Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
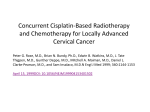
Advanced Stage of Anal Squamous Cell Carcinoma. A Case Report Anamaria Rusu1, Tănase Timiş2, Raluca Popiţă3, Gabriel Kacsó4,5 Institute of Oncology „Ion Chiricuta”, Departments of 1) Radiation Oncology; 2) Medical Oncology, 3) Radiology, 4) Brachytherapy; 5) University of Medicine and Pharmacy „Iuliu Hatieganu” Cluj, Romania Carcinoma of the anal canal accounts for 2% of digestive-system cancers, with squamous cell carcinoma the most common histological type. Combination chemotherapy and radiotherapy is firmly established as the primary therapy for patients with locally advanced squamous cell anal cancer undergoing curative-intent treatment, with anal sphincter preservation in most patients. We present the case of a 42 year old woman, T4N2Mo G3 squamous anal carcinoma, achieving a complete response after external beam radiotherapy concomitant with Capecitabine and Cisplatin, plus interstitial brachytherapy boost and adjuvant chemotherapy. Key words: curative conservative therapy, squamous anal cancer Introduction Carcinoma of the anal canal accounts for 2% of digestive-system cancers, with squamous cell carcinoma the most common histological type. Five-year survival rates range from 78% in patients with local stage disease to only 18% in patients with distant metastases (1). Combined modality therapy consisting of concurrent 5-FluroUracil (5FU), Mitomycin C (MMC) and radiation therapy (RT) is the standard of care for advanced stages of anal squamous cell carcinoma (2). There is no consensus on the optimal dose of RT and of the alternatives of concomitant Cisplatin based regimens. Case report A 42 year old Caucasian woman with no history of significant pathology complained of narrow, bloody stools and anal pain, persisting for 3 months. At presentation the patient had a good general condition ECOG 1 (due to mild symptoms) without weight loss, BMI of 21.5 Kg/m2. Clinical findings were scarce: sensibility at palpation of the lower abdomen left colic chord with no superficial enlarged lymph nodes. Digital rectal examination (DRE) revealed an exophytic tumor of the posterior wall of the anal canal and lower rectum, fixed, with sphincter invasion, which covered a length of 6 cm from the anus, 3.5 cm large and 2 cm in Journal of Radiotheraphy & Medical Oncology August 2012 Vol. 18 No 1: 36-40 Address for correspondence: Gabriel Kacsó, MD, PhD Brachytherapy Department “Ion Chiricuta” Cancer Center Cluj- Napoca, Romania Email: gabi.kacso @gmail.com thickness. The CBC, renal and liver functions were in the normal range as well as squamous cell carcinoma antigen (SCC-N). The HIV antibodies were negative; HPV was not done due to lack of reagents. At recto-colonoscopy the patient was found to have a 5 cm maximum diameter tumor into the posterior wall of the anal canal associated with internal hemorrhoids. The tumor presented an irregular contour with ulcerated areas and infiltration into the low rectum. The rest of the colon was normal. Biopsy of the anal tumor concluded on a poor differentiated squamous cell carcinoma (Fig. 1). Abdominal ultrasound and chest X-ray did not show liver or lung metastases. Enhanced Magnetic Resonance Imagery (MRI) revealed a tumor of 5.8 cm in length /3.2 cm large / 2 cm in depth, invading the levator anal muscle, one right internal obturator lymph node (LN) of 17 mm diameter and several internal iliac LN with a maximum diameter of 8 mm (Fig 2). The final diagnosis was squamous cell carcinoma of the anal canal, T4N2M0, stage III; ECOG1, no co-morbidities. Fig. 1. Poor differentiated (G3) squamous cell carcinoma at 10 x magnification, hematoxilin-eosine (courtesy of Dr. Ferariu). Locally advanced anal squamous carcinoma The case was discussed in multidisciplinary round table and concurrent chemo-radiation (CRT) was decided. After informed consent, the patient received conformal external beam radiation (EBRT) 45Gy / 25fr / 33day to the posterior pelvis in a prone position, concomitant with daily oral Capecitabine 825 mg/sqm twice daily (daily dose of 1650 mg) and weekly iv. Cisplatin 30mg/sqm. We used a 3 field technique with wedges on the transversal fields in order to minimize the urinary and sexual toxicity (to lower the irradiation of the bladder, the vulva and the vagina). The internal iliac and obturator LN received additional 10Gy/5fr conformal RT and the inguinal LN were boosted bilaterally in a supine position by direct anterior fields with electrons, 12 MeV (according to the depth of the femoral vessels on the scanner), 3Gy/fr, 2 fr/ wk to achieve a total dose of 45 Gy. Using the CTCAEv.3.0 scale, we recorded a G3 perineal acute toxicity (skin) which healed within 15 days after the end of the EBRT; G1 gastrointestinal toxicity (diarrhea) and