Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
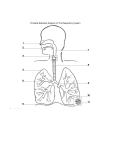
Respiratory System Dr. Michael P. Gillespie Functions Gas exchange. Regulation of blood ph. Contains receptors for the sense of smell. Filters inspired air. Produces sounds. Rids the body of some water and heat in expired air. Gas Exchange Cells use oxygen (O2) for metabolic reactions that release energy from nutrient molecules and produce ATP. These reactions release carbon dioxide (CO2). The cardiovascular system and the respiratory system cooperate to supple O2 and eliminate CO2. Components Nose. Pharynx (throat). Larynx (voice box). Trachea (windpipe). Bronchi. Lungs. Upper Respiratory System Nose. Pharynx. Associated structures. Lower Respiratory System Larynx. Trachea. Bronchi. Lungs. Functional Divisions Conducting portion. Interconnecting cavities and tubes both outside and within the lungs that filter, warm, moisten air and conduct it into the lungs. Nose, pharynx, larynx, trachea, bronchi, bronchioles, and terminal bronchioles. Respiratory portion. Tissues within the lungs where gas exchange occurs. Respiratory bronchioles, alveolar ducts, alveolar sacs, and alveoli. Otorhinolaryngology Diagnosis and treatment of the ears, nose and throat. Pulmonologist Diagnosis and treatment of disease of the lungs. Nose External and internal portions. External Nose Supporting framework of bone and hyaline cartilage covered with muscle and skin and lined with a mucous membrane. Frontal bone, nasal bones, and maxillae form the bony framework. External Nose The cartilaginous framework consists of the septal cartilage, lateral nasal cartilages, and alar cartilages. External Nose The two openings are the external nares or nostrils. Functions: Warming, moistening, and filtering incoming air. Detecting olfactory stimuli. Modifying speech vibrations as they pass through large, hollow, resonating chambers. Resonance refers to prolonging, amplifying, or modifying a sound by vibration. Internal Nose A large cavity in the anterior aspect of the skull. Lies inferior to the nasal bone and superior to the mouth. The internal nares or choanae provide communication between the external nose and the pharynx. Ducts from the paranasal sinuses and the nasolacrimal ducts also open into the internal nose. Internal Nose Lateral walls: ethmoid, maxillae, lacrimal, palatine, and inferior nasal conchae bones. Floor: the hard palate which consists of the palatine bones and the palatine process of the maxillae. Internal Nose Nasal cavity – the space within the internal nose. The anterior portion just inside the nostrils is called the vestibule. The nasal septum divides the cavity into right and left sides. Primarily hyaline cartilage, but also the vomer, and perpendicular plate. Air Filtration The vestibule is lined by skin containing coarse hairs, which filter out large dust particles. Three shelves are formed by the superior, middle, and inferior conchae. The conchae divide the nasal septum into groove like passageways called the superior, middle, and inferior meatuses. A mucous membrane lines the cavity and its shelves. Air Filtration The arrangement of the conchae and meatuses increases surface area in the internal nose. It traps water droplets during exhalation to prevent dehydration. The olfactory receptors line the superior nasal conchae and adjacent septum (olfactory epithelium). Air Filtration Inspired air is warmed by blood in the capillaries. Mucous secreted by goblet cells moistens the air and traps dust particles. Cilia move the mucous and trapped particles towards the pharynx to be swallowed or spit out. Rhinoplasty “Nose job”. The structure of the external nose is altered. Often performed for cosmetic reasons. Sometimes performed to repair a fractured nose or a deviated septum. Pharynx The pharynx or throat is a funnel shaped tube about 13 cm long. It starts at the internal nares and extends to the cricoid cartilage (the most inferior cartilage of the larynx). Pharynx Its wall is composed of skeletal muscles and it is lined with a mucous membrane. Pharynx Functions: Passageway for air and food. Resonating chamber for speech sounds. Houses the tonsils (participate in immune responses). Anatomical regions: Nasopharynx. Oropharynx. Laryngopharynx. Nasopharynx The nasopharynx is the superior portion of the pharynx. Extends from the posterior nasal cavity to the soft palate. 