minor modifications for the latter: 10µL sample was mixed with 40µL EIA buffer and the EIA plate was incubated at 4ºC overnight to increase sensitivity. Standards were made from pooled male Wistar rat serum (SeraLab, UK) in the presence of sCT (ChemPrep Inc., FL., USA). The rationale for use of two different EIA kits for serum samples was that 10-fold lower serum volumes could be used for the Phoenix assay and it also had a wider linear concentration range. The Bachem EIA had greater sensitivity at low pM concentrations, which the Phoenix assay could not detect. Samples from instillations was analysed using the Bachem EIA in order to cater for very low serum sCT concentrations, while samples following i.v. administration were analysed with the Phoenix EIA, where interrat variation was less at higher serum sCT concentrations. Pharmacokinetic (PK) data was plotted as meanSEM after subtraction of the individual sCT concentration at time zero. The peak sCT concentration (Cmax), the time to reach max (tmax), area under the curve (AUC) and 9 half-life (t½) were calculated using WinNonLin® 5.3, noncompartmental analysis (PharSight Corporation, USA). The absolute bioavailability (F) of sCT was calculated: F (%) = (AUC04h*Di.v./AUCi.v.*Dinst) *100, where AUC0-4h was the area under the sCT serum concentration curve between 0 and 4 h and AUVi.v was the area under the sCT serum concentration curve after i.v. administration (20g/mL). I.V. data was fitted to a two-compartment model using WinNonLin®, from which initial serum () - and terminal () t½ were determined, and these values were used to deconvolute the colonic instillation data. Serum calcium was analysed with a Randox Laboratory clinical chemistry analyser (Ryan et al., 2009). 2.6 Histology Following instillation studies, intestinal tissues were placed in 10% (v/v) buffered formalin for at least 48 hours. Tissues were processed and stained with hematoxylin & eosin (H&E), alcian blue and neutral red. The slides were scanned in 20X scanning mode on a NanoZoomer 2.0-HT (Hamamatsu) and viewed at 20X. 2.7 Data analysis Statistical analysis was carried out using Prism-5® (GraphPad®, San Diego, USA). Two-tailed unpaired Students t-tests were used for comparison. Results are presented as the mean ± standard error of the mean (SEM). A significant difference was considered if p<0.05. 3. Results 3.1 Effects of TDM on TEER and permeability across Caco-2 and E12 monolayers Caco-2 and E12 monolayers were exposed to three different concentrations of TDM (0.01, 0.05 and 0.1% w/v) to assess effects on apical-to-basolateral side fluxes of 3H-mannitol and sCT over 60 min. Mean basal TEER values were 971 Ω.cm2 for Caco-2 monolayers (n=3, 10 each in triplicate), 1009 Ω.cm2 for E12 monolayers (n=4), and 1026 Ω.cm2 for E12 after preincubation with 10mM NAC (n=2). TEER values were significantly decreased for each TDM concentration in Caco-2, E12 and in E12 monolayers exposed to NAC at 60 min compared to controls (p<0.01 for 0.01% TDM, p<0.0001 for 0.05 and 0.1% w/v TDM). TEER decreased across both Caco-2 monolayers and E12 monolayers by 32%, 78% and 81% and by 51%, 74% and 74%, respectively in the presence of 0.01, 0.05 and 0.1% w/v TDM compared to initial values. For E12 monolayers exposed to 10mM NAC for 15 min, TEER decreased by 53%, 72% and 73% for 0.01, 0.05 and 0.1% w/v TDM. Papp values for both sCT and 3H-mannitol on Caco-2 monolayers and E12 monolayers revealed concentration-dependent increase in the presence of TDM (Fig. 1). This was reflected in increased enhancement ratios (Fig. 1e,f), noting slightly higher ratios for the E12 monolayers than the Caco2 monolayers. 0.05% w/v TDM statistically increased the Papp for sCT and 3H-mannitol by ~50% and by 10-20%, across E12 and Caco-2 monolayers respectively. The mean basal Papp for sCT on Caco-2 monolayers was 7.8 x10-8 cm/s, within the range of previous reports (Song et al., 2005;Youn et al., 2006), while it was 6.5 x10-8 cm/s for E12 monolayers. These values are consistent with very low paracellular permeation. The mean basal Papp for 3H-mannitol was 1.1 x10-6 cm/s for Caco-2 monolayers while it was 6.2 x10-7 cm/s for E12. The Papp values for sCT and 3H-mannitol across E12 monolayers preincubated with 10mM NAC for 15 min before addition of TDM concentrations were comparable to those in E12 monolayers in the absence of NAC; the mucolytic had no effect on flux (Fig. 2a,b). While, enhancement ratios with TDM application were higher for sCT in NAC-treated versus untreated E12 monolayers, this reflects a slightly lower basal Papp in the former and absolute values were not different. Similarly, [3H]-mannitol Papp enhancement ratios were unaffected by NAC in E12 monolayers (Fig. 2c) and basal values were similar in 11 the presence and absence of NAC. TDM was therefore an effective permeation enhancer for mannitol and sCT in both in Caco-2 monolayers as well as in mucous covered E12 monolayers. 