Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
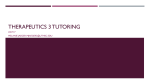
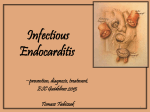
INFECTIVE ENDOCARDITIS and valvular vegetations Alex Yartsev 30/03/2010 Pathological definitions INFECTIVE ENDOCARDITIS • The colonization or invasion of heart valves or the mural endocardium by a microbe VEGETATIONS • Masses of thrombotic debris and organisms, attached to valves or myocardial tissue, and destructive to that tissue Robbins and Cotran Pathologic Basis Of Disease (8th ed) A vegetation Subacute Mitral Endocarditis, Strep viridans Acute endocarditis of congenitally bicuspid aortic valve, by Staph aureus Robbins and Cotran Pathologic Basis Of Disease (8th ed) Acute IE or Subacute IE? • Definition dependent on virulence and course ACUTE: 10-20% of cases • Infection of a normal valve • Rapidly progressing, usually Staph Aureus • Rapidly destructive, necrotising, ulcerative SUBACUTE – 80-90% of cases • Infection of a previously diseased, deformed valve • Slowly progressing, usually Streptococcus • Gradually destructive, more like erosive Robbins and Cotran Pathologic Basis Of Disease (8th ed) There are 3 main pathogens Defective valves: – 60% of cases its Streptococcus viridans Normal valves – Staph Aureus especially if the valve belongs to an IV drug user Prosthetic valves: - Staph epidermitis OTHER ORGANISMS: Enterococci, Haemophilus, Actinobacillus, Cardiobacterium, Eikenella, Kingella… All oral organisms In 10-15% of cases, no organism is found. Robbins and Cotran Pathologic Basis Of Disease (8th ed) A Word About Streptococci • Alpha hemolytic: reduce iron from hemoglobin – Strep pneumoniae, Strep viridans • Beta hemolytic: lysis of whole RBCs – Group A: S.pyogenes rheumatic fever – Group B: S.agalactiae neonatal meningitis – Group C: S.equi “distemper of horses” – Group D: Enterococci – Group G: S.canis dog saliva Predisposing factors FOREMOST: Anything that predisposes to bacteraemia Dental procedures, oral infections,IV drug use, surgery, IV cannulas, central lines, huge obvious infections elsewhere, or minute trivial areas of slightly broken skin Predisposing factors • • • • • • Rheumatic heart disease Mitral valve prolapse Degenerative calcific valvular stenosis NORMAL bicuspid aortic valve Prosthetic valves Unrepaired and repaired congenital defects Robbins and Cotran Pathologic Basis Of Disease (8th ed) Complications • • • • • Brain abscess Lung abscess Heart failure Glomerulonephritis (immune complexes) Emboli anywhere Common clinical Features • Fever, chills, rigors • New heart murmr • New onset of heart failure signs/symptoms Problems otherwise unexplained: • Brain abscesses • Lung abscesses • Glomerulonephritis Uncommon clinical features • Roth spots (Retinal hemorrhages) • Janeway lesions (painless microabscesses ) Oslers nodes (painful immune complex deposits) Robbins and Cotran Pathologic Basis Of Disease (8th ed) Tally and O’Connor Populations at risk • IV drug users: usually tricuspid valve • Valve replacement patients • Patients with repaired or unmanaged septal defects • Past history of rheumatic heart disease Preventative measures • COCHRANE: “There remains no evidence about whether penicillin prophylaxis is effective or ineffective against bacterial endocarditis in people at risk who are about to undergo an invasive dental procedure. “ Diagnosis • Duke criteria: MAJOR citeria – Streptocucus viridans in blood culture – Staph aureus in blood culture in absence of primary focus – Persistently positive blood culture: organism consistent with infective endocarditis from • Blood cultures drawn more than 12 hours apart, or • all of three, or majority of four or more separate blood cultures, with the first and last drawnat least 1 hour apart – Evidence of Endocardial involvement: +ve ECHO Diagnosis: Duke Criteria Need 2 major Or 1 major and 3 minor Or 5 minor criteria • MAJOR CITERIA – Positive blood culture, for a characteristic organism – Echo identification of a valvular mass or partial separation of an artificial valve Diagnosis: Duke Criteria • MINOR CITERIA – – – – – – Predisposing heart lesion IV drug use Vascular lesions eg. splintr hemorrhages or petechiae Immunological phenomena eg. Oslers nodes, Roth spots Single culture positive for an unusual organism Echo findings consistent with but not diagnostic of endocarditis TTE or TOE? • TTE for aortic valve • TOE for mitral, pulmonary, tricuspid • TTE less sensitive for vegetations than TOE Practical Management • • • • Delay of diagnosis = lower survival Three sets of cultures before antibiotics; Then, commence empiric therapy Continue for 6 weeks Ohs Intensive Care Manual 6th ed; Therapeutic Guidelines Empirical antibiotics • Therapeutic Guidelines suggest: – Benzylpenicillin 1.8 g q4h, PLUS – Flucloxacillin 2g q4h PLUS – Gentamicin 6mg/kg daily ALSO – Add Vancomycin if the pt has a prosthetic valve or the infection is hosptial-acquired Good Evidence • COCHRANE: “There remains no evidence about whether penicillin prophylaxis is effective or ineffective against bacterial endocarditis in people at risk who are about to undergo an invasive dental procedure. “ Most people still use ampicillin or clindamycin Antibiotics for the prophylaxis of bacterial endocarditis in dentistry: Oliver et al, 2008