5 openings in its wall: 2 internal nares. Eustachian tubes (a.K.A. Auditory or pharyngotympanic). Opening into the oropharynx. Nasopharynx Pharyngeal tonsils. The nasopharynx is lined with pseudostratified ciliated columnar epithelium, which moves mucous down towards the inferior part of the pharynx. The eustachian tubes help to equalize air pressure between the pharynx and middle ear. Oropharynx The intermediate portion of the pharynx. Extends from the soft palate to the hyoid bone. One opening – the fauces (throat), the opening from the mouth. Common passageway for air, food, and drink. Lined with nonkeratinized stratified squamous epithelium to withstand abrasion from food particles. Palatine and lingual tonsils are found here. Laryngopharynx Inferior portion of the pharynx. Otherwise known as the hypopharynx. Opens to the esophagus posteriorly and the larynx anteriorly. Both a respiratory and a digestive pathway. Lined with nonkeratinzed stratified squamous epithelium. Larynx Voice box. A short passageway that connects the laryngopharynx with the trachea. Lies in the midline of the neck anterior to the 4th through 6th cervical vertebrae. Larynx Composed of 9 pieces of cartilage. Thyroid cartilage (Adam’s apple). Larynx Epiglottis – a large leaf shaped piece of elastic cartilage. During swallowing, the epiglottis closes off the glottis (vocal cords) and prevents food from entering the larynx and airways inferior to it. It shunts food to the esophagus. Larynx Cricoid cartilage. A ring of cartilage that forms the inferior wall of the larynx. This cartilage serves as the landmark for making an emergency airway (tracheostomy). Voice Production The mucous membrane of the larynx forms two pairs of folds. Ventricular folds (false vocal cords) – superior. Vocal folds (true vocal cords) – inferior. If air is directed against the vocal folds they vibrate and produce sounds (phonation). Voice Production The greater the pressure of the air, the louder the sound. Pitch is controlled by tension on the vocal folds. If they are pulled taught, the pitch raises. Decreasing muscular tension results in lower sounds. Vocal folds are usually thicker and longer in males than in females resulting in a lower pitch. Laryngitis & Cancer Of The Larynx Laryngitis is an inflammation of the larynx. It is often caused by a respiratory infection or irritants such as cigarettes or smoke. Laryngitis & Cancer Of The Larynx Chronic inflammation in long term smokers can cause a permanent hoarseness. Cancer of the larynx is found almost exclusively in smokers. Treatment consists of radiation therapy and / or surgery. Trachea The trachea (windpipe) is a tubular passageway for air that is about 12 cm long and 2.5 cm in diameter. Trachea It is anterior to the esophagus and extends from the larynx to the superior border of the 5th thoracic vertebra where it branches to form bronchi. Trachea Layers: Mucosa. Pseudostratified ciliated columnar epithelium and goblet cells. Submucosa. Hyaline cartilage. 16 – 20 incomplete, horizontal rings that resemble the letter C. The open part of each ring faces the esophagus and allows slight expansion of the esophagus into the trachea during swallowing. The solid C shaped ring prevents collapse of the trachea. Adventitia. Areolar connective tissue that joins the trachea to the surrounding tissues. Tracheostomy & Intubation Several conditions can block airflow: A crushing injury to the chest. Inflammation of the mucous membrane causing swelling. Vomit or another foreign object may be aspirated into it. If the obstruction is superior to the larynx, a tracheostomy may be performed. Tracheostomy & Intubation A tracheostomy is an operation to make an opening into the trachea. Intubation involves inserting a tube into the mouth or nose and passing it inferiorly through the larynx or trachea. The tube pushes any flexible obstruction out of the way. Mucous can be suctioned through the tube and the lumen provides a passageway for air. Bronchi The trachea divides into a right primary bronchus and a left primary bronchus at the superior border of T5. Carina – the ridge where the trachea branches into the right and left bronchi. The mucous membrane is the most sensitive here and triggers the cough reflex. Upon entering the lungs, the primary bronchi divide into secondary (lobar) bronchi – one for each lobe of the lung. 3 on the right and 2 on the left. Bronchi They then branch to tertiary (segmental) bronchi and eventually bronchioles. Terminal bronchioles are the smallest branch. This branching is referred to as the bronchial tree. Bronchial Control The amount of cartilage decreases as we move down the bronchial tree and the amount of smooth muscle increases. With no supporting cartilage, muscle spasms can close of the airways as in an asthma attack. Bronchial Control Sympathetic nerve stimulation causes relaxation of the smooth muscles of the bronchioles through release of epinephrine and norepinephrine. The parasympathetic division of the ANS and mediators of allergic reactions such as histamine cause contraction of bronchiolar smooth muscle. Lungs Trauma to the chest which causes one lung to collapse may not affect the other as they are in two distinct