3.2 Assessment of toxicity on Caco-2 and E12 monolayers Cytotoxicity induced by TDM following 60 min flux studies in Caco-2, E12 and E12 monolayers exposed to NAC was assessed by LDH release. LDH release from the apical side of the Caco-2 monolayers showed a significant increase in the presence of TDM (Fig. 3), which correlated with data from the MTT (3-(4,5-Dimethylthiazol-2-yl)-2,5diphenyltetrazolium bromide) assay in Caco-2 cells (Petersen et al., 2012). LDH release from the apical side of the E12 monolayers also revealed a significant increase for all TDM concentrations (Fig. 3), whereas application of NAC did not change the LDH release profile. LDH release was significantly higher in the Caco-2 cell monolayers than the E12 monolayers at most TDM concentrations, suggesting that the mucus layer provides some protection (Fig. 3). The key data was that 75% cell death was seen with 0.05% w/v TDM at 60 min in Caco-2 and E12 monolayers, the same concentration that induced large Papp changes for sCT and [3H]-mannitol. This would infer that the two processes are difficult to separate at an in vitro level. 3.3 In situ instillation of jejunum, ileum and colon Fig. 4 shows the serum calcium changes when 400g/kg sCT was administered in the presence and absence of 0.1% w/v TDM to the jejunum, ileum and colon. The decrease in calcium levels following sCT administration to the three segments were not statistically significant different between sCT and sCT in the presence of TDM, however there were clear reductions in levels in both formats in all three tissues compared to PBS controls. Serum 12 calcium levels were however, statistically reduced in the presence of TDM at time 60 min time point compared to sCT alone in colonic instillations (p 0.05). Overall, with this exception, the pharmacodynamic effects on serum calcium in the three regions were equivalent for TDM on sCT action, confirming the limitations of this assay as a discriminating tool for sCT formulation screening. PK parameters (Cmax, Tmax and AUC) derived by non-compartmental analysis (NCA) for serum [sCT] following instillations are shown (Table 1). The mean AUC for rats administered sCT by the i.v. route was 667743±45275 min.pM, and this was used to calculate absolute bioavailability (F) for instillations. No statistical PK differences were seen however when sCT was instilled to jejunal and ileal segments in the presence and absence of 0.1% TDM (Fig. 5b, c). The absolute bioavailability (F) for sCT in the absence and presence of TDM for jejunal and ileal instillations was also very low and not different (Table 2), hence there was no statistical difference in AUC of jejunal and ileal sCT instillation in the presence and absence of TDM and the relative F was therefore not calculated. Importantly, there was a statistical increase in AUC upon colonic instillation of sCT with 0.1% TDM (Table 1, Fig. 5d) and the relative F for colon administration of sCT in the presence of TDM was 22.5% compared to sCT in its absence. The mean absolute colonic F for sCT was 1.0% (control) and 4.6% in the presence of 0.1% TDM, calculated from the AUC derived by NCA in WinNonLin® (Table 2). Performing model fitting in WinNonLin® of i.v. data; the i.v. data fitted a two-compartment model with the macro-constants and determined to 0.13 min-1 and 0.019 min-1 equivalent to and half-life (t½) of 5.3 min and 36.1 min, respectively. A similar t½ () was previous reported in rats (Ryan et al., 2009; Sinko et al., 1995) and dogs (Lee and Sinko, 2000). The derived macro-constants was used to perform deconvolution of colon data in WinNonLin®, which gave a mean absolute F of 1.4% and 5.1% in the absence and presence of TDM, 13 respectively, correlating well to the absolute F derived from the colonic AUC’s and calculated absolute F by NCA. Deconvolution revealed that the maximum absorption rate was at 5 min. The harmonic mean of the apparent t½ for administration in colon was 22.5 min (range 13.751.5) in the absence of TDM and 20.9 min (range 12.2-109.0) in the presence of 0.1% w/v TDM, as calculated by NCA. This was not statistically different from the apparent t½ of 29.2 min detected following i.v. administration, also calculated byNCA. Furthermore, it was not statistically significant from the terminal t½ () derived by fitting i.v. data to a twocompartment (by NCA). Unlike the calcium serum assay, PK data therefore confirmed that both basal sCT absorption and the permeation enhancing effects of TDM on sCT absorption were substantially increased in the colon compared to small intestinal regions. 