Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
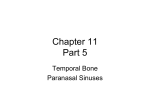
CE ONLINE Optimizing Functional Endoscopic Sinus Surgery Outcomes with Drug Delivery An Online Continuing Education Activity Sponsored By Grant Funds Provided By Welcome to Optimizing Functional Endoscopic Sinus Surgery Outcomes with Drug Delivery (An Online Continuing Education Activity) CONTINUING EDUCATION INSTRUCTIONS This educational activity is being offered online and may be completed at any time. Steps for Successful Course Completion To earn continuing education credit, the participant must complete the following steps: 1. Read the overview and objectives to ensure consistency with your own learning needs and objectives. At the end of the activity, you will be assessed on the attainment of each objective. 2. Review the content of the activity, paying particular attention to those areas that reflect the objectives. 3. Complete the Test Questions. Missed questions will offer the opportunity to reread the question and answer choices. You may also revisit relevant content. 4. For additional information on an issue or topic, consult the references. 5. To receive credit for this activity complete the evaluation and registration form. 6. A certificate of completion will be available for you to print at the conclusion. Pfiedler Enterprises will maintain a record of your continuing education credits and provide verification, if necessary, for 7 years. Requests for certificates must be submitted in writing by the learner. If you have any questions, please call: 720-748-6144. CONTACT INFORMATION: © 2015 All rights reserved Pfiedler Enterprises, 2101 S. Blackhawk Street, Suite 220, Aurora, Colorado 80014 www.pfiedlerenterprises.com Phone: 720-748-6144 Fax: 720-748-6196 Overview Chronic rhinosinusitis (CRS) is a widespread, debilitating disease that can significantly affect a person’s quality of life. The care pathway for patients with CRS involves a complex combination of medical and surgical therapy. While functional endoscopic sinus surgery (FESS) is a recognized treatment for CRS and various sinus disorders, the majority of these patients have symptom recurrence typically within one year after surgery, resulting in poor outcomes. Therefore, numerous perioperative techniques aimed at maintaining surgical outcomes are generally employed to facilitate postoperative outcomes. The purpose of this continuing nursing education activity is to provide a review of the role of drug delivery following FESS in optimizing patient outcomes. An overview of the anatomy and physiology of the paranasal sinuses, followed by the clinical implications of CRS, will be presented. The care pathway for CRS patients will be outlined, including the indications for FESS and the clinical considerations related to continued medical therapy. The various drug classes and routes of administration to the sinuses postoperatively will be reviewed and the clinical support data documented in the literature. Learner Objectives After completing this continuing education activity, the participant should be able to: 1. Explain the anatomy and physiology of the paranasal sinuses. 2. Describe the care pathway for patients with CRS. 3. Identify the indications for various drugs after FESS. 4. Differentiate the options for postoperative drug delivery to the sinuses. Intended Audience This continuing nursing education activity is intended for otorhinolaryngology nurses and other health care professionals who are interested in learning more about innovative drug delivery options for continued medical therapy and improved outcomes in patients following FESS. Credit/Credit Information State Board Approval for Nurses Pfiedler Enterprises is a provider approved by the California Board of Registered Nursing, Provider Number CEP14944, for 2.0 contact hours. Obtaining full credit for this offering depends upon attendance, regardless of circumstances, from beginning to end. Licensees must provide their license numbers for record keeping purposes. The certificate of course completion issued at the conclusion of this course must be retained in the participant’s records for at least four (4) years as proof of attendance. 