Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
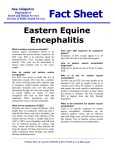
Neurocrit Care DOI 10.1007/s12028-013-9822-5 PRACTICAL PEARL Successful Management of Severe Neuroinvasive Eastern Equine Encephalitis Linda C. Wendell • N. Stevenson Potter Julie L. Roth • Stephen P. Salloway • Bradford B. Thompson • Ó Springer Science+Business Media New York 2013 Abstract Background Eastern Equine Encephalitis (EEE) virus is an arbovirus that mostly causes asymptomatic infection in humans; however, some people can develop a neuroinvasive infection associated with a high mortality. Methods We present a case of a patient with severe neuroinvasive EEE. Results A 21-year-old man initially presented with headache, fever, and vomiting and was found to have a neutrophilic pleocytosis in his cerebrospinal fluid. He eventually was diagnosed with EEE, treated with high-dose methylprednisolone and intravenous immunoglobulin. His course in the NeuroIntensive Care Unit was complicated by cerebral edema and intracranial hypertension, requiring osmotherapy, pentobarbital and placement of an external ventricular device, and subclinical seizures, necessitating multiple anti-epileptic drugs Conclusions A multifaceted approach including aggressive management of cerebral edema and ICP as well as treatment with immunomodulating agents and cessation of seizures may prevent brain herniation, secondary neurologic injury and death in patients with EEE. Effective management and treatment in our patient contributed to a dramatic recovery and ultimate good outcome. Keywords Eastern Equine Encephalitis Intracranial hypertension Cerebral edema Seizure Introduction Eastern Equine Encephalitis (EEE) virus is an arbovirus that causes human infection via a mosquito vector. While most infections with EEE virus are asymptomatic, symptomatic infections typically manifest as a generalized illness with fever. Neuroinvasive illness is uncommon with an incidence for all arboviruses in the United States of 0.20 per 100,000 persons [1]. In 2010, ten cases of EEE virus were reported by the Centers for Disease Control. All ten patients had encephalitis and required hospitalization. Five of these patients died [2]. We present a case report and successful management of a patient with EEE. Case Report L. C. Wendell (&) N. S. Potter B. B. Thompson Departments of Neurology and Neurosurgery, Rhode Island Hospital/Warren Alpert School of Medicine at Brown University, 593 Eddy Street, APC 712, Providence, RI 02903, USA e-mail: [email protected] J. L. Roth Department of Neurology, Rhode Island Hospital/Warren Alpert School of Medicine at Brown University, Providence, RI, USA S. P. Salloway Departments of Neurology, Butler Hospital/Warren Alpert School of Medicine at Brown University, Providence, RI, USA A 21-year-old man initially presented to the emergency department of an outside hospital with 24 h of headache, fever, and vomiting. He had a past medical history of beta thalassemia minor, recent extraction of his wisdom teeth on amoxicillin and recent exposure to mosquitos while golfing. Initial evaluation revealed a fever (103.8 °F), a normal neurologic exam, a leukocytosis (11.9 9 109 per L) and hyponatremia (133 mEq/L). Initial head CT was reported as normal although there was a question of a right temporal hypodensity. Lumbar puncture (LP) was performed in the emergency department and demonstrated 585 nucleated 123 Neurocrit Care cells/mm3 with a neutrophilic predominance (75 %), elevated protein (485 mg/dL) and negative Gram stain. Herpes simplex virus (HSV) polymerase chain reaction (PCR) was sent. He was started on ceftriaxone, vancomycin, metronizadole, and acyclovir for empiric coverage of bacterial meningitis and HSV encephalitis. He was admitted, and his hospital course was complicated by generalized convulsions, treated with phenytoin, and hypercarbic respiratory failure, requiring noninvasive positive pressure ventilation (NIPPV) and transfer to the ICU. The following day, he was transferred to our hospital’s NeuroICU for further management. On exam, he opened his eyes to voice, had decreased attention and concentration, was nonverbal, had normal cranial nerves and normal strength, and followed simple commands. MRI brain (Fig. 1) performed on hospital day (HD) #2 of his admission to our hospital revealed T2 and FLAIR hyperintensities involving the bilateral mesial temporal lobes, the left uncus and right insular cortex without associated restricted diffusion or enhancement; leptomeningeal engorgement was most prominent along the high bifrontal convexities; and basal cisterns were patent. HSV PCR from the outside hospital was negative. Repeat LP demonstrated an elevated opening pressure (46 cm H20), 70 nucleated