3.4 Histology data Colonic mucosae were assessed for gross histology in the presence and absence of 0.1% w/v TDM after 4 h instillation. Colonic tissue exposed to sCT without TDM generally appeared as healthy intestinal mucosa, whereas TDM-exposed tissue showed mild oedema and evidence of cell sloughing to a varying degree (Fig. 6). Some mucous secretion within the colonic segments was also observed, corresponding well with results from rat isolated colonic mucosae used in Ussing chambers (Petersen et al., 2012). These data suggest that the cytotoxicity data seen for TDM in intestinal epithelial cell lines is much exaggerated over that detected in the intestine in vivo and that histology data in tissue is more relevant and reliable. 4. Discussion Attempts to formulate an oral sCT as a second line treatment for osteoporosis have been made without success for over 20 years. Typically, very low oral bioavailability has been reported, but even 1% would be of the same order as current nasal sCT products (Illum, 2012; Grant 14 and Leone-Bay, 2012), and this seems to be the case in the recent Phase III ORACAL trial for Ostora™ where primary end-points were met (Binkley et al., 2012). Our data suggests that incorporation of alkyl maltoside permeation enhancers that work selectively in the colon may increase oral bioavailability of sCT over approaches aimed at the small intestine. This has not been shown before. The Unigene/Tarsa oral sCT formulation that completed Phase III releases the protected peptide in the duodenum as the pH rises. Even though basal sCT permeability is lower there than in colon and despite relatively low sCT bioavailability, it may still compete with marketed nasal counterparts. Unigene/Tarsa’s oral sCT formulation contains citric acid incorporated in vesicles with the peptide primarily in order to protect it from small intestinal peptidases, which have sub-optimal activity at acidic pH values. These vesicles are then entrapped in a capsule with a pH-dependent coating designed to release in the duodenum. The formulation does not contain an enhancer unlike their PTH formulations, which contain lauroyl carnitine (LeCluyse et al., 1991; Mehta, 2010). This is because a much higher oral bioavailability is required for PTH than for sCT. The low nasal bioavailability seen with the highly potent licenced peptides means that there is substantial waste that would not be acceptable for other peptides. Therefore, there is a search on for effective epithelial enhancers with potential for both nasal and oral peptide delivery as these would increase the range of less potent peptides that could be formulated. Our approach was therefore to examine whether one of the main alkyl maltosides present in the Intravail® technology may be leveraged from nasal delivery to a colonic delivery application. We were also influenced by recent studies showing that Intravail® could increase the oral bioavailability of octreotide and a leptin-like peptide in mice (Lee et al., 2010; Maggio and Grasso, 2011). In addition, our in vitro data revealed that TDM increased fluxes of [14C]mannitol and FD-4 across isolated rat colonic but not small intestinal mucosae and moreover, 15 the enhancement caused by the non-ionic detergent was at concentrations well above its critical micelle concentration (Petersen et al., 2012). This led to the current study where we placed the emphasis on rat in vivo instillations in different intestinal regions with sCT. Firstly, we showed that TDM increased the Papp value of sCT across Caco-2 and mucuscovered E12 monolayers in a concentration-dependent fashion and these data matched the pattern seen for [3H]-mannitol. Basal sCT Papp values across Caco-2 monolayers corresponded well with previous studies (Song et al., 