Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Myocardial infarction wikipedia , lookup
Electrocardiography wikipedia , lookup
Cardiac surgery wikipedia , lookup
Jatene procedure wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
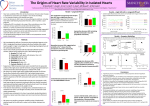
13 Heart Rate Variability 1 Variability of heart rate and regulation of systolic blood. pressure evaluated by fixed rate atrial pacing Joerg Barnstedt, Kilian Tegethoff, Aninka Stellmacher, Jan H. Baumert, Martin Dambacher*, Monika Adt and Axel W. Frey* Deutsches Herzzentrum Berlin, Institut !%r Anaesthesiologie, Augustenburger Platz 1, 13353 Berlin, Germany, *Hen-Zentrum Bad Krozingen, 79188 Bad Krozingen, Germany Introduction: In this study we investigated cardiovascular regulation using spectral analysis of variability of heart rate (HRV) and systolic arterial blood pressure (BPV). It is well known that most of the autonomic regulation of heartbeat effects on the sinus node. Using fixed rate atrial pacing, we wanted to determine the contribution of AV-variability to total HRV and evaluate sympathetic and parasympathetic power in the pacing condition compared with sinus rhythm by analysing spectral power in each frequency band. The routine implantation of temporal atrial pacemaker electrodes after coronary artery bypass graft (CABG) surgery allows us to obtain recordings of ECG and invasively measured arterial blood pressure when correct function of the external pacemaker is checked. In a former study [l], we found that fixed rate atrial pacing reduced HRV substantially but that there was still a residual variability detectable,which we considered to be due to AV-variability, intrinsic cardiac circuits or mechanical effects. The aim of this study was to review these findings and to investigate changes in systolic blood pressure when HRV is abolished by an external pacemaker. As variations in heart rate are an important mechanism of autonomic cardiovascular control, their effect on blood pressure oscillations was evaluated in this study. The particular situation of our patients after cardiovascular surgery was taken into account in this context. Patients and methods: 26 patients were investigated after CABG surgery in the operation room or.shortly after arrival on the ICU. Patients were 43 to 76 years of age. All had normal left ventricular function (Ejection fraction > 50%); patients with reduced renal function, diabetes mellitus, cardiac arrhythmia and thyreotic dysfunction were excluded from the study. No former cardiovascular operation should have been performed on the patients. All patients were still anaesthetized with a combination of benzodiazepindopioidpancuronium and mechanically ventilated with ten to twelve breaths per minute. They were medicated with intravenous dopamine (at a dose of 10 to 30 mg per hour) and nitrates (2.0 to 6.0 mg per hour). Electrodes of the external pacemakers had been implanted in the right atrium at a distance of about two centimeters from the sinus node. During recording of data no other examinations or manoeuvers were allowed to prevent a change in auotonomic balance induced by stress or awakening. ECG and invasively measured arterial blood pressure were recorded in 26 patients by copying ‘Hellige’-Monitor signals with a portable ‘vitaport’-system. Two recordings lasting 150 seconds each were obtained from all patients. During the first recording patients had sinus rhythm of 65 to 88 bpm. After that the atrium was stimulated at 91 to 115 bpm. Discrete Fourier spectral analysis was used to quantifL HRV and BPV. Power spectral density was calculated as the area under the curve for low fiequency spectral density (LF) between 0.003Hz and 0.15Hz and high frequency spectral density (HF) between 0.15 Hz and 0.5 Hz. For the determination of HRV we analysed variability of RRinterval while BPV was analysed by the determination of variability systolic blood pressure (SBP). Power spectra of variability during sinus rhythm were compared with spectra during pacing in LF as well as in HF. Median values of spectral power were compared using Wilcoxon’s matched pairs test. A value of p < 0.05 was considered significant. Results: Mean heart rate increases from 78-bpm to 102Xipm. HRV decreases visibly but