Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Jatene procedure wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
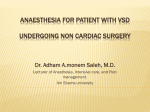
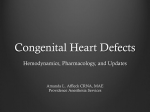
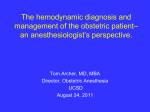
THERAPY AND PREVENTION CONGENITAL HEART DISEASE Significance of systemic vascular resistance in determining the hemodynamic effects of hydralazine on large ventricular septal defects MAKOTO NAKAZAWA, M.D., ATSUYOSHI TAKAO, M.D., YONG CHON, M.D., TAKASHI SHIMIZU, M.D., MAYUMI KANAYA, M.D., AND KAzuo MOMMA, M.D. Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017 ABSTRACT The hemodynamic effects of hydralazine were studied in 17 infants and young children with ventricular septal defects to clarify the significance of systemic vascular resistance (SVR) in determining these effects. Patients with peak pulmonary arterial pressures greater than 75% of systemic pressure were placed in group 1, which was further divided into group Ia (n = 6), consisting of those with a control SVR of 20 U m2 or higher, and group lb (n = 8), consisting of those with a lower SVR. Group II consisted of three patients with lower pulmonary arterial pressures. Intravenous injection of hydralazine (0.3 mg/kg) reduced SVR in all but two patients. The magnitude of reduction correlated with prehydralazine (control) SVR (r = .66, p < .01). Systemic blood flow (Qs) increased from 3.7 0.7 to 5.0 + 0.8 1/min/m2 (p < .005). The mean systemic arterial pressure for all patients decreased from 69 + 2 to 65 2 mm Hg (p < .01) and the mean pulmonary arterial pressure decreased from the control value by 9 4% (p < .01) in group I and by 17 + 1% in group II. Pulmonary blood flow (Qp) did not change significantly in either group. The Qp/Qs ratio was reduced from 3.6 0.4 to 2.4 0.2 (p < .02) in group Ia. In sharp contrast, however, it increased from 2.6 + 0.3 to 3.3 0.5 (p = .06) in group lb. The posthydralazine Qp/Qs ratio, expressed as percent of the control value, inversely correlated with the control SVR (r = - .61, p = .02) in group I. The response was not different in the group II patients. Thus, we conclude that control SVR is important for prediction of the hemodynamic effects of afterload reduction by hydralazine in infants and young children with large ventricular septal defects, and that this drug may be beneficial in patients with high control SVRs since a high SVR brings about a decrease in the Qp/Qs ratio. Circulation 68, No. 2, 420-424, 1983. THE HEMODYNAMIC EFFECTS of vasodilating drugs on ventricular septal defects (VSDs) have been reported by several investigators," although the results are not conclusive. In previous studies a wide variety of drugs with different sites of action were used, which resulted in inconsistent results. In addition, there was a great variation in hemodynamic characteristics of study subjects at control, i.e., in the size of their VSDs, in their systemic or pulmonary vascular resistances (SVRs or PVRs), and in the responsiveness of the vessels on which the drugs acted in the subjects. The amount of shunt flow through a VSD is determined by the ratio of PVR to SVR in a large and nonrestrictive VSD, or by the interrelationship between the size of the VSD and SVR in a restrictive VSD.7 In either condition, the amount of shunt flow is From the Department of Pediatric Cardiology, The Heart Institute of Japan, Tokyo Women's Medical College, Tokyo. Address for correspondence: Makoto Nakazawa, M.D., Department of Pediatric Cardiology, The Heart Institute of Japan, Tokyo Women's Medical College, 10 Kawada-cho, Shinjuku-ku, Tokyo 162, Japan. Received Dec. 2, 1982; revision accepted April 25, 1983. 