2005; Torres-Lugo et al., 2002; Youn et al., 2006), and the TDM-induced concentration-dependent increase in the [3H]-mannitol Papp value across Caco-2 cell monolayers matches previous findings (Petersen et al., 2012; Yang et al., 2005). Since TEER reductions were seen in parallel, this supported an initial conclusion that the effect was paracellular. Such a conclusion was somewhat invalidated by LDH release assay cytotoxicity results showing substantial cell death during 60 min incubation at the same concentrations of TDM that increased Papp values. These findings are consistent with the nonionic surfactant properties of TDM, which lead to reductions in plasma membrane potential and mitochondrial membrane potential in Caco-2 cells following short-term exposure (Petersen et al., 2012). Papp values for sCT and [3H]-mannitol across E12 monolayers in which mucus was removed by NAC (Keely et al., 2005) were very similar to values obtained in E12 and Caco-2. While this was in keeping with reports that mucus produced by other HT29MTX sub-clones is not a major hindrance to either hydrophilic or hydrophobic drug diffusion across the epithelium (Pontier et al., 2001), data from other mucus-covered HT29-H subclones suggested that the mucus elaborated by that line prevented flux of the highly lipophilic molecule testosterone (Karlsson et al., 1993). In sum, the in vitro data indicated that mucous lying above the E12 monolayers did not prevent the permeation-enhancement effects of TDM and that in vivo effects in the intestine should similarly not be influenced. 16 In vitro Caco-2 cell LDH data raised a concern that toxicity and permeation enhancement might be intimately related, however LDH release from isolated colonic mucosae exposed to the same concentrations of TDM for 60 min was not as high (Petersen et al., 2012), compared to observations in Caco-2 monolayers. This was further supported by gross histology of TDM-exposed tissue from the in situ instillation experiments where, although some cell sloughing and mild oedema was seen, the epithelial barrier was still intact. That Caco-2 cell cytotoxicity studies overestimate actual intestinal tissue damage by enhancers is well established (Aungst, 2012). The likely reason is the lack of capacity for in vitro models to rapidly repair in the face of damage compared to in vivo (Cano-Cebrian et al., 2005;Maher et al., 2009). In sum, despite the caveat on cytotoxicity, the in vitro data demonstrating sCT permeation enhancement in the presence of TDM supported the carrying out of in vivo studies. In situ instillations to different rat intestinal regions proved that TDM acts selectively in the colon to increase sCT absorption and this confirmed the flux data for the presence of TDM in rat intestinal tissue mucosae mounted in Ussing chambers (Petersen et al., 2012). Basal absorption of sCT was significantly higher across the in situ colon compared to other regions. Others demonstrated an increased hypocalcemic effect of sCT in rats after intra-colonic administration in a PEGylated format compared intra-jejunal instillation of the same formulation (Mansoor et al., 2005). A very low absolute F of 0.02% was also reported following rat intra-duodenal administration of sCT (Sinko et al., 1995). This suggests that permeability to small hydrophilic molecules is inherently increased across colon compared to the small intestine. Others report that the effectiveness of the related dodecyl maltoside (DDM) as an enhancer was in the order: rectum > colon > ileum > jejunum, where little 17 absorption was detected (Murakami et al., 1992;Fetih et al., 2005), so it would seem that there is a class effect for alkyl maltosides relating to large intestine permeability enhancement. Even though the colonic mucosa seems to be generally more responsive to permeation enhancers than ileal and jejunal regions (Maroni et al., 2012), some agents are effective in the small intestine. An example is sodium caprate, which is a component of several peptide formulations designed to release payload in the small intestine (Maher et al., 2009). The small intestine must withstand regular exposure to 30mM bile salts and mixed micelles in the fed state, so it requires a high level of structural robustness compared to colon. There are also lower fluid volume and longer residence times in colon, along with potential solvent drag effects, which may favourably impact permeability (Maher and Brayden, 2012). In general, the level of proteolysis in the colon of humans are lower than that in the small intestine (Gibson et al., 1989) and this may in part explain why sCT has a shorter t½ in jejunal fluid than in colonic (Mansoor et al., 2005). On the other hand, proteases originating from bacterial fauna are found selectively in the colon (Gibson et al., 1989) and human CT was still susceptible to degradation in rat caecal contents (Tozaki et al., 1997). In the Ussing chamber studies demonstrating colon-specific effects of TDM and DDM (Petersen et al., 2012), stability was not an issue for [3H]-mannitol or FD-4 and this would suggest that a difference in membrane composition between jejunum and colon relating to fluidity is the most important differentiating factor. Placing the in situ colonic sCT bioavailability in context, the absolute F value of 4.6% achieved with 0.1% TDM appears impressive, although it must be emphasised that regional intestinal instillations do not factor in potential losses during GI transit or the impact of dilution for an oral formulation. Therefore, this is the best data that can be detected in rats if 18 sCT and TDM could be reliably protected, delivered and released together in the colon in a controlled release formulation. Still, enteric-coated sCT capsules for small intestinal delivery have achieved an absolute F of up to 1.8% after oral administration to rats (Wu et al., 2010), so the current data would suggest that this can be improved upon by targeting the colon and using an appropriate enhancer. A colonic F for sCT approaching 5% would be significantly higher than current nasal formulations and other oral formulations in clinical trials targeted at the jejunum and ileum. Finally, there is the question of how to compare serum calcium data in response to sCT. The calcium decrease seen with sCT and TDM did not show any significant difference compared to native sCT at a dose of 400 µg/kg in any region, except at 60 min in the colon. The calcium decrease of 20-30% seen in all intestinal segments was in the range of previous reports following s.c., intrajejunal and intracolonic administration of sCT in rats (Cheng and Lim, 2009;Cetin et al., 2008;Wu et al., 2010;Mansoor et al., 2005). A maximum hypocalcemic threshold level exists due to calcium homeostasis and moreover, even i.v. dosing of sCT does not induce serum calcium decreases in a strict dose-dependent fashion (Ryan et al., 2009;Mansoor et al., 2005;Cheng and Lim, 2009). Profound elevations in serum sCT are not accompanied by major hypocalcaemia, since low levels of calcium will lead to a rebound in PTH secretion, which acts on kidney and bone to mobilise plasma calcium levels (Friedman, 2011). A stabile circulating calcium level is vital for the electrophysiological performance of most cells and consequently, a self-regulating system with several interacting hormones exists (de Paula and Rosen, 2010). As a read-out, serum calcium reductions in response to oral sCT can therefore provide useful information as to whether the peptide is bioactive in the intestine, however they provide no insight into rank ordering effective formulations and consequently PK data is what should be relied upon. 19 5. Conclusion In summary, for the first time TDM proved to be effective as an intestinal permeation enhancer for sCT across Caco-2 and E12 monolayers. In rat in situ instillations, TDM preferentially increased absorption of sCT in the colonic region of the intestine compared to proximal jejunum or ileum. Importantly, in contrast to in vitro cytotoxicity studies, in vivo toxicity assessment confirmed a wide margin between doses of TDM that induce permeation and those which damage tissue. These novel data indicate that oral peptide formulations utilizing TDM as an absorption enhancer may potentially be developed to target the colonic region for improved systemic bioavailability. Acknowledgements Novo Nordisk A/S supported for the post-doctoral fellowship of SBP. Additional support was from Science Foundation Ireland grant Number 07/SRC/B1154 (The Irish Drug Delivery Network). Thanks to Ms. Margaret Coady for assistance with tissue histology and to Tanira Aguirre for assistance with instillations, both at UCD. Also thanks to Sebastian Beck Jørgensen, Kent Emil Pedersen and Helle Andersen for assistance with i.v. rat studies, and to Christian Rosenquist and Susanne Halkier for discussion on the sCT EIA, and to Flemming Seier Nielsen for discussion and interpretation of WinNonLin® data (all at Novo-Nordisk). 