chambers. There are two layers of the pleural membrane: Visceral pleura and parietal pleura. The pleural cavity is the space between these membranes and is filled with serous fluid. Lungs Pleurisy or pleuritis is an inflammation of the pleural membrane. Pleural effusion is an accumulation of fluid in the pleural space due to persistence of inflammation. Surface Anatomy Of The Lungs Base. Apex. Costal surface. Mediastinal (medial) surface. Hilus. Root. Cardiac notch. Lobes, Fissures, & Lobules The lungs are divided into lobes by fissures. Each lung has an oblique fissure. The right lung also has a horizontal fissure. The left lung has a superior and an inferior lobe. The right lung has these as well as a middle lobe. Each lobe receives its own secondary (lobar) bronchus. Lobes, Fissures, & Lobules Superior, middle, and inferior bronchi on the right and superior and inferior bronchi on the left. The tertiary (segmental) bronchi arise from the lobar bronchi and supply a bronchopulmonary segment. Lobes, Fissures, & Lobules Terminal bronchioles are called respiratory bronchioles. Respiratory bronchioles are subdivided into alveolar ducts. There are about 25 orders or branching from the trachea to the alveolar ducts. Alveoli The alveoli and alveolar sacs surround the opening of the alveolar ducts. An alveolus is a cup-shaped outpouching lined by simple squamous epithelium. Alveoli An alveolar sac consists of 2 or more alveoli that share a common opening. Type I and type II alveolar cells line the alveolar wall along with alveolar macrophages (dust cells). Type II alveolar cells secrete alveolar fluid with surfactant. Surfactant lowers the surface tension of the alveolar fluid and prevents the alveoli from collapsing. Respiratory Membrane The alveolar walls and capillary walls form the respiratory membrane. Exchange of O2 and CO2 takes place here. The respiratory membrane is very thin, which allows for rapid diffusion of gases. The lungs contain an estimated 300 million alveoli, providing a surface area of about 70m2 for the exchange of gases. Nebulization Nebulization is a treatment that administers medication in the form of droplets suspended in air to the respiratory tract. The patient inhales the medication as a fine mist. Various drugs are used. Some relax the smooth muscles of the respiratory tract, some reduce the thickness of mucous, and antibiotics are used. Blood Supply To The Lungs Deoxygenated blood passes from the right ventricle into the pulmonary trunk, which divides into a left and right pulmonary artery. Four pulmonary veins return oxygenated blood to the left atrium. Blood Supply To The Lungs Pulmonary blood vessels constrict in the presence of hypoxia (low O2) unlike blood vessels elsewhere in the body. This shunts blood from poorly ventilated areas of the lung to well-ventilated regions. This is known as ventilation-perfusion coupling because the perfusion (blood flow) matches the ventilation (air flow) to an area. Blood Supply To The Lungs Bronchial arteries, which branch from the aorta, deliver oxygenated blood to the lungs. This blood perfuses the walls of the bronchi and bronchioles. Pulmonary Ventilation Respiration (gas exchange) occurs in 3 steps: Pulmonary ventilation (breathing) – the mechanical flow of air into (inhalation) and out of (exhalation) the lungs. External respiration – the exchange of gases between the air spaces of the lungs and the blood in the capillaries. Internal respiration – the exchange of gases between the blood in systemic capillaries and tissue cells. Pulmonary ventilation (breathing) is the process by which gases flow between the atmosphere and the lung alveoli. Inspiration & Expiration Pressure Changes During Pulmonary Ventilation Air moves into the lungs when air pressure in the atmosphere is greater than air pressure in the lungs. Air moves out of the lungs when the pressure inside the lungs is greater than the pressure in the atmosphere. Inhalation Breathing in is called inhalation (inspiration). Increasing the volume of the lungs causes inhalation. Contraction of the diaphragm and the external intercostals expands the lungs. Boyles Law The pressure of a gas in a closed container is inversely proportional to the volume of the container. If the size of a closed container increases, the pressure inside the container decreases. If the size of a closed container decreases, the pressure inside the container increases. Muscles Of Inhalation The most important muscle of inhalation is the diaphragm. The next most important muscles in inhalation are the external intercostals. Exhalation Breathing out is called exhalation (expiration). Elastic recoil of the chest wall and lungs causes exhalation. Recoil of the elastic fibers that were stretched during inhalation. The inward pull from surface tension of the