Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
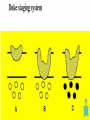
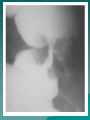
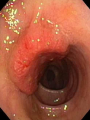
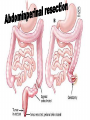
Cancer colon and rectum (Incidence) General 2nd common after brochogenic carcinoma in men 4th common in females Age – Abroad old – Egypt 40y Etiology Of Colon Cancer Hereditary nonpolyposis colon cancer 5-6% Sporadic Colon Cancer 92% Chronic IBD 1% Familial Adenomatous polyposis and rare syndromes 1% Cancer colon and rectum (Etiology) Diet – Diet lacking vegetables – Low residue diet---increase constipation – High fiber diet----increase bile--carcinogens – Cooked meat -----carcinogens Precancerous lesions – Polyps--- tubuls, villous, FAP – IBD – Uretrocolic anastomsis Familial Adenomatous Polyposis (FAP) Autosomal dominant inheritance of mutated APC gene in chromosome 5 Hundreds to thousands of colorectal adenomas, average age of onset 16 Colon cancer by age 45 (mean age 39, &% by age 21) Familial Adenomatous Polyposis (FAP) Genetic tests, counseling age 10 to 12 Flexible sigmoidoscopy – annually or biannually for positive genetic test Colectomy when adenomas develop Hereditary Nonpolyposis Colorectal Cancer Syndrome (HNPCC) Autosomal dominant inheritance of altered mismatch repair gene Cancers preceded by a few rapidly growing adenomas Cancers multiple, proximal, younger age of onset Cancer colon and rectum (pathology) 3% 5% 3% 5% 5% 12 % 7% 2% 38% 21% Pathology ( NEA) Pathology (MP) Adenocarcinoma 95% – Well differentiated – Moderately differentiated – Poorly differentiated Mucoid or colloid signet ring Squamous cell carcinoma Rare types Stage 0 Colorectal Cancer Known as “cancer in situ,” meaning the cancer is located in the mucosa Removal of the polyp (polypectomy) is the usual treatment Stage I Colorectal Cancer cancer has grown through mucosa and invaded the muscularis (muscular coat) Treatment is surgery to remove the tumor and some surrounding lymph nodes Stage I Colorectal Cancer Stage II Colorectal Cancer The cancer has grown beyond the muscularis of the colon or rectum but has not spread to the lymph nodes Stage II Colorectal Cancer Stage III Colorectal Cancer The cancer has spread to the regional lymph nodes (lymph nodes near the colon and rectum) Stage III Colorectal Cancer Stage IV Colorectal Cancer The cancer has spread outside of the colon or rectum to other areas of the body Stage IV Colorectal Cancer Stage IV Colorectal Cancer Stage IV Colorectal Cancer Methods of spread Intramural spread – Spread is three-dimensional; the distal margin is of great concern in low rectal cancers (2-3 cm are considered enough) Extension to adjacent structures Lymphatic spread – – – – N N N N 1 2 3 4 Epicolic paracolic intermediate (SMA, IMA) central groups of LN (para Aortic). IMA Superior rectal Internal iliac Middle rectal Inferior rectal Inguinal LN Methods of spread Hematogenous spread – Predominantly to the liver – The lung is the second affected organ Transperitoneal spread – Seedlings – malignant ascites – omental deposits – Specially occurring in mucinous cancer and is beyond surgical cure. Clinical picture of cancer Colon & Rectum Alteration in bowel habit Sever form mainly constipation Alteration in bowel habit in the form of mild diarrhea Anemia, which is quite severe Intestinal obstruction is late A mass felt in advanced cases Complication of Acute appendicitis Intussussption Perforation hge Vague upper abdominal pain Intestinal obstruction early A mass felt in early cases Complication of Perforation hge 1- Rectal bleeding most frequent presentation. 2-Sense of incomplete evacuation 3-Tenesmus is prominent in rectal cancer 4- Recent alteration in bowel habit (increasing constipation alternating with diarrhea or spurious morning diarrhea Signs Cancer colon General – Anaemia & loss of weight – Virchow’s LN – Oedema of LL Abdominal – Abdominal Mass – Liver mass – Ascites – PR & PV Krukenberg Plummer’s shelf Cancer Rectum General – Anaemia & loss of weight – Lung metastases Abdominal – Liver mass – Ascites – PR Mass in the rectum 90 % of cases Investigations Laboratory – – – – Liver function CBC anaemia Stool for occult blood Tumor markers (CEA &Ca19) Investigations Radiological – – – – Proctosigmoidoscopy – Chest x ray or CT Double contrast barium enema Ultrasonography for the liver and LN CT or MRI which will more accurately delineate the LN and perirectal fat Diagnose almost 50% of the cases Colonoscopy – It is the gold standard Rectal cancer Cancer colon Cancer caecum Cancer sigmoid General Rules (1) Preoperative preparation Traditional –Pre –Pre –Pre –Pre –Pre by by by by by 5 4 3 2 1 method days ----- low residue diet days ----- low residue diet days ----- fluid only days ------ NPO days ------ NPO Mechanical & Chemical General Rules (1) Preoperative preparation Mechanical –Laxative at night 60 cm parrafin –Cleaning enema up to 4 time per day Chemical –Neomycin –Erythromycin –Metronidazole General Rules (1) Preoperative preparation Rapid method –Polyethylene glycol can be drunk or given through NG Tube 2-3 liters over 24 hours –Alternatively (in urgent cases) on table lavage using appendix stump as a portal of entry can be very effective General Rules (2) Radical resection Any surgical resection requires 5 cm proximal and 2 cm distal clearance for colonic lesions Radial margin should be histopathologically free of tumor if possible Lymph node resection should be performed to the origin of the feeding vessel General Rules (3) During resection 1. 2. 3. 4. 5. Surgical resection requires 5 cm proximal and 2 cm distal clearance for colonic lesions Early vein ligation High artery ligation Non touch technique En block resection General Rules (3) Asses operability 1. 2. 3. 4. 5. Tumor mobile or fixed LN involvement Peritoneal; seedlings Malignant ascites Liver metastases Depending on site of lesion surgical options Caecum, ascending colon,– Right hemicolectomy hepatic flexure --Extended right hemicolectomy Transverse colon – transverse colectomy or Extended right hemicolectomy Splenic flexure, descending colon – Left hemicolectomy Sigmoid colon – sigmoidectomy or Anterior resection Caecum Cancer rectum Upper 1/3 --–Anterior resection Lower 1/3 –Abdomino-perineal resection with proximal permanent stoma Cancer rectum Middle 1/3 --–Abdomino-perineal resection with proximal permanent stoma –Low Anterior resection with stapler –Sphincter saving options Abdoinosacral approach Pull-through with trans-anal colo-anal anastmosis Rectal Dissection Anterior Rectal Dissection Posterior –Low Anterior resection with stappler –Low Anterior resection with stappler