20 Figure legends Fig 1. Papp of [3H]-mannitol and sCT across Caco-2 and E12 monolayers with TDM (0.01, 0.05 and 0.1% w/v). (a) Caco-2: Papp [3H]-mannitol, (b) E12: Papp [3H]-mannitol, (c) Caco-2: Papp sCT, (e) E12: Papp sCT, (e) Caco-2 enhancement ratios versus controls in the absence of TDM, (f) E12 enhancement ratios versus controls in the absence of TDM. (n=3 for Caco-2 and n=4 for E12). Fig 2. Papp of [3H]-mannitol and sCT across E12 monolayers incubated with NAC (10 mM) and TDM (0.01, 0.05 and 0.1% w/v). (a) Papp [3H]-mannitol, (b) Papp sCT, (c) enhancement ratios versus controls in the absence of TDM. (n=2). Fig 3. LDH release after 60 min exposure of Caco-2 and E12 monolayers with TDM. Caco-2 monolayers (n=3), E12 monolayers (n=3), E12 monolayers with 10mM NAC (n=2). LDH release by lysis buffer was set to 100%. P < 0.001 for 0.01% TDM; P < 0.0001 for 0.05 and 0.1% TDM versus untreated controls; P < 0.05 between Caco-2 and E12 monolayers for 0.01% and 0.05% w/v. Fig 4. Serum calcium decrease in % of initial value for rat sCT instillation studies. (a) Jejunum, (b) Ileum and (c) Colon. N number as for Fig.5. (○) sCT control, () sCT with 0.1% w/v TDM, (□) PBS control (n=2 for each intestinal segment). Fig 5. Serum sCT in rats. (a) i.v. (n=4), (b) Jejunal instillations (n=7 sCT control, n=5 with 0.1% w/v TDM), (c) Ileal instillations (n=5 control, n=6 with TDM), (d) Colonic instillations (n=6 control, n=5 with TDM). (○) sCT solution, () sCT with 0.1% w/v TDM. The i.v. dose of sCT: (20µg/kg); instillation dose: (400µg/kg). 21 Fig 6. Histology of rat colonic tissue after 4 h colonic instillations with sCT (400µg/kg). (a) sCT solution, (b) 0.1% w/v TDM with sCT. Upper panel: H&E; lower panel: alcian blue and neutral red (Bar=200µm). 22 References 1. Ahsan,F., Arnold,J., Meezan,E., Pillion,D.J., 2001. Enhanced bioavailability of calcitonin formulated with alkylglycosides following nasal and ocular administration in rats. Pharm. Res. 18, 1742-1746. 2. Ahsan,F., Arnold,J.J., Yang,T., Meezan,E., Schwiebert,E.M., Pillion,D.J., 2003. Effects of the permeability enhancers, tetradecylmaltoside and dimethyl-beta-cyclodextrin, on insulin movement across human bronchial epithelial cells (16HBE14o-). Eur. J. Pharm. Sci. 20, 27-34. 3. Aungst,B.J., 2012. Absorption enhancers: applications and advances. AAPS J. 14, 10-18. 4. Behrens,I., Stenberg,P., Artursson,P., Kissel,T., 2001. Transport of lipophilic drug molecules in a new mucus-secreting cell culture model based on HT29-MTX cells. Pharm. Res. 18, 11381145. 5. Binkley,N., Bolognese,M., Sidorowicz-Bialynicka,A., Vally,T., Trout,R., Miller,C., Buben,C.E., Gilligan,J.P., Krause,D.S., 2012. A phase 3 trial of the efficacy and safety of oral recombinant calcitonin: The Oral Calcitonin in Postmenopausal Osteoporosis (ORACAL) trial. J.Bone Miner.Res. 27, 1821-1829. 6. Cano-Cebrian,M.J., Zornoza,T., Granero,L., Polache,A., 2005. Intestinal absorption enhancement via the paracellular route by fatty acids, chitosans and others: A target for drug delivery. Curr.Drug Deliv. 2, 9-22. 7. Cetin,M., Youn,Y.S., Capan,Y., Lee,K.C., 2008. Preparation and characterization of salmon calcitonin-biotin conjugates. AAPS PharmSciTech. 9, 1191-1197. 8. Cheng,W., Lim,L.Y., 2009. Lipeo-sCT: a novel reversible lipidized salmon calcitonin derivative, its biophysical properties and hypocalcemic activity. Eur. J. Pharm. Sci 37, 151-159. 9. Chesnut,C.H., III, Azria,M., Silverman,S., Engelhardt,M., Olson,M., Mindeholm,L., 2008. Salmon calcitonin: a review of current and future therapeutic indications. Osteoporos. Int. 19, 479-491. 10. Chesnut,C.H., III, Silverman,S., Andriano,K., Genant,H., Gimona,A., Harris,S., Kiel,D., LeBoff,M., Maricic,M., Miller,P., Moniz,C., Peacock,M., Richardson,P., Watts,N., Baylink,D., 2000. A randomized trial of nasal spray salmon calcitonin in postmenopausal women with established osteoporosis: the prevent recurrence of osteoporotic fractures study. PROOF Study Group. Am. J. Med. 109, 267-276. 11. de Paula,F.J., Rosen,C.J., 2010. Back to the future: revisiting parathyroid hormone and calcitonin control of bone remodeling. Horm. Metab. Res. 42, 299-306. 12. Fetih,G., Lindberg,S., Itoh,K., Okada,N., Fujita,T., Habib,F., Artersson,P., Attia,M., Yamamoto,A., 2005. Improvement of absorption enhancing effects of n-dodecyl-beta Dmaltopyranoside by its colon-specific delivery using chitosan capsules. Int. J. Pharm. 