Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
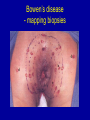
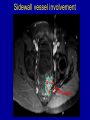
Surgery for Anal Cancer Peter Sagar The General Infirmary at Leeds Where is the anal canal? • Perianal cancer • Anal canal cancer Anal canal Perianal neoplasms • Perianal skin – junction of the hair-bearing skin and anoderm of the anal canal Perianal neoplasms • • • • Squamous cell carcinoma Basal cell carcinoma Bowen’s disease Perianal Paget’s disease Squamous cell carcinoma • • • • • Rolled everted edges Central ulceration Late diagnosis 30% misdiagnosed Spread to lymph nodes Perianal squamous cell carcinoma - treatment • Wide local excision – well differentiated, up to 3 cm • Less favourable lesions- chemoradiation (40-70 Gy) Perianal basal cell carcinoma • • • • • • Uncommon 1-2 cm Rarely metastasize Misdiagnosed in 33% Delayed diagnosis Rx – local excision with adequate margins Bowen’s disease • Intraepidermal squamous cell carcinoma • Associated with primary internal malignancies (5%) • Discrete scaly or crusted plaques Bowen’s disease - mapping biopsies Bowen’s disease - excise deep to subcutaneous fat Perianal Paget’s disease • Extramammary Paget’s found in axilla and anogenital region • Uncommon • Eczematous lesions • Visceral carcinomas in 50% Perianal Paget’s disease - biopsy & identify Paget’s cells Perianal Paget’s disease - Excise deep to subcutaneous fat & up to dentate line Outline of flaps Arrowhead flaps Flaps sutured to anal canal Y shaped flaps at completion Squamous cell carcinoma of the anal canal • Long h/o minor perianal symptoms • 33% misdiagnosed • Assess primary lesion • Examine groins • Proctoscopy • Endoanal ultrasound • MRI Squamous cell carcinoma of the anal canal • Spread determined by dentate line • 20% nodal involvement at presentation • Extensive Ca may invade muscular/bony walls of the pelvis Squamous cell cancer - treatment • Local excision • CHEMORADIATION • Abdominoperineal resection Inguinal lymph node • No indication for prophylactic groin dissection • Ominous sign if present at presentation • Rx chemoradiation to groin nodes Patient Numbers Total Number of Patients 188 Not treated with XRT Treated with XRT 13 175 50Gy 110 49.9-30.1Gy 9 30Gy <30Gy 39 17 Clinical Stage - primary 50 45 40 35 30 No 25 20 15 10 5 0 T1 T2 T3 Stage T4 Clinical stage - nodes 80 70 60 50 No 40 30 20 10 0 N0-1 N2-3 Nodal stage Patterns of failure 14 12 10 8 6 4 2 0 Local Distant Both TIME TO LOCAL FAILURE 14 12 10 8 6 4 2 0 3/12 - 6/12 6/12 - 12/12 > 1YR Local control 1,1 1,0 ,9 Local control ,8 ,7 ,6 ,5 ,4 ,3 ,2 ,1 0,0 0 20 40 60 Time (months) 80 100 Overall survival 1,1 1,0 ,9 ,8 ,7 ,6 ,5 ,4 ,3 ,2 ,1 0,0 0 20 40 60 Time (months) 80 100 Overall survival by stage 1,2 T1 1,0 ,8 T2 T3 ,6 T4 ,4 ,2 0,0 0 20 40 60 Time (months) 80 100 Local control by stage 1,1 1,0 ,9 ,8 ,7 ,6 ,5 T4 ,4 ,3 ,2 ,1 0,0 0 20 40 60 Time (months) 80 100 Salvage Surgery Treated to 50Gy 110 Local recurrence 23 Number had salvage surgery 13/23 Alive and well 5 Dead disease 6 Dead other 2 Patterns of failure • Anal area or regional lymph nodes • APER for residual or recurrent carcinoma • Fixed disease at time of Rx failure, median survival = 8 mths APER for local failure of treatment • Not easy Technical tips • Fill the hole • Tackle pelvic side wall involvement • Sacral invasion Rectus abdominus flap Sidewall vessel involvement vessels Pelvic side wall • BLEEDING • • • • Suture Fibrillar surgicell Argon beamer Be prepared to pack Direct invasion of the sacrum • Choose level of sacrectomy carefully • Frozen section • Beware bleeding from pre-sacral veins APR+S vs TPE+S Summary • High index of suspicion • Mapping biopsies (4 or 12 quadrants) • Excision biopsy • Failure of local treatment = referral to specialist centre Anorectal melanoma • Depressing • Third most common site • Confused with thrombosed haemorrhoid • Spread submucosally WLE vs APER • 428 patients • WLE n=90, APER n=189 • Free of disease at 5yrs: – WLE = 8% – APE = 13%