isn’t eliminated totally in presence of atrial pacing: Table 1: Changes in HRV; median values, n = 26. LF represents low frequency, HF high frequency power spectral density (ms*/Hz) Sinus rhythm 8.78 9.39 LF HF . Pacing 0.05 1-18 HRV in the low frequencies is diminished to 99.4% of HRV during sinus rhythm and is thus virtually abolished. In the high frequency band the decrease of 87.4% is less distinctive than in the low frequencies. am 0.10 am a+o 0.30 ay1 F K W K V CHd Figure 1: HRV spectra during sinus rhythm (top) and pacing . Example from one patient. Total values of systolic and diastolic blood pressure do not change markedly (Mean values of systolic blood pressure increase from 127.0to 127.3mmHg while diastolic blood pressure increases from 64.7 to 69.3 mmHg). Blood pressure fluctuations appear during pacing in the low frequencies as well as in the high frequencies. In fact, we observed a marked increase of HF BPV while LF BPV changes scarcely and without any statistic significance: Table 2:Changes in BPV; median values, n = 26. LF represents low frequency, HF high frequency power spectral density fmmHe*/Hz).*D<O.OS Sinus rhythm Pacing LF 2.33 2.44 HF 8 21 1 1 81 * . Heart Rate Variability 14 FQEOUENCY I H z l k y r e 2: Systolic BPV spectra changes during sinus rhythm (top md pacing Example of one patient. Discussion: It is widely accepted that low frequency fluctuations in heart rate are mediated by the sympathetic as well as the parasympathetic nervous system whereas. variability in frequencies above approximately 0.15 Hz is dependent on respiration and mediated solely by the parasympathetic system. Parasympathetic influences preponderate over sympathetic effects in the SA node, while there’s no dominance of sympathetic or vagal activity at the AV node [Z]. Fluctuations in the vasomotor tone are caused by baroceceptor feedback, thennoregulatory mechanisms [3] and local adjustments in vascular beds [4]. They are induced by sympathetic activity to the arterioles and conducted via the baroreflex. In the power spectrum, oscillations in the vasomotor tone appear at approximately 0.1 Hz [3]. The analysis of our results of low frequency and high ‘frequency changes in RR-intervals shows that LF HRV is totally eliminated while HF HRV decreases dramatically but still exists. Our current results are comparable to former investigations [I]. Median spectral power in the HF band is diminished to a value of about 10% compared with sinus rhythm. This leads to the conclusion that in the pacing condition sympathetic heart rate variability is totally abolished. The residual variability in the high frequencies could reveal the contribution of AV-variability to total HRV or possibly represent an enhanced vagal tone during pacing. Moreover, mechanical effects caused by atrial stretching or changes in atrio-ventricular volume due to respiration, as they occur in denervated transplanted hearts [5],must be considered to be responsible for the detected HF HRV. All patients in our study are mechanically ventilated with a peak inspiratory pressure of 21 to 34 mbar. As passive ventilation leads to a decrease of total HRV with an increase of respiratory sinus arrythmia in healthy volunteers [6], power spectral density is probably generally reduced in our patients and the relatively high residual HF variability may be enhanced by the passive ventilation. An evaluation of variability of PQ-conduction time would be helpful conduction time would be helphl for a detailed analysis of sympathetic and parasympathetic influence on the lower conduction system of the heart. In fact, we have co!lected such data, but as technical inexactness in pwave detection is probably more distinctive than PQ-variability, an exact determination is still difficult. The arterial blood pressure is regulated by the complex system of baroreflex control. This control mechanism maintains homeostasis by keeping mean blood pressure constant over short periods and adapting it to the demand in’ longer intervals. Changes in cardiac volume loading and cardiac output as well as changes in the muscular tone of the peripheral vessels modulate SBP. The elimination of HRV in our study allows us to evaluate how shortterm heart rate oscillations influence arterial blood