Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
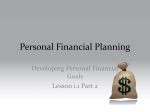
Health Care Spending Growth Michael Chernew April 18, 2012 Definitional issues matter Focus on spending at the population (national) level (i.e., Price x Quantity), not – Spending per unit of service [i.e. Price] – Cost of producing a unit of service – Spending for a disease cohort Distinguish between total spending or government spending – Total spending is the most comprehensive – Government spending causes most alarm Taxes Data Health Care Spending is not Sustainable National Health Expenditure as % of GDP 20 18 16 % of GDP 14 12 10 8 6 4 2 0 1960 1965 1970 1975 1980 1985 1990 1995 2000 2005 Excess Spending Growth 19401950 19501960 19601970 19701980 19801990 19902000 20002009 Average annual growth in per capita health expenditures Average annual growth in per capita GDP Excess growth in health expenditures 4.0% 3.6% 5.6% 4.2% 4.9% 3.0% 3.2% 3.1% 1.5% 2.7% 2.0% 2.0% 2.1% 0.5% 0.9 2.1 2.9 2.2 1.4 0.9 2.7 Share of per capita Income Growth Devoted to Health Care 5.3% 5.5% 12.9% 16.5% 25.5% 18.7% 91.5% 2005 Dollars (adjusted using GDP deflator) Source: Spending and population data obtained from Centers for Medicare & Medicaid Services National Health Expenditures Data, 2011 and Newhouse (1992). Consequences of Higher Taxes If finance higher health care spending by taxes: – Marginal tax rates of high income earners could rise to 70% by 2060 – GDP declines(relative to trend) by 11%. Magnitudes depend on the exact assumptions about tax policy Source: Baicker and Skinner: 2011: Assumes health care spending growth consistent with 2010 CBO long run forecast Private Health Care Spending is not Sustainable Concepts and Evidence Slowing spending growth Spending High spending, rapid growth Low spending, rapid growth Low spending, slow growth Time Level vs. Growth Change in Medicare Spending vs. Percentage PCPs Drivers of Spending Growth Could obesity be driving spending Probably contributes to spending growth The effects interact with technology Costs were growing faster than real GDP for EVERY 10 year period since WWII – Even before obesity epidemic If the only change between 1987 and 2001 were BMI, then real, per capita spending would have risen ~ 1%/ year Long run drivers of spending growth Medical technology – New knowledge (and associated stuff) Less important factors – Prices – Aging – Rising incomes – More generous coverage (static effects) – Inefficiency – Inappropriate use – Liability Types of technology changes 1951 - 1971 : little ticket items – lab tests – X-Rays 1971 - 1981 : big ticket items – CABG – C-section – radiation & chemotherapy for breast cancer Early and Mid 1990s – Pharmaceuticals 2000’s – Imaging, – Biologics Myth: In Other Industries Technology Lowers Spending Do not confuse price (cost per unit) with overall spending – Computers Prices fall: Spending rises Demand is crucial to determine effects of technology on spending Benefits May Justify Cost Slowing spending growth requires us to slow growth in price or quantity Determining when to apply medical technologies is crucial Average value of technology (widely viewed as great) may differ from marginal value (may be small) – Knowing when to apply technology is crucial Our goal must be to promote ‘value’ Technology Reflects the System Insurance Cost Containment Can we change the system to preserve innovation but manage new knowledge more efficiently? Implications Reductions in the level of spending are important, maybe VERY important, but… Determinants of spending growth often differ from determinants of level of spending Strategies to control spending growth must be either: – Continual one time savings – Fundamental environmental change Public spending growth can be controlled by shifting spending to patients