G1 leukopenia. Two weeks after CRT, the MRI concluded on a major partial remission of 90%. One week later we delivered a radiation boost by interstitial HDR Iridium 192 brachytherapy (BT). In spinal anesthesia, 9 needles were implanted, 2 hemi-circumferential parallel rows (5 inner and 4 outer).The external arch was justified by the initial distal infiltration into the levator anal muscle. The needle 37 was loaded on 5 cm length and she received DT=12 Gy /3fr /2 days (Fig. 4).The patient subsequently had three cycles of adjuvant chemotherapy Capecitabine 2000mg/sqm daily, D1-14/q21 plus Cisplatin 75mg/sqm/D1/q21, with upper digestive tract toxicity G3 (vomiting) and mild hematologic toxicity (leukopenia- G2, neutropenia- G1). Three months after the end of chemotherapy, she was in complete remission (clinically, at ultrasound and MRI Fig. 3), with excellent anal and bladder continence and no late toxicity > G1. She was offered hormonal replacement therapy for alleviating the symptoms of radiation induced menopause. Discussion The incidence of anal squamous cell carcinoma has increased both in men and women during the last three decades, associated with HIV and human papilloma viruses (HPV), with the diagnosis at younger age (as was our patient but not HIV related). We did not perform a HPV genotyping. There is no data concerning the possible favorable prognosis of HPV related anal carcinoma treated by chemoradiation, as it is demonstrated for the same histological type in head and neck cancers (3). Local and lymphatic extension are the most common routes of spread, the vascular dissemination being less Fig. 2. Transversal, coronal and sagital MRI view before treatment (arrows indicating the tumor). Fig. 3. Transversal, coronal and sagital MRI view showing complete remission after chemoradiation, brachytherapy and adjuvant chemotherapy. 38 Rusu et al Fig. 4. Oblique radiography of palisade of hollow 9 needles in 2 plans surrounding the anus and lower rectum with related dosimetry (in red is the100% prescription isodose). common, although the latter is higher among patients with advanced disease. Direct invasion into the sphincter muscles and perianal connective tissue occurs early in the course of the disease, and about one-half of patients present with tumor invasion of the rectum, peri-anal region or both. This was one of the reasons why we delivered a radiation boost by interstitial HDR brachytherapy with needles in 2 plans. Tumors in the distal canal drain to the inguinal–femoral, the external and common iliac nodal regions. About 15% of patients have clinical evidence of inguinal lymphnodes (LN) at presentation and involvement is usually unilateral. However, microscopic invasion into the inguinal LN occurs in up to 60 % of advanced stages. It was not surprising therefore that we did not find clinically enlarged inguinal LN but we designed the RT plan in order to cover them as elective target volume. Advances in radiation techniques and seminal studies combining chemotherapy and radiation have led to their use as standard definitive treatment for advanced stages of anal squamous carcinoma, reserving surgery for recurrent or persistent disease. The ability of radiation or chemoradiation treatment over surgery alone in achieving local tumor control while preserving the ano-rectal function without sacrificing survival has served as a model for organ preservation in other types of cancer (4). In a trial conducted by the UK Coordinating Committee for Cancer Research (5), patients were randomized to receive radiation alone or combined-modality therapy. The total dose (TD) was 45Gy in 20 to 25 fractions over 4 or 5 weeks. The combined-modality group was given radiation in combination with 5-FU and Mitomycin C on the first day of each course of chemotherapy. If the tumor had not regressed by at least 50% at 6 weeks after the CRT, surgery or further radiation (15Gy /6 fr to a perineal field or an interstitial implant of 25Gy/ 2-3 day) was considered. The local recurrence rates were 36% in the combined-modality group and 59% in the radiation-only group. Another trial conducted by EORTC (6) that compared radiation alone versus CRT. Radiation was given to a total dose of 45Gy over 5 weeks; chemotherapy included 5-FU given as a continuous infusion during the first and fifth week of radiation and Mitomycin C given as an intravenous bolus on the first day of each course of chemotherapy. After 6 weeks, a boost dose of radiation by EBRT or interstitial techniques was given (15 Gy for complete response and 20 Gy for partial response).Tumor regression rates were significantly higher in the CRT group. The colostomy-free survival rate at 5 years was 70% for the CRT group and only 52% for the treated with radiation alone. These trials have shown significant improvements from the