420 greatly affected by SVR.8 Since SVR is a major factor determining afterload to the left ventricle, it can be hypothesized that the effect of afterload reduction on the amount of interventricular shunting is dependent on the control SVR and on responsiveness of the systemic vascular beds. To test this hypothesis, we studied 17 infants and young children with VSDs and obtained hemodynamic data before and after the intravenous administration of hydralazine, an afterload-reducing drug. Subjects and methods The subjects of this study were 14 patients with isolated VSDs, two patients with VSDs and a patent ductus arteriosus, and one patient with a VSD type of double-outlet right ventricle. Patients' ages ranged from 2 to 36 months (mean, 12 +- 10 [SD] months) and 11 were less than 1 year old. The major clinical findings and treatments for each patient are summarized in table 1. Informed consent was obtained for each patient before the study began. Right and left heart catheterization was done in each patient before and 10 min after an intravenous injection of hydralazine at a dose of 0.3 mg/kg and while oxygen consumption was being measured by the flow-through method. Systemic CIRCULATION THERAPY AND PREVENTION-CONGENITAL HEART DISEASE TABLE 1 Clinical findings and treatments Patient No. Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017 Group la 1 2 3 4 5 6 Group lb 7 8 9 10 11 12 13 14 Group II 15 16 17 Age (months) Weight (kg) RR 7 11 20 4 13 6 6.0 8.0 9.5 5.5 7.6 7.1 5 6 7 11 5 2 26 26 6 32 15 Paco2 Liver (cm) CTR (%) Digoxin (mg) 50 48 36 45 50 46 48 47 37 50 40 42 4 2 1 3 2 3 61 59 59 61 65 63 0.06 0.08 0.06 0.10 0.08 4.0 5.4 5.6 7.7 6.0 4.2 9.0 11.0 58 53 50 55 54 56 40 40 43 43 36 40 32 47 44 40 2 3 3 2 2 2 3 1 61 62 58 65 55 60 61 58 0.04 0.06 0.05 0.08 5.8 14.0 48 30 40 36 35 33 4 1 2 58 57 54 8.1 SpironoFurosemide lactone (mg) (mg) 10 12 5 4 - 4 - - 15 15 0.04 - 10 10 12 5 - 0.05 15 0.08 - 15 RR = respiratory rate (times/min); CTR = cardiothoracic ratio. and pulmonary blood flows (Qs and Qp) were obtained by the Fick method and then SVR and PVR were calculated and expressed in units per square meter (mm Hg/l/minim2). The patients were assigned to one of three groups according to their hemodynamic characteristics at control. The patients who had a peak pulmonary arterial pressure (PAP) of more than 75% of the peak systemic arterial pressure (SAP) were assigned to group I, which was further divided into a group of patients with SVRs of 20 U_m2 or higher (group Ia, n = 6) and a group of those with lower SVRs (group Ib, n = 8). The patients with lower peak PAPs were placed in group II (n = 3). The data were analyzed by the Student t test. All values were expressed as mean + SEM. Results The effects of an elevation in SVR on hemodynamics in patients with large VSDs. There was no statistical difference between group la and group lb for each of following parameters: mean SAP, mean PAP, mean right atrial pressure (RAP), Qp, PVR, and peak PAP/peak SAP ratio. However, in group Ia mean left atrial pressure (LAP) was higher (p < .01), Qs was less (p < .005), and the Qp/Qs ratio was larger (p < .05) than in group lb (table 2). The effect of hydralazine on cardiovascular pressure. Mean SAP for the total patient group decreased from 69 + 2 to 65 + 2 mm Hg (by 7 + 2%; p < .01) after hydralazine. The largest reduction observed among the patients was from 77 to 57 mm Hg (26% reduction). LAP was reduced in 12 patients and remained unchanged in five, the mean reduction being from 12 ± 1 Vol. 68, No. 2, August 