293, 127135. 13. Friedman,P.A., 2011. Hormonal regulation of calcium and phophate homeostasis. In: Brunton,L.; Chabner, B and Knollman, B. .(Ed.), Goodman and Gilman's The Pharmacological Basis of Therapeutics (12th Ed.). The McGraw-Hill Companies, Inc., pp. 1275-1306. 14. Gibson,S.A., McFarlan,C., Hay,S., MacFarlane,G.T., 1989. Significance of microflora in proteolysis in the colon. Appl. Environ. Microbiol. 55, 679-683. 15. Grant, M., Leone-Bay, A., 2012. Peptide therapeutics: it’s all in the delivery. Therapeutic Delivery 3, 981-996. 16. Hubatsch,I., Ragnarsson,E.G.E., Arthursson,P., 2007. Determination of drug permeability and prediction of drug absorption in Caco-2 monolayers. Nature Protocols 2, 2111-2119. 17. Illum,L., 2012. Nasal drug delivery - Recent developments and future prospects. J. Controlled Release161, 254-263. 18. Karlsson,J., Wikman,A., Artursson,P., 1993. The mucus layer as a barrier to drug absorption in monolayers of human intestinal epithelial HT29-H goblet cells. Int. J. Pharm. 99, 209-218. 19. Karsdal,M.A., Henriksen,K., Arnold,M., Christiansen,C., 2008. Calcitonin: a drug of the past or for the future? Physiologic inhibition of bone resorption while sustaining osteoclast numbers improves bone quality. BioDrugs 22, 137-144. 20. Karsdal,M.A., Henriksen,K., Bay-Jensen,A.C., Molloy,B., Arnold,M., John,M.R., Byrjalsen,I., Azria,M., Riis,B.J., Qvist,P., Christiansen,C., 2011. Lessons learned from the development of oral calcitonin: the first tablet formulation of a protein in phase III clinical trials. J. Clin. Pharmacol .51, 460-471. 21. Keely,S., Rullay,A., Wilson,C., Carmichael,A., Carrington,S., Corfield,A., Haddleton,D.M., Brayden,D.J., 2005. In vitro and ex vivo intestinal tissue models to measure mucoadhesion of poly (methaerylate) and N-trimethylated chitosan polymers. Pharm. Res. 22, 38-49. 22. LeCluyse,E.L., Appel,L.E., Sutton,S.C., 1991. Relationship between drug absorption enhancing activity and membrane perturbing effects of acylcarnitines. Pharm. Res. 8, 84-87. 23. Lee,D.W., Leinung,M.C., Grasso,P., 2010. Oral delivery of mouse [D-Leu-4]-OB3, a synthetic peptide amide with leptin-like activity, in male Swiss Webster mice: A study comparing the 24 pharmacokinetics of oral delivery to intraperitoneal, subcutaneous, intramuscular, and intranasal administration. Regul.Pept. 160, 129-132. 24. Lee,Y.H., Sinko,P.J., 2000. Oral delivery of salmon calcitonin. Adv.Drug Deliv.Rev. 42, 225238. 25. Maggio,E.T. & Pillion, D. , 2012. High efficiency intranasal drug delivery using Intravail® alkylsaccharide absorption enhancers. Drug Delivery and Translational Research (In Press). DOI 10.1007/s13346-012-0089-8. 26. Maggio,E.T., Grasso,P., 2011. Oral delivery of octreotide acetate in Intravail« improves uptake, half-life, and bioavailability over subcutaneous administration in male Swiss Webster mice. Regul.Pept. 167, 233-238. 27. Maher, S. and Brayden, D. J, 2012. Overcoming poor permeability: translating permeation enhancers for oral peptide delivery. Drug Discovery Today: Technologies. 9, e113-e119. 28. Maher,S., Leonard,T.W., Jacobsen,J., Brayden,D.J., 2009. Safety and efficacy of sodium caprate in promoting oral drug absorption: from in vitro to the clinic. Adv.Drug Deliv.Rev. 61, 1427-1449. 29. Manicourt,D.H., Azria,M., Mindeholm,L., Thonar,E.J., Devogelaer,J.P., 2006. Oral salmon calcitonin reduces Lequesne's algofunctional index scores and decreases urinary and serum levels of biomarkers of joint metabolism in knee osteoarthritis. Arthritis Rheum. 54, 3205-3211. 30. Mansoor,S., Youn,Y.S., Lee,K.C., 2005. Oral delivery of mono-PEGylated sCT (Lys18) in rats: regional difference in stability and hypocalcemic effect. Pharm. Dev. Technol. 10, 389-396. 31. Maricic,M.J., 2012. Oral calcitonin. Curr Osteoporos Rep 10, 80-85. 32. Maroni,A., Zema,L., Del Curto,M.D., Foppoli,A., Gazzaniga,A., 2012. Oral colon delivery of insulin with the aid of functional adjuvants. Adv.Drug Deliv.Rev. 64, 540-556. 33. Mehta, N, 2010. Clinical development of an oral formulation of recombinant calcitonin. The Peptide Conference 2010. http://www.unigene.com/wpcontent/uploads/2011/09/ClinicalDevofOralsCTPresentation1.pdf. Accessed August 25th. 2012. 34. Murakami,M., Kusanoi,Y., Takada,K., Muranishi,S., 1992. Assessment of enhancing ability of medium-chain alkyl saccharides as new absorption enhancers in rat rectum. Int. J. Pharm. 