addition of chemotherapy to radiation in terms of primary tumor control and colostomy-free survival rate but not in terms of overall survival rate. Concerns over the hematologic toxicity of Mitomycin C and its long-term effect have led to the use of cisplatin with 5-FU for the treatment of anal cancer. This combination showed complete response rates of 90% to 95% and colostomy-free survival rates of 86% at 3 years. The toxicity of Cisplatin and 5-FU seemed to be more limited (7). A phase III Gastrointestinal Intergroup study (RTOG 9811) compared radiation therapy with concurrent 5-FU and MMC versus two courses of induction 5-FU and Cisplatin followed by concurrent radiation with 5-FU and Cisplatin (8). Radiation doses up to 59 Gy were allowed for patients with T3-T4 or node positive disease. Rate of loco regional control, disease-free survival, overall survival, acute nonhematologic toxicity and long–term toxicity were similar in both treatment groups. Severe acute hematologic toxicity was significantly worse in the MMC group (61% versus 42%). However, the cumulative colostomy rate was lower in the MMC than in the Cisplatin group (10% versus 19%). Results from the ACCORD-03 randomized phase III clinical trial also suggest that there is no benefit of chemotherapy given prior to chemoradiation. In this study patients with locally advanced anal cancer were randomized to receive induction therapy with 5-FU/cisplatin or no induction therapy followed by chemoRT (they were further randomized in order to receive an additional radiation boost or not). No differences were observed between tumor complete response, tumor partial response, 3-year colostomy-free survival, local control, event-free survival, or 3-year overall survival (9). Results from recent phase III trials in anal cancer have Locally advanced anal squamous carcinoma failed to show any benefit for neoadjuvant chemotherapy (NACT) with cisplatin, or cisplatin-based consolidation CT compared to CRT alone for loco-regional control, diseasefree survival (DFS) and overall survival (OS). In total, for CRT, 103 retrospective/observational studies, four phase I/II studies, 16 phase II prospective studies, two randomised phase II studies, and six phase III trials of CRT in anal cancer were identified (10). Only three phase II CT studies in metastatic disease were identified. Few retrospective studies were consistent in their use of CT or radiation doses, and long-term follow-up (> 3 years) was rare. In anal cancer T3/T4 lesions fare badly (3 year DFS 40-68%). Cisplatin appears an effective drug, but novel strategies have not allowed progress against MMC, infusional 5FU and radiotherapy. New substances such as capecitabine and oxaliplatin have been tested in phase II trials. Because anal cancer overexpresses the epidermal growth factor receptor (EGFR) and a KRAS wild type is usually present, treatment with the EGFR antibody cetuximab is potentially interesting. Phase I trials have shown that the combination with RCT is practicable; however, phase II trials have not yet been carried out (11). EBRT with 5 FU and cisplatin and an interstitial implant has been effective in treating anal cancer. In a long–term study conducted in France, this strategy resulted in colostomy-free survival rates of 71% at 5 years and 67% at 8 years (12). There is an increasing body of literature suggesting that toxicity can be reduced with advanced radiation delivery techniques. There is considerable interest in the use of IMRT for anal cancer. A dosimetric comparison of IMRT and conventional radiation-treatment plans showed that using IMRT resulted in a reduction of dose to the femoral head and neck and to the external genitalia, with comparable coverage of tumor volume (13-15). Based on results of three recent randomized phase III trials, neither induction chemotherapy (RTOG 98-11, ACCORD 03) or RT dose escalation (ACCORD 03) improved the outcome of concurrent 5-FU/MMC-CRT. A randomized phase II trial (EORTC 22011-40014) compared concurrent 5-FU/MMC-CRT with cisplatin/ MMC-CRT. The response rate of cisplatin/MMC-CRT was promising, but compliance to this regimen was limited. Current phase I/II studies are evaluating the use of capecitabine, oxalipatin, and the EGFR (epidermal growth factor receptor) inhibitor cetuximab. Concurrent 5-FU/MMC-CRT without induction or maintenance chemotherapy remains the standard of care for anal cancer patients (19). In this case, the particularities are the chemotherapy regimen and the brachytherapy technique in 2 plans. We combined EBRT to chemotherapy with daily Capecitabine and weekly iv. Cisplatin to maximally increase the radiosensitivity. Capecitabine has proven equivalent efficacy to 5-FU in colon and rectal adenocarcinoma. We adjusted the doses according to the data published for rectal cancers 39 and on