1983 to 10 + 1 mm Hg (- 2 + 1 mm Hg; p < .02) after hydralazine. For these changes there was no difference between the groups. Mean PAP in group I, which was 56 + 3 mm Hg before hydralazine, was reduced to 50 + 3 mm Hg (p < .01). PAP was also reduced in group II (by 17 ± 1% from control). The mean RAP decreased in 13 patients and increased in two others and it was unchanged in the remaining two patients. The total group mean reduction was from 6 + 1 before to 5 ± 1 mm Hg after hydralazine, but this reduction was not statistically significant. The effects of hydralazine on SVR and PVR. Mean SVR in all patients was significantly (p < .005) reduced (from 19.0 + 1.6 to 15.1 ± 0.9 U m2) by hydralazine. Posthydralazine SVR, expressed as percent of the control value, inversely correlated with prehydralazine SVR (r = - .66, p < .01; figure 1). In group Ia, in which the control SVR was high by definition, the reduction in SVR was greater (29 ± 6%) than in group Ib (6 + 5%; figure 2). The change in PVR in group Ia was not significant and was only barely significant in group lb (4.8 ± 0.7 to 3.6 ± 0.6 U-m2; p < .05). The magnitude of changes in PVR did not correlate with prehydralazine PVR. The effects of hydralazine on Qs, Qp, and the Qp/Qs ratio. Qs increased after hydralazine in all but one 421 NAKAZAWA et al. TABLE 2 Hemodynamic effects of hydralazine in infants and children with VSDs Patient SAP Age No. (months) C Group la 1 7 11 2 3 20 4 5 6 Mean ± SD 4 13 6 (SEM) Group lb 7 5 8 6 Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017 9 10 11 12 13 14 Mean 7 11 5 2 26 26 ±SD (SEM) Group II 15 6 16 17 36 15 PAP LAP RAP H C H C H 72 70 83 64 75 67 72 7 (3) 74 70 85 56 68 56 68 11 (5) 41 67 57 47 65 35 52 13 (5) 52 55 39 47 57 31 47 10 (4) 13.5 18.5 17 9.5 12 13.5 13.5 16 17 8 12 7 12 4 4 15 4 4 7 5 7 4 (2) 61 77 70 68 53 60 67 75 66 8 (3) 53 57 65 68 60 60 63 60 61 5 (2) 72 77 61 60 38 50 56 60 59 12 (4) 62 67 59 53 40 35 53 51 53B 11 (4) 11.5 11.5 11.5 9 10.5 9.5 9 8 8 7 9 8.5 10 9 10 9.5 98 10 1.2 1.3 (0.4) (0.4) 63 80 75 57 73 72 25 31 18 21 26 15 15 15 8 14A 3 (1) 7 15 4.5 PVR H C H C 2.3 4.0 3.1 6.2 5.4 2.4 3.9 1.6 (0.7) 4.3 5.8 2.0 5.9 4.6 21.8 22.0 30.5 23.6 34.1 23.1 (2) 7 10.5 7 3 5.5 3.5 6 3 (1) 6 9 9.5 6 3 2 5 5 6 3 5 8 6.5 5 2.5 2 5 3 5 B 2 6.8 7.6 4.2 5.3 2.8 2.9 2.8 5.6 4.8 1.9 (1) (0.7) (0.7) (0.6) 11 7.5 3.5 3.5 6 3 C 2.7 1.5 2.6 Qp SVR 2.4 4.2 1.7 (0.7) 6.8 5.6 3.5 2.4 2.9 1.0 3.0 3.2 3.6B 1.8 2.3 0.9 1.9 H C H 20.0 18.0 16.1 16.8 24.3 12.4 25.9A 17.9B 5.2 4.0 (2.1) (1.6) 11.9 10.5 12.8 6.1 9.8 9.0 10.0 2.4 (1.0) 8.9 3.3 6.9 3.0 11.2 2.7 6.6 2.5 9.8 2.2 10.2 2.9 8.9 2.8A 1.8 0.4 (0.8) (0.2) 14.5 13.9 9.4 15.9 15.1 18.8 12.0 17.5 14.6 3.0 8.9 8.6 11.8 9.7 10.8 13.8 16.7 9.1 11.2 2.8 (1.0) 7.4 10.2 14.2 18.8 11.5 27.7 14.7 13.0 14.7 6.2 12.6 11.6 10.5 15.0 17.1 14.1 10.9 16.3 13.5 2.5 (I1.1) (0.9) 20.0 15.4 23.4 12.0 11.0 18.0 C = control data;H = 10 min after hydralazine. kp < .05 for difference between group Ia and group Ib; 8p < .05 for difference between C and H; cp patient (No. 9) who already had a Qs of 6.4 I/min/m2 and a SVR of 9.4 U.m2. After hydralazine in this patient Qs was 5.6 1/min/m2 and SVR was 10 U.m2. The total group mean Qs increased from 3.7 + 0.7 to 5.0 ± 0.8 I/min/m2 (p < .005). Qp decreased in three of the six patients in group la and in two of the eight patients in group Jb, while it increased in two in group Ia and in six in group lb. The mean changes were not statistically significant in either group (figure 3). The Qp/Qs ratio decreased in group Ia from 3.6 + 0.4 to 2.4 ± 0.2 (p < .02). In sharp contrast, the ratio increased in group