cells/mm3 with a lymphocytic predominance (74 %), elevated protein (297 mg/dL), and negative Gram stain. HSV PCR was resent, and the results were again negative. Extensive serum and CSF work-up for other viral encephalitides was also pursued. Doxycycline was added to his antibiotic regimen for coverage of tickborne illnesses; however, work-up for these illnesses was negative. Fig. 1 Non-contrast axial FLAIR MRI brain at presentation demonstrating bilateral temporal hyperintensities 123 On HD #3, head CT revealed bilateral mesial temporal lobe hypodensities consistent with previous MRI findings as well as right greater than left effacement of the Sylvian fissures, small ventricles and diffuse sulcal effacement. He received 1 g/kg boluses of 20 % mannitol IV q6 h and 3 % hypertonic saline (HTS) continuous infusion for a target sodium of 155 mEq/L to treat empirically for intracranial hypertension (Fig. 2). Cerebrospinal fluid (CSF) culture remained negative from his initial LP. Vancomycin and metronidazole were discontinued given no evidence for Streptococcus pneumonia infection or abscess from recent dental work. He was continued on ceftriaxone, doxycycline, and acyclovir. His mental status continued to worsen, and he required intubation for airway protection on HD #4. On exam, he had no eye opening, equal and reactive pupils, conjugate roving eye movements, positive corneal, gag and cough reflexes, localization of his arms, and withdrawal of his legs. He was monitored on continuous electroencephalography (EEG) (Table 1), which demonstrated severe diffuse encephalopathy and subclinical seizures; levetiracetam was added for further seizure management. The patient was found to have a mildly positive serum mycoplasma IgM (1:64). Ceftriaxone was discontinued, and doxycycline was increased to cover possible CSF mycoplasma infection. On HD #5, his exam worsened to extensor posturing of his arms and triple flexion of his legs. An intracranial pressure (ICP) monitor (Codman, Codman & Shurtleff, Inc., Raynham, MA) was placed in the right frontal lobe. Initial ICP was 21 mm Hg. He required 30 cc boluses of 23.4 % HTS and continuous infusion of 3 % HTS to keep ICP <20 mm Hg. Repeat head CT on HD #6 demonstrated continued diffuse sulcal effacement and partial effacement of the basal cisterns. Serum EEE IgM was found to be positive (1:128). CSF EEE IgM was confirmed positive by the Massachusetts Department of Health. The remainder of the work-up for other viral encephalitides was negative. Doxycycline and acyclovir were discontinued. He was started on methylprednisolone 1 g IV qday and intravenous immunoglobulin (IVIg) 0.4 mg/kg qday on HD #8. The patient continued to have elevated ICP despite universal measures, sedation with propofol and fentanyl, maintenance of eucarbia and optimization of osmotherapy. On HD #9, he required a single dose of pentobarbital 100 mg IV for sustained ICP >40 mm Hg, and ICP improved from 57 to 12 mm Hg. An external ventricular device (EVD) (Codman, Codman & Shurtleff, Inc., Raynham, MA) was then placed and allowed to drain at 0 cm H20 above the level of the Foramen of Monroe with sustained improvement in ICP to <20 mm Hg (initial ICP 6 mm Hg). He had recurrent electrographic seizures on continuous EEG requiring addition of valproic acid. Due to development of a rash on his back and inadequate seizure Neurocrit Care Fig. 2 Hospital management of patient’s intracranial hypertension. ICP intracranial pressure, LP lumbar puncture, EVD external ventricular drain, HTS hypertonic saline, solid Line ICP in mm Hg, dotted line serum sodium in mEq/L, black triangle 20 % Mannitol 1 g/kg IV, black diamond 23 % HTS 30 cc IV, open diamond 23 % HTS 30 cc IV and pentobarbital 100 mg IV Table 1 Results of electroencephalogram (EEG) monitoring during hospital course and anti-epileptic drug (AED) regimen used Hospital Day 1 EEG Results AED Regimen Moderate-severe diffuse encephalopathy, occasional left hemisphere sharp waves Phenytoin 3–4 Severe diffuse encephalopathy, burst suppression Phenytoin 5–7 Frequent runs of left frontal or bifrontal 1–2 Hz rhythmic activity, consistent with ongoing electrographic seizure; severe diffuse encephalopathy with burst suppression Phenytoin, levetiracetam 8–9 Frequent runs of left frontal or bifrontal rhythmic 2–4 Hz activity lasting 10 s to 20 min (15–20 per hour), consistent with ongoing electrographic seizure; severe diffuse encephalopathy Phenytoin, levetiracetam, propofol 10 Runs of bifrontal and left temporal 2 Hz rhythmic activity (5–15 per hour) consistent with electrographic seizures; severe diffuse encephalopathy Phenytoin, levetiracetam, valproate, propofol 11–12 Runs of bifrontal, rhythmic 1–2 Hz activity (15 per hour), consistent with