film of alveolar fluid. Active Exhalation Exhalation becomes active only during forceful breathing such as when playing a wind instrument or during exercise. The muscle of exhalation then contract. Abdominals. Internal intercostals. Factors Affecting Pulmonary Ventilation Surface tension of alveolar fluid. A deficiency in surfactant in premature infants causes respiratory distress syndrome. Factors Affecting Pulmonary Ventilation Compliance of lungs refers to how much effort is required to stretch the lungs. Decreased compliance results from scar tissue (TB), excess fluid (pulmonary edema), a deficiency in surfactant, or paralysis of muscles of inspiration. Airway resistance – any condition that narrows or obstructs airways increases resistance. Chronic obstructive pulmonary disorders (COPD) such as asthma, emphysema, or bronchitis increase airway resistance. Breathing Patterns Eupnea – a normal pattern of quiet breathing. Costal breathing – shallow (chest) breathing. An upward and outward movement of the chest due to contraction of the external intercostal muscles. Diaphragmatic breathing – deep (abdominal) breathing consisting of outward movement of the abdomen from contraction and descent of the diaphragm. Modified Respiratory Movements Coughing Sneezing Sighing Yawning Modified Respiratory Movements Sobbing Crying Laughing Hiccuping Valsalva maneuver Lung Volumes & Capacities Tidal volume (VT)– the volume of one breath. Minute ventilation (MV) is the volume of inhaled and exhaled air in one minute. It is determined by multiplying the respiratory rate by the tidal volume. A spirometer or respirometer are utilized to measure the volume of air used. A spirogram is the record of this volume. Lung Volumes & Capacities Typically, about 70% of the tidal volume reaches the respiratory portion of the respiratory system. The remaining airways are known as the anatomic dead space. By inhaling deeply, you can take in additional air (inspiratory reserve volume). Lung Volumes & Capacities The expiratory reserve volume is the additional air from a forced exhale. Even after a forced breath, some air remains. This is the residual volume. Lung Volumes & Capacities The inspiratory capacity is the sum of the tidal volume and the inspiratory reserve volume. The functional residual capacity is the sum of residual volume and expiratory reserve volume. Vital capacity is the sum of inspiratory reserve volume, tidal volume, and expiratory reserve volume. Total lung capacity is the sum of vital capacity and residual volume. External Respiration External respiration or pulmonary gas exchange is the diffusion of O2 from air in the alveoli of the lungs to blood in pulmonary capillaries and the diffusion of CO2 in the opposite direction. External respiration converts deoxygenated blood coming from the right side of the heart into oxygenated blood that returns to the left side of the heart. External respiration occurs only in the lungs. Internal Respiration Internal respiration or systemic gas exchange is the exchange of CO2 and O2 between the systemic capillaries and tissue cells. Internal respiration occurs in tissues throughout the body. Oxygen Transport Oxygen does not dissolve easily in water. Most of the blood O2 is bound to hemoglobin. Oxygen and hemoglobin bind in an easily reversible reaction to form oxyhemoglobin. Carbon Monoxide Poisoning Carbon monoxide CO is a colorless and odorless gas found in exhaust fumes from automobiles, gas furnaces, space heaters, and tobacco smoke. CO binds to hemoglobin about 200 times as strong as O2 and uses up the available hemoglobin molecules. Carbon Monoxide Poisoning Bright, cherry red color of the lips is a sign. Administering pure oxygen speeds up the dissociation of CO from hemoglobin and can save a persons life. Respiratory Center The respiratory center in the brain stem controls the basic rhythm of respiration. 3 areas: Medullary rhythmicity area – controls the basic rhythm. Inspiratory and expiratory areas. Pneumotaxic area – impulses turn off the inspiratory area before the lungs become too full. Apneustic area – activates the inspiratory center and prolongs inspiration. Chemoreceptor Regulation Chemoreceptors regulate the levels of O2 and CO2. Central chemoreceptors are located in the medulla oblongata. Peripheral chemoreceptors are located in the aortic bodies and carotid bodies. Hypoxia A deficiency of O2 at the tissue level. 4 types: Hypoxic hypoxia – low PO2 in arterial blood from high altitude, airway obstruction or fluid in the lungs. Anemic hypoxia – too little hemoglobin due to hemorrhage, anemia, CO poisoning. Ischemic hypoxia – blood flow to a tissue is reduced. Histotoxic hypoxia – tissues cannot use O2 properly due to some toxic agent (I.E. Cyanide poisoning). Influences On Respiration See page 840 in text.