lb from 2.6 + 0.3 to 3.3 ± 0.5 (p = .06); figure 4). There was a significant difference between the changes in these two groups (p < .005). The QpIQs ratio did not change substantially in two group II patients; one of these had a small VSD and the other had a high Qp/Qs ratio and an SVR of 15.4 U.m2. In another group II patient with a control SVR of 20 U m2, however, the Qp/Qs ratio decreased from 2.0 to 1.3. To evaluate the effect of control SVR on the change in Qp/Qs ratio in patients with large VSDs, the posthy422 C H C H 3.7 3.3 5.3 3.2 2.8 4.5 3.8B 0.9 (0.4) 3.4 3.5 4.7 2.4 4.5 3.1 3.6A 0.9 (0.4) 2.4 2.1 2.1 2.1 3.5 2.3 2.4B 0.5 (0.2) 4.3 5.1 5.6 4.2 3.5 4.3 5.8 4.3 4.6 1.1 0.8 (2.2) (0.4) (0.3) 2.1 1.8 1.8 2.5 3.1 4.2 2.8 2.3 2.6 0.8 (0.3) 1.7 2.0 2.5 4.5 3.3 6.0 3.0 3.0 3.3c 1.4 (0.5) 2.0 2.0 1.2 1.3 1.9 1.3 5.6 5.4 10.5 12.4 3.8 5.1 = Qp/Qs Qs 4.2 4.9 6.4 3.9 3.5 3.2 5.6 4.0 4.5 2.8 5.2 3.2 4.3 6.6 4.0 .06. dralazine Qp/Qs ratio, expressed as percent of the control value, was compared with the prehydralazine SVR in group I patients and a rough but significant correlation was found (r = -.61, p = .02; figure 5). Group II patients were excluded from this analysis because their VSDs were smaller, although their SVR responses were not different from those of group I patients (figure 5). The control PVR, however, did not correlate with the change in the Qp/Qs ratio. Discussion In infants with large VSDs, left ventricular performance is depressed by volume overload in association with a relative lack of left ventricular muscle mass.9 This is hemodynamically manifested by an elevation in left ventricular filling pressure and a decrease in Qs. The latter stimulates the renin-angiotensin system, catecholamine release, and the sympathetic nervous system, '° resulting in an increase in SVR. The high resistance impedes left ventricular ejection in a failed heart, which causes a further decrease in the forward flow and an increase in the left-to-right shunt, so that a CIRCULATION THERAPY AND PREVENTION-CONGENITAL- HEART DISEASE SVR(0/o) after H L/min/m' 30 T 0 110 1 * Y= -1.8 X + 116 r= -0.66 n= 17 *. 90g I a -ns ns 20 -+ II I -b . 0 70 . I . 10 S 0 50 132±16 % 92*8 % I 10 0 ---I I 40 prehydralazine SVR; units-m2 20 Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017 FIGURE 1. SVR after hydralazine, expressed as percent of the control value (SVR [%] after H), correlated significantly (p < .01) with control SVR. vicious cycle is formed. It is therefore expected that if the amount of shunting is reduced by any intervention, the vicious cycle can be interrupted and clinical improvement can be obtained. The conditions of patients with VSDs are similar to those of patients with mitral regurgitation when the left ventricle is regarded from a purely hemodynamic point of view. It has been established that afterload reduction in mitral regurgitation is beneficial because it reduces the amount of regurgitation, lowers LAP, and increases the forward flow.1'I' This suggests that afterload reduction in patients with VSDs may be effective in reducing the amount of shunting. However, reaction of the pulmonary vascular bed to vasodilators can not be ignored in patients with large VSDs because the I -b I .a units-ml 0o 30 C C H H c FIGURE 3. Changes in Qp. There were no statistically significant changes in either group Ia or group lb patients or when comparing the two groups. amount of shunting is determined by the ratio of PVR to SVR. It is known that in patients with other cardiac diseases vasodilators dilate the pulmonary vascular bed as well as the systemic one,"' 'v"7 although