electrographic seizure which resolves with phenobarbital; severe diffuse encephalopathy Pheyntoin, levetiracetam, valproate, phenobarbital 12–13 Intermittent runs of bifrontal 1.5–2 Hz rhythmic activity (1–5 per hour); moderate-severe diffuse encephalopathy Phenytoin, levetiracetam, phenobarbital 13–14 Runs of bifrontal rhythmic 1 Hz activity (15 per hour); moderate diffuse encephalopathy Phenytoin, levetiracetam, phenobarbital 14–15 Runs of generalized or bifrontal rhythmic 1.5 Hz activity (2–10 per hour); moderate encephalopathy Phenytoin, levetiracetam, phenobarbital 18 Moderate diffuse encephalopathy Phenytoin, levetiracetam, phenobarbital Six-month follow-up Normal background rhythms (9–11 Hz) with left posterior temporal sharp waves Levetiracetam, weaning off phenobarbital control, valproic acid was discontinued and phenobarbital was added with good effect. After five doses of methylprednisolone and IVIg and better seizure control (HD #12), the patient’s exam had improved to opening eyes spontaneously, tracking and regarding the examiner but not following commands, localizing both arms (left greater than right), and withdrawing both legs. He was weaned off sedation and successfully extubated on HD #14 though he initially required NIPPV for hypercarbia. His exam had improved to being alert, saying occasional words, following commands and displaying purposeful and spontaneous movement of his arms and legs. EVD was weaned successfully and removed on HD #20. Repeat MRI brain on HD #21 (Fig. 3) demonstrated increased T2 hyperintensity in the bilateral medial thalami and left anterior putamen and patchy enhancement of the left hippocampus, mesial temporal lobe and amygdala. He continued to improve and became more conversant but with mild inattention and slowness in responding to questions. He was discharged on HD #30 to an acute rehabilitation facility. At one year, his Glasgow Outcome Scale-Extended (GOS-E) score was 6, indicating upper moderate disability. 123 Neurocrit Care independently and enroll in limited college coursework. Levetiracetam had been weaned off, and he remained seizure free. Discussion Fig. 3 Non-contrast axial FLAIR MRI brain on hospital day #21 demonstrating thalamic and basal ganglia FLAIR hyperintensities He was living at home with his parents, struggled with short-term memory difficulties and was being treated for anxiety. A routine EEG performed five months after presentation demonstrated a return of normal background rhythms, though with occasional epileptiform discharges in the left hemisphere. He had been seizure free for several months on levetiracetam monotherapy. MRI brain demonstrated improvement in previously seen hyperintensities but ventricular enlargement with basal ganglia and mesial temporal atrophy, including hippocampal volume loss that may correlate with his cognitive and behavioral symptoms (Fig. 4). At two years, his GOS-E was seven, indicating lower good recovery. His short-term memory continued to improve, and he could complete activities of daily living Fig. 4 Non-contrast axial FLAIR MRI brain one year post-discharge demonstrating resolution of previous FLAIR hyperintensities 123 We described a 21-year-old man with EEE who developed seizures, cerebral edema and intracranial hypertension, requiring aggressive management to prevent brain herniation and death. EEE is associated with a high rate of morbidity and mortality. One case series of 36 EEE patients reported that only one patient fully recovered and 36 % of patients died [3]. No specific antiviral treatment for EEE exists; thus, supportive care is the cornerstone of management [4]. With any encephalitis, the first steps in management begin with identifying the pathogen, which is commonly a virus. Neuroimaging, preferably with MRI, and CSF analysis are paramount in identifying a diagnosis [4]. The thalami and basal ganglia are most frequently involved in EEE as was seen in our patient. Cortical involvement can be in differing locations [3]. Depressed level of consciousness and coma are prominent in EEE [3], and patients must be monitored closely for ability to protect the airway, impending respiratory failure and necessity for intubation [5]. In patients with worsening consciousness, it is also imperative to suspect cerebral edema and intracranial hypertension. Encephalitic patients with coma or imaging findings concerning for intracranial hypertension should be considered for ICP monitoring [6]. Three-fourths of patients with viral encephalitis will require specific treatment for cerebral edema, and the Glasgow Coma Scale (GCS) is not predictive of initial ICP [7, 8]. The importance of monitoring Neurocrit Care for intracranial hypertension in these patients has been described in a small