Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
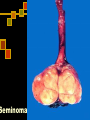
Testicular carcinoma Epidemilogy 90-95% are germ cell Incidence five times higher among white men Most common solid tumor in males ages 15-35 often is in right What is Testicular Cancer? Germ cell tumors (GCT): ~95% of TC Seminomas: most common subtype (~50%); slow growing and radiosensitive Nonseminomas: often occur in third decade; rapid metastasis to lymph nodes and lung Non-Germ Cell Tumors (Non-GCTs) Stromal: ~4% of adult TC Secondary tumors: arise in another organ Risk factor Gonadal Dysgenesis Trauma prompts evaluation Hormones 20-30% develop cancer (gonadoblastoma) DES/OCP probably do not increase risk Atrophy (mumps orchitis) Cryptorchidism: 7-10% of patients with testicular cancer have a history of cryptorchidism Abnormal germ cell morphology Elevated temperature Interference with normal blood supply 5-10% of patients with testicular cancer and a history of cryptorchidism develop cancer in the contralateral testis Orchidopexy does not prevent development of cancer – just allows for detection Clinical manifestation Patients often present with a painless testicular mass Gynecomastia Pain, swelling, or hardness in scrotum a less frequent complaint About 10% report recent testicular trauma Swelling in lower extremities, back pain, cough, or dyspnea may indicate advanced disease 5% germ cell 30-50% Sertoli/Leydig 1-2% have bilateral disease at diagnosis More common on the right Diffrentiated Diagnosis Torsion Epididymitis Epididimoorchitis Hydrocele Hernia Hematoma Spermatocele Syphilitic gumma Work-up Exam U/S CXR +/- Chest CT Abdominal CT Can identify small nodal deposits <2 cm MRI and PET scan no advantage over CT Markers Elevation after orchiectomy generally represents metastatic disease Conversely normalization does not rule out metastatic disease Alpha-Fetoprotein Expressed by the early embryo (also liver and GI tract) Single chain Half-life: 5-7 days Produced by pure embryonal, teratocarcinoma, yolk sac, mixed tumors (NOT pure choriocarcinoma or seminoma) Falsely elevated in liver dysfunction, viral hepatitis Human Chorionic Gonadotrophin Secretory product of the placenta Alpha unit (LH,FSH,TSH) and beta unit Half-life: 24-36 hours Produced by syncytiotrophoblastic tissue All choriocarcinomas, 40-60% embryonal, 5-10% seminoma Falsely elevated in hypogonadism and marijuana use Lactic Acid Dehydrogenase Presents normally in smooth, cardiac and skeletal muscle, liver and brain Most useful in advanced seminoma or tumors where other markers are not elevated Many false positives Testis cancer GERM CELL Seminoma 30-60% Non-seminoma Embryonal 3-4% Yolk sac Teratoma 5-10% Choriocarcinoma 1% Mixed 40% NONGERM CELL Leydig 1-3% Sertoli <1% Gonadoblastoma 0.5% Seminoma: Most common germ cell tumor Pure seminomas never secrete AFP 5-10% secrete HCG (usually classic) At diagnosis: 65-75% confined to the testis 10-15% with regional retroperitoneal nodes 5-10% with advanced juxtorenal or visceral disease Seminoma Classic 82-85% Anaplastic 5-10% Age 30s Islands /sheets of cells with syncytiotrophoblasts (5-10%) Stage for stage no different than classic Spermatocytic 2-12% Low metastatic potential Older population (>50) 6% bilateral Emberional Peak age 25-35 May secrete both AFP and B-HCG Metastatic deposits usually contain teratoma (80%) Yolk Sac (Infantile embryonal) Peak age: infants and children Also may spread hematogenously Secretes AFB and B-HCG Embryoid bodies (Schiller-Duvall bodies) resemble 1-2 week old embryos surrounded by syncytiotrophoblasts and cytotrophoblasts Choriocarcinoma Peak age 20-30 Worst prognosis of all testis tumors Hematogenous spread (especially to lungs) Always secrete B-HCG Teratoma Peak age 25-35 Poor response to chemotherapy and XRT Pure forms should not secrete AFB or B-HCG Can arise from malignant transformation after chemotherapy for NSGCT Contains all 3 germ layers in the mature form and is undifferentiated in immature form TNM Staging of Testicular Tumour T0 T1s T1 T2 = = = = T3 = T4 = No evidence of Tumour Intratubular, pre invasive Confined to Testis Invades beyond Tunica Albuginea or into Epididymis Invades Spermatic Cord Invades Scrotum N1 = N2 = N3 = Multiple< 5 node/Single < 2 cm Multiple < 5 node / Single 2-5 cm Any node > 5 cm PRINCIPLES OF TREATMENT Treatment should be aimed at one stage above the clinical stage Seminomas Radiotherapy. Non-Seminomas are Radio-Resistant and best treated by Surgery Advanced Disease or Metastasis - Responds Radio-Sensitive. well to Chemotherapy Treat with PRINCIPLES OF TREATMENT Radical INGUINAL ORCHIDECTOMY is Standard first line of therapy Lymphatic spread initially goes to RETRO-PERITONEAL NODES Early hematogenous spread RARE Bulky Retroperitoneal Tumours or Metastatic Tumors Initially “DOWN-STAGED” with CHEMOTHERAPY Treatment of Seminomas Stage I, IIARadical Inguinal Orichidectomy followed by radiotherapy to Ipsilateral Retroperitonium & Ipsilateral Iliac group Lymph nodes (2500-3500 rads) Bulky stage II and III Seminomas Radical Inguinal Orchidectomy is followed by Chemotherapy Treatment of Non-Seminoma Low Grade RADICAL ORCHIDECTOMY followed by RETROPERITONEAL LYMPH DISSECTION High Grade: Initial CHEMOTHERAPY followed by SURGERY for Residual Disease Radical Orchiectomy Survival at 5 years Seminoma Stage I Stage II A Stage II B-III Non-seminoma 98% 96-100% 92-94% >90% 33-75% 55-80% NON_GERM CELL Leydig Cell 1-3% of all testis tumors Bimodal age distribution: ages 5-9 and 25-35 Bilateral in 5-10% No association with cryptorchidism Prepubital children may present with virilization and elevated urinary 17-ketosteroid levels; adults are usually asymptomatic (25% gynecomastia) Treatment: radical orchiectomy and RPLND for malignant tumors (10% malignant) Sertoli Cell Less than 1% of all testicular tumors Bimodal age of distribution: < 1 year and 20-45 years old 10% lesions are malignant Virilization seen in children and gynecomastia in adults Treatment: Radical orchiectomy with RPLND in malignant disease Gonadoblastoma 0.5% of testicular tumors Seen in patients with gonadal dysgenesis 4/5 patients are phenotypic females with streak gonads Treatment: Radical orchiectomy with gonadectomy of the contralateral gonad (bilateral in 50%) Secondary testicular tumor Lymphoma Large without pain 50% bilatral ¼ with systemic symptom treatment: radical orciectomy+chemotherapy Leukemia: in 50% bilatral Dx : biopsy Metastatic tumor: very rarely source: prostat lung GI melanoma kidney