pressure. In the low frequencies, where arterial blood pressure increases scarcely during pacing, BPV is caused mainly by the variability in peripheral vasomotor activity. HRV obviously doesn’t modulate blood pressure significantly in this frequency range. Our findings are comparable to investigations in conscious dogs [4]. The power spectral density in the frequencies above approximately 0.15 Hz is strongly influenced by respiration. Changes in vasomotor tone and central venous pressure don’t have any effect on these frequencies [7]. Our findings indicate that normally HF oscillations in heart rate caused by respiration seem to have a marked effect on systolic blood pressure fluctuations. We assume that nomally HF HRV compensates HF blood pressure fluctuations to keep arterial blood pressure as constant as possible. Triedman et al. considered HF fluctuations in blood pressure mainly to be caused by mechanical effects rather than autonomically mediated mechanisms, as experiments during autonomic blockade have shown [7]. The particular hernodynamic status of our patients compared to a normal population must be taken into account as well. All patients are more or less in a state of hypovolemia aRer CABG surgery which is enhanced by treatement with intravenous volume leads to a reduced cardiac output and therefore to a reduced arterial pressure. We detected relatively high oscillations in blood pressure in the low frequencies as well as in the high frequencies which probably represent the rather instable hemodynamic status of all patients after cardiovascular surgery. This effect might be exaggerated by the mechanical ventilation. During positive pressure ventilation, filling of the right heart is reduced and thereby stroke volume and arterial blood pressure decreases. Rooke et al. have show. that during mechanical ventilation hemorrhage, which can also contribute in our patients increases the variability of systolic blood pressure [8]. Conclusions: In consideration of the particular hemodynamic status after CABG surgery we found that: HRV is detectable even during fixed rate atrial pacing and appears only in the high frequencies. Further investigations especially regarding the variability of PQ-conduction time will shed light on the physiological origin of this phenomenon. The regulation of systolic blood pressure is strongly influenced by heart rate variations in the respiration dependent fiequencies. Our fmdings lead to the conclusion that HF HRV is an important regulation mechanism for HF blood pressure fluctuations. Our results might have clinical importance when ability of fast HR modulation is reduced, for example in patients with congestive heart failure or permanently implanted cardiac pacemakers. References: 1, Tegethoff K, Baumert J-H, Frey AW,Adt M: The part of AVnode variability in total heart rate variability evaluated by fixed rate atrial pacing. Computers in Cardiology 1994, Bethesda: IEEE Computers Society Press:3 13-15. 2. Levy MN, Zielske H: Autonomic control of cardiac pacemaker activity and atrioventricular conduction. J Appl Physiol 1969; 27: 447-65 Heart Rate Variability Kitney RI: Beat by beat relationships between heart rate, blood pressure and respiration. Kitney RI and Rompelman (Eds.): The beat by beat investigation of cardiovascular function. Clarendon Press Oxford 1987, 146-178 Akselrod S, Gordon D, Madwed JB,Snidman NC, Shannon C, Cohen RJ: Hemodynamic regulation: investigation by spectral analysis. Am. J. Physiol. 1985;246:H867-H87 Carpeggiani C. Emdin M, Balocchi et al.: Rhythmic heart rate changes in cardiac transplantation. M. Di Rienzo et al. (Eds): Blood pressure and heart rate variability, 10s Press, 1992:242252 15 6. Haggenmiller C, Baumert JH, Adt M, Frey AW: How breathing pattern modulates heart rate. Computers in Cardiology 1994, Bethesda: IEEE Computers Society Press: 753-56 7. Triedman JK, Saul P: Blood pressure modulation by central venous pressure and respiration. Buffering effects of the heart rate reflexes. Circulation. 1994;89: 169-179 8. Rooke G.A., Schwid H. A. Shapira Y: The effect of graded hemorrhage and intravascular volume replacement on systolic pressure variation in humans during mechanical and spontaneous ventilation. Anesth Analg 1995;80:925-32