case series of ten patients with viral encephalitis, mostly herpes encephalitis. An ICP >20 mm Hg was associated with mortality, but transient elevations in ICP did not prohibit survival. Intracranial hypertension peaked on average at day 12 in patients with viral encephalitis [8]. Our patient had multiple episodes of intracranial hypertension that peaked eleven days into his hospital course. He had elevations of ICP >40 mm Hg which ultimately improved with aggressive medical treatment and placement of an EVD. Decompressive craniectomy can also be considered in patients with elevated ICP who fail aggressive medical therapy and has been reported as a lifesaving treatment in a patient with bacterial meningitis and refractory intracranial hypertension [9]. Given that our patient’s ICP improved after placement of an EVD, we elected not to pursue this approach. In addition to ventilatory support for airway protection and management of cerebral edema and elevated ICP, our patient required specific management for seizures. Since encephalitis leads to cortical inflammation, seizures can be a common feature [10]. Half of patients with EEE will have seizures, most frequently generalized convulsions [3]. Titration of multiple anti-epileptic medications and monitoring with continuous EEG were required to control seizures in our patient. Despite having several findings that would have predicted a poor prognosis, including initial CSF white count >500 cells/mm3 [3], initial ICP >12 mm Hg [8], and GCS score <7 [7], our patient had a good outcome secondary to effective management and treatment of cerebral edema, intracranial hypertension, and seizures. In addition to control of seizures and ICP, high-dose methylprednisolone and IVIg may have contributed to improved outcome. Complete recovery was reported in a comatose man with EEE who received steroids and IVIg [11]. A more recent case of severe cytomegalovirus encephalitis also demonstrated improved outcome after use of steroids and IVIg [12]. While EEE can cause direct neuronal injury, it also produces inflammatory damage, leading to necrosis and demyelination of neurons. Immunosuppression might seem counterintuitive in the setting of infection, but IVIg and methylprednisolone may contribute to halting cytotoxic edema secondary to the inflammatory cascade triggered by EEE infection and help to improve outcome [11]. A multi-faceted approach including aggressive management of cerebral edema and elevated ICP as well as treatment with immunomodulating agents and cessation of seizures may prevent secondary neurologic injury and death in patients with EEE. Effective management and treatment in our patient contributed to a dramatic recovery and ultimate good outcome. Disclosure None. References 1. Centers for Disease Control and Prevention (CDC). West nile virus disease and other arboviral diseases—United States, 2011. MMWR Morb Mortal Wkly Rep. 2012;61:510–4. 2. Centers for Disease Control and Prevention (CDC). West Nile virus disease and other arboviral diseases–United States, 2010. MMWR Morb Mortal Wkly Rep. 2011;60(30):1009–13. 3. Deresiewicz RL, Thaler SJ, Hsu L, Zamani AA. Clinical and neuroradiographic manifestations of eastern equine encephalitis. N Engl J Med. 1997;336(26):1867–74. 4. Tunkel AR, Glaser CA, Bloch KC, et al. The Management of Encephalitis: clinical Practice Guidelines by the Infectious Diseases Society of America. Clin Infect Dis. 2008;47(3):303–27. 5. Gaieski DF, Nathan BR, Weingart SD, Smith WS. Emergency neurologic life support: meningitis and encephalitis. Neurocrit Care. 2012;17(Suppl 1):S66–72. 6. Ropper AH, Gress DR, Diringer MN, Green DM, Mayer SA, Bleck TP. Neurological and neurosurgical intensive care. 4th ed. Philadelphia: Lippincott Williams and Wilkins; 2004. 7. Whitley RJ, Alford CA, Hirsch MS, et al. Vidarabine versus acyclovir therapy in herpes simplex encephalitis. N Engl J Med. 1986;314(3):144–9. 8. Barnett GH, Ropper AH, Romeo J. Intracranial pressure and outcome in adult encephalitis. J Neurosurg. 1988;68(4):585–8. 9. Baussart B, Cheisson G, Compain M, et al. Multimodal cerebral monitoring and decompressive surgery for the treatment of severe bacterial meningitis with increased intracranial pressure. Acta Anaesthesiol Scand. 2006;50(6):762–5. 10. Ziai W, Lewin J III. Update in the diagnosis and management of central nervous system infections. Neurol Clin. 2008;26(2):427–68. 11. Golomb MR, Durand ML, Schaefer PW, McDonald CT, Maia M, Schwamm LH. A case of immunotherapy-responsive eastern equine encephalitis with diffusion-weighted imaging. Neurology. 2001;56(3):420–1. 12. Xu X, Bergman P, Willows T, et al. CMV-associated encephalitis and antineuronal autoantibodies—a case report. BMC Neurol. 2012;12(1):87. 123