the published phase II studies in anal squamous carcinoma. Weekly Cisplatin concomitant to RT is standard for cervix squamous carcinoma. We used a prone position 3 field conformal RT technique with wedges on the transversal fields in order to minimize the urinary and sexual toxicity (to lower the irradiation of the bladder, the vulva and the vagina). The brachytherapy implant was optimized on the shrinkage volume after CRT but the depth of the 100% coverage isodose to the initial infiltration into the levator anal muscle was adapted. Consequently, a two plan implant was required, which is rather unusual for this topography. The adjuvant chemotherapy, although not standard care for advanced stages, has not yet been properly assessed and there is a suggestion that N2 patients (as our case) might benefit more than the T3-4No ones (16). After the end of treatment, a complete remission (clinically, ultrasound and MRI) with a mild profile of toxicity was achieved. Further follow-up is required . Conclusion Combination chemotherapy and radiotherapy is firmly established as a primary therapy for patients with squamous cell anal cancer undergoing curative-intent treatment, with anal sphincter preservation in most patients. Surgery should not be pursued unless clinical evidence of disease progression is shown. Treatment-related toxicity can be significant, causing interruption in treatment that can compromise local control. Strategies to minimize toxic effects and improve rates of local control are being investigated, such as our scheme with brachytherapy boost (instead of EBRT) and the Capecitabine- Cisplatin regimen (instead of 5FU-MMC). References 1. Jemal A, Siegel R, Ward E, et al. Cancer Statistics. CA Cancer J Clin 2008;58(2):71–9 2. Ryan DP, Compton CC, Mayer RJ et al. Carcinoma of the anal. N Engl J Med 2000; 34:792-800. 3. Stina Syrjänen. Human Papillomaviruses in Head and Neck Carcinomas. N Engl J Med 2007; 356:1993-95. 4. Weber DC, Kurtz JM, Allal AS et al. The impact of gap duration on local control in anal canal carcinoma treated by split-course radiotherapy and concomitant chemotherapy. Int J Radiat Oncol Biol Phys 2001; 50:675–80. 5. Glynne-Jones R, Sebag-Montefiore D, Adams R, McDonald A, Gollins S, James R, Northover JM, Meadows HM, Jitlal M; UKCCCR Anal Cancer Trial Working Party. the impact of variations in the duration of the treatment gap and overall treatment time in the first UK Anal Cancer Trial (ACT I).Int J Radiat Oncol Biol Phys. 2011; 81:1488-94. 6. Matzinger O, Roelofsen F, Mineur L, Koswig S, Van Der SteenBanasik EM, Van Houtte P, Haustermans K, Radosevic-Jelic L, Mueller RP, Maingon P, Collette L, Bosset JF; EORTC Radiation Oncology and Gastrointestinal Tract Cancer Groups. Eur J Cancer. 2009; 45: 2782-91. 40 7. Créhange G., Bosset M., Lorchel F., et al: Combining cisplatin and mitomycin with radiotherapy in anal carcinoma. Dis Colon Rectum 2007; 50:43-49. 8. Ajani JA, Winter KA, Gunderson LL et al. Mitomycin, and radiotherapy vs. fluorouracil, cisplatin, and radiotherapy for carcinoma of the anal canal: a randomized controlled trial. JAMA. 2008; 299:1914-21. 9. T. Conroy, M. Ducreux, C. Lemanski, E. Francois, M. Giovannini, F. Cvitkovic, X. Mirabel, O. Bouché, C. Montoto-Grillot, D. Peiffert. France Treatment intensification by induction chemotherapy (ICT) and radiation dose escalation in locally advanced squamous cell anal canal carcinoma (LAAC): Definitive analysis of the intergroup ACCORD 03 trial. J Clin Oncol 2009; 27:15s. 10. Lim F, Glynne-Jones R. Chemotherapy/chemoradiation in anal cancer: a systematic review. Cancer Treat Rev. 2011;37:520-32. 11. Fraunholz I, Rabeneck D, Weiss C, Rödel C. Combined-modality treatment for anal cancer: current strategies and future directions. Strahlenther Onkol. 2010;186: 361-6. Rusu et al 12. Gerard JP, Ayzac L, Hun D, et al. Treatment of anal canal carcinoma with high dose radiation therapy concomitant fluorouracilcisplatinum. Long term results in 95 patients. Radiother Oncol 1998; 41:169-76. 13. Salama J.K., Mell L.K., Schomas D.A., et al. Concurrent chemotherapy and intensity-modulated radiation therapy for anal canal cancer patients: a multicenter experience. J Clin Oncol 2007; 25:4581- 86. 14. Milano MT, Jani AB., Farrey KJ, et al: Intensity-modulated radiation therapy (IMRT) in the treatment of anal cancer: toxicity and clinical outcome. Int J Radiat Oncol Biol Phys 2005; 63:354-61. 15. Devisetty K., Mell .K., Salama JK., et al: Anal cancer treated with intensity modulated radiation therapy (IMRT) and concurrent chemotherapy: a dosimetric analysis of acute gastrointestinal toxicity. Int J Radiat Oncol Biol Phys 2006; 66:S287. 16. Das P, Bhatia S, Eng C, et al. Predictors and patterns of recurrence after definitive chemoradiation for anal cancer. Int J Radiat Oncol Biol Phys 2007; 68:794-800.