Fripp et al.'8 have reported that hydralazine failed to reduce the PVR in two patients with pulmonary vascular obstructive disease secondary to congenital heart disease. In this study and in another by Goldberg et al.'9 the magnitude of reduction in vascular resistance by vasodilators was shown to be a function of the pretreatment resistance value. This implies that either a nonconstricted vessel is not dilated to any great extent by the drugs or that an already dilated vessel no longer responds, as was the case in patient 9. In patients in whom PVR alone is elevated functionally, vasodilators will act more on the pulmonary than on the sysQp/Qs 11 H l.a 6- I-b 11 40T 30\T 30 _ p± /= p c 0.02 0.01 ns + 4- :0.06 20 --_> 71 + 71*6% 144 2 - - 10 94t5% 125±11% 71t6 % p < 0.02 0- p < 0.005 C H C H C H O FIGURE 2. Changes in SVR. SVR was significantly (p < .005) reduced in all patients, but the reduction was larger in group Ia than in group lb. NS = not significant at p > .05; C = control data; H = data obtained 10 min after hydralazine. Vol. 68, No. 2, August 1983 ~ C H C H C H FIGURE 4. Changes in the Qp/Qs ratio. The ratio decreased in group Ia and increased in group lb patients. The changes were statistically different in the two groups. 423 NAKAZAWA et al. QP/Qs after H ( % of the control ) 200 ,Y = 165 - 3.3 X 0 r = - 0.61 150 + n= 14 . 100 *'- * 0@ + Group I; 0 Group 11; 0 0 0 . *s 0. 50 0 References 0 0 10 20 30 40 units-m2 Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017 FIGURE 5. The Qp/Qs ratio after hydralazine, expressed as percent of the control value, correlated significantly (p = .02) with control SVR in patients with large VSDs (group I). The data from group II patients are plotted in this figure, showing that the Qp/Qs response was not different from that in group I. temic vascular bed, so that Qp will increase more than Qs or shunt flow; this was the case in patients in group lb of this study. The response, however, will be the opposite in patients with elevated SVRs. This was shown to be true in group Ia patients. Since in infants with large VSDs PVR is mildly to moderately elevated by the medial thickening,7 elevation of SVR is a prerequisite for obtaining reduction in the Qp/Qs ratio with vasodilators. The change in PVR varied in this study. Since there was no correlation between the pretreatment value for PVR and the magnitude of the change, the apparent PVR response does not seem to be an active one, but seems to be affected passively by Qp which, in turn, is determined by the amount of shunting. It is likely that, in patients in whom the response of SVR was greater than that of pulmonary circulation, Qp decreased and the apparent value for PVR was elevated or unchanged. On the other hand, when PVR was lowered more than SVR by hydralazine, the decrease in PVR became apparent. In a patient with a moderate-sized VSD, the amount of shunting is determined by the size of the VSD and augmented by elevation of SVR, as illustrated by the case of patient 15. This response was also seen in the experimental studies of Synhorst et al.3 and Boucek et al.4 The model used in their studies was a restrictive and moderate-sized VSD and the muscular tone of systemic resistant vessels would be expected to be high due to experimental stress. Vasodilators would therefore dilate the constricted systemic vascular bed to increase Qs and decrease the shunt flow. 424 As shown in our study, reduction of the Qp/Qs ratio is not necessarily associated with a decrease in Qp because an increment in venous return secondary to an increase in Qs offsets the decrease in