79, 159-169. 35. Nielsen,R.H., Bay-Jensen,A.C., Byrjalsen,I., Karsdal,M.A., 2011. Oral salmon calcitonin reduces cartilage and bone pathology in an osteoarthritis rat model with increased subchondral bone turnover. Osteoarthritis Cartilage 19, 466-473. 25 36. Petersen, S. B., Nolan, G., Maher, S., Rahbek, U. L., Guldbrandt, M., and Brayden, D. J, 2012. Evaluation of alkyl maltosides as intestinal permeation enhancers: Comparison between rat intestinal mucosal sheets and Caco-2 monolayers. Eur. J. Pharm. Scie. In Press. 37. Pontier,C., Pachot,J., Botham,R., Lenfant,B., Arnaud,P., 2001. HT29-MTX and Caco-2/TC7 monolayers as predictive models for human intestinal absorption: role of the mucus layer. J.Pharm.Sci. 90, 1608-1619. 38. Ryan,S.M., Wang,X., Mantovani,G., Sayers,C.T., Haddleton,D.M., Brayden,D.J., 2009. Conjugation of salmon calcitonin to a combed-shaped end functionalized poly(poly(ethylene glycol) methyl ether methacrylate) yields a bioactive stable conjugate. J. Controlled Release 135, 51-59. 39. Sinko,P.J., Smith,C.L., McWhorter,L.T., Stern,W., Wagner,E., Gilligan,J.P., 1995. Utility of pharmacodynamic measures for assessing the oral bioavailability of peptides. 1. Administration of recombinant salmon calcitonin in rats. J.Pharm.Sci. 84, 1374-1378. 40. Song,K.H., Chung,S.J., Shim,C.K., 2005. Enhanced intestinal absorption of salmon calcitonin (sCT) from proliposomes containing bile salts. J. Controlled Release 106, 298-308. 41. Stern, W. and Gilligan, J. P, 1999. Oral salmon calcitonin pharmaceutical products. Unigene Laboratories Inc. USP 5,912,014. 42. Sugita,Y., Takao,K., Toyama,Y., Shirahata,A., 2007. Enhancement of intestinal absorption of macromolecules by spermine in rats. Amino Acids (Vienna) 33, 253-260. 43. Torres-Lugo,M., García,M., Record,R., Peppas,N.A., 2002. pH-Sensitive hydrogels as gastrointestinal tract absorption enhancers: transport mechanisms of salmon calcitonin and other model molecules using the Caco-2 cell model. Biotechnol.Prog. 18, 612-616. 44. Tozaki,H., Emi,Y., Horisaka,E., Fujita,T., Yamamoto,A., Muranishi,S., 1997. Degradation of insulin and calcitonin and their protection by various protease inhibitors in rat caecal contents: implications in peptide delivery to the colon. J. Pharm. Pharmacol. 49, 164-168. 45 Wu,L., Zhang,G., Lu,Q., Sun,Q., Wang,M., Li,N., Gao,Z., Sun,Y., Li,T., Han,D., Yu,X., Wang,L., Sun,W., Zhao,D., Wu,Y., Lu,Y., Chen,X., 2010. Evaluation of salmon calcitonin (sCT) enteric-coated capsule for enhanced absorption and GI tolerability in rats. Drug Dev.Industrial Pharm. 36, 362-370. 46. Yang,T., Arnold,J.J., Ahsan,F., 2005. Tetradecylmaltoside (TDM) enhances in vitro and in vivo intestinal absorption of enoxaparin, a low molecular weight heparin. J.Drug Targeting 13, 2938. 26 47. Youn,Y.S., Jung,J.Y., Oh,S.H., Yoo,S.D., Lee,K.C., 2006. Improved intestinal delivery of salmon calcitonin by Lys18-amine specific PEGylation: stability, permeability, pharmacokinetic behavior and in vivo hypocalcemic efficacy. J. Controlled Release 114, 334-342. Caco-2 E12 25 (a) *** 20 Papp (cm/sec) (x10-6) *** 15 10 5 0 *** 15 *** 10 5 *** 0. 1% 0. 05 % 0. 01 % C tl 0. 1% 0. 05 % 0. 01 % C tl 0 60 60 (c) Papp (cm/sec) (x10-7) *** *** 40 20 0 (d) *** 40 *** 20 ** (e) 0. 1% C tl 0. 1% 0. 05 % 0. 01 % C tl 0 0. 05 % sCT Papp (cm/sec) (x10-7) (b) 20 0. 01 % [3H]-mannitol Papp (cm/sec) (x10-6) 25 (f) 0.01% 0.05% 0.1% [3H]-mannitol 1.1 14.1 17.0 sCT 2.1 49.7 55.2 27 0.01% 0.05% 0.1% [3H]-mannitol 2.1 17.3 23.1 sCT 4.6 46.8 68.3 Fig. 1 28 Papp (cm/sec) (x10-6) 25 (a) 20 *** 15 *** 10 5 *** 0. 1% 0. 05 % 0. 01 % C tl 0 Papp (cm/sec) (x10-7) 60 (b) *** *** 40 20 ** 0. 1% 0. 05 % 0. 01 % C tl 0 0.01% 0.05% 0.1% [3H]-mannitol 2.3 19.3 24.8 sCT 7.7 92.3 98.1 (c) Fig. 2 150 *** 100 *** *** *** *** *** * * 50 *** *** *** 0. 1% 0. 05 % 0. 01 % on tr ol 0 C %LDH * Fig. 3 Jejunum (a) (b) 110 % drop in [Ca] 110 100 90 80 70 100 90 80 70 0 50 100 150 200 0 50 Time, min. 100 150 200 Time, min. Colon (c) 110 % drop in [Ca] % drop in [Ca] Ileum 100 90 80 * 70 0 50 100 150 200 Time, min. Fig. 4 I.V. Jejunum 80 (a) 15000 (b) sCT [pM] sCT [pM] 60 10000 5000 40 20 0 0 50 100 150 200 0 250 0 50 Time, min. 200 250 200 250 Colon 20000 (c) (d) 15000 sCT [pM] 300 sCT [pM] 150 Time, min. Ileum 400 100 200 10000 5000 100 0 0 0 50 100 150 Time, min. 200 250 0 50 100 150 Time, min. Fig. 5 (a) (b) Fig. 6 33