left-to-right shunting.2 In summary, the effect of hydralazine on the Qp/Qs ratio in infants and young children with large VSDs was largely dependent on pretreatment SVR, which was shown by the fact that the Qp/Qs ratio was reduced only in those with a high control SVR. 1. Beekman RH, Rocchini AP, Rosenthal A: Hemodynamic effects of nitroprusside in infants with a large ventricular septal defect. Circulation 64: 553, 1981 2. Beekman RH, Rocchini AP, Rosenthal A: Hemodynamic effects of hydralazine in infants with a large ventricular septal defect. Circulation 65: 523, 1982 3. Synhorst DP, Lauer RM, Doty DB, Brody MJ: Hemodynamic effects of vasodilator agents in dogs with experimental ventricular septal defect. Circulation 54: 472, 1976 4. Boucek MM, Chang R, Synhorst DP: Effects of prazosin and hydralazine on the hemodynamics of chronically instrumented lambs with ventricular septal defect. Circulation 62 (suppl III): III1 15, 1980 (abstr) 5. Linday LA, Levin AR, Klein AA, Reidenberg MM, Engle MA: Effect of vasodilators on left-to-right shunt in infants and children. Pediatr Res 14: 447, 1980 (abstr) 6. Macri R, Redaelli S: Vasodilator in VSD's. Circulation 56: 329, 1980 (letter) 7. Rudolph AM: Congenital disease of the heart. Chicago, 1974, Year Book Publishers 8. Tanenbaum HL, Pfaff WW: Effect of pressor amines on experimental intracardiac shunts and valvular regurgitation. Dis Chest 44: 485, 1963 9. Jarmakani MM, Graham TP Jr, Canent RV Jr, Spach MS, Capp MP: Effect of site of shunt on the left heart volume characteristics in children with ventricular septal defect and patent ductus arteriosus. Circulation 40: 411, 1969 10. Talner NS: Heart failure. In Moss AJ, Adams FH, Emmanouilides GC, editors: Heart disease in infants, children and adolescents, ed 2. Baltimore, 1977, Williams & Wilkins Co., p 660 11. Franciosa JA: Effectiveness of long-term vasodilator administration in the treatment of chronic left ventricular failure. Prog Cardiovasc Dis 24: 319, 1982 12. Greenberg BH, Massie BM, Brundage BH, Botvinick EH, Parmley WW, Chatterjee K: Beneficial effects of hydralazine in severe mitral regurgitation. Circulation 58: 273, 1978 13. Harshow CW, Grossman W, Munro AB, McLaurin LP: Reduced systemic resistance as therapy for severe mitral regurgitation of valvular origin. Ann Intem Med 83: 312, 1975 14. Lupi-Herrera E, Sandoval J, Seoane M, Bialostozky D: The role of hydralazine therapy for pulmonary arterial hypertension of unknown cause. Circulation 65: 645, 1982 15. Rubin LJ, Peter RH: Oral hydralazine therapy for primary pulmonary hypertenson. N Engl J Med 302: 69, 1980 16. Chatterjee K, Parmley WW: The role of vasodilator therapy in heart failure. Prog Cardiovasc Dis 19: 301, 1977 17. Mason DT: Symposium on vasodilator and inotropic therapy of heart failure. Am J Med 65: 101, 1978 18. Fripp RR, Gewitz MH, Werner JC, Whitman V, Rashkind WJ: Oral hydralazine in patients with pulmonary vascular disease secondary to congenital heart disease. Am J Cardiol 48: 380, 1981 19. Goldberg S, Mann T, Grossmanr W: Nitrate therapy of heart failure in valvular heart disease. Am J Med 65: 161, 1978 CIRCULATION Significance of systemic vascular resistance in determining the hemodynamic effects of hydralazine on large ventricular septal defects. M Nakazawa, A Takao, Y Chon, T Shimizu, M Kanaya and K Momma Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017 Circulation. 1983;68:420-424 doi: 10.1161/01.CIR.68.2.420 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1983 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/68/2/420 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/