3 IACET Pfiedler Enterprises has been accredited as an Authorized Provider by the International Association for Continuing Education and Training (IACET). CEU Statements • As an IACET Authorized Provider, Pfiedler Enterprises offers CEUs for its programs that qualify under the ANSI/IACET Standard. • Pfiedler Enterprises is authorized by IACET to offer 0.2 CEUs for this program. ACCREDITATION This program has the prior approval of AAPC for 2.0 continuing education hours. Granting of prior approval in no way constitutes endorsement by AAPC of the program content or the program sponsor. Release and Expiration Date: This continuing education activity was planned and provided in accordance with accreditation criteria. This material was originally produced in January 2015 and can no longer be used after January 2017 without being updated; therefore, this continuing education activity expires January 2017. Disclaimer Pfiedler Enterprises does not endorse or promote any commercial product that may be discussed in this activity. Support Funds to support this activity have been provided by Intersect ENT. Authors/Planning Committee/Reviewer Rose Moss, RN, MN, CNOR Nurse Consultant/Author/Planning Committee C & R Moss LLC Judith I. Pfister, RN, BSN, MBA Program Manager/Planning Committee Pfiedler Enterprises Julia A. Kneedler, RN, MS, EdD Program Manager/Reviewer Pfiedler Enterprises 4 Casa Grande, AZ Aurora, CO Aurora, CO Disclosure of Relationships with Commercial Entities for Those in a Position to Control Content for this Activity Pfiedler Enterprises has a policy in place for identifying and resolving conflicts of interest for individuals who control content for an educational activity. Information below is provided to the learner, so that a determination can be made if identified external interests or influences pose potential bias in content, recommendations or conclusions. The intent is full disclosure of those in a position to control content, with a goal of objectivity, balance and scientific rigor in the activity. For additional information regarding Pfiedler Enterprises’ disclosure process, visit our website at: http://www. pfiedlerenterprises.com/disclosure Disclosure includes relevant financial relationships with commercial interests related to the subject matter that may be presented in this continuing education activity. “Relevant financial relationships” are those in any amount, occurring within the past 12 months that create a conflict of interest. A commercial interest is any entity producing, marketing, reselling, or distributing health care goods or services consumed by, or used on, patients. Activity Authors/ Planning Committee/Reviewer Rose Moss, RN, MN, CNOR No conflict of interest Judith I. Pfister, MBA, RN Co-owner of company that receives grant funds from commercial entities Julia A. Kneedler, EdD, RN Co-owner of company that receives grant funds from commercial entities 5 PRIVACY AND CONFIDENTIALITY POLICY Pfiedler Enterprises is committed to protecting your privacy and following industry best practices and regulations regarding continuing education. The information we collect is never shared for commercial purposes with any other organization. Our privacy and confidentiality policy is covered at our website, www.pfiedlerenterprises.com, and is effective on March 27, 2008. To directly access more information on our Privacy and Confidentiality Policy, type the following URL address into your browser: http://www.pfiedlerenterprises.com/privacypolicy In addition to this privacy statement, this Website is compliant with the guidelines for internet-based continuing education programs. The privacy policy of this website is strictly enforced. CONTACT INFORMATION If site users have any questions or suggestions regarding our privacy policy, please contact us at: Phone: 720-748-6144 Email: [email protected] Postal Address: 2101 S. Blackhawk Street, Suite 220 Aurora, Colorado 80014 Website URL: http://www.pfiedlerenterprises.com 6 INTRODUCTION Chronic rhinosinusitis (CRS) is a widespread disease that represents one of the most common health care problems in the United States today.1 While the precise etiology of CRS remains unclear, mucosal inflammation is understood to be one of the primary underlying causes. In this regard, even minimal inflammation in a localized but critical area (e.g., the ostiomeatal complex) can result in significant pathology in the surrounding areas and trigger widespread sinonasal disease. The care pathway for patients with CRS involves a complex combination of medical and surgical therapy. Functional endoscopic sinus surgery (FESS) is now a wellestablished treatment option for patients with sinus disease; however, despite advances in surgical techniques and equipment, the potential for complications during the postoperative period remains.2 Adverse wound healing in the form of inflammation, mucosal edema, polyposis, adhesions, and middle turbinate (MT) lateralization may result in suboptimal outcomes and the recurrence of both the disease and symptoms postoperatively. Therefore, mitigating these issues has been shown to improve long term patient outcomes.13 Medications used in the management of CRS patients after FESS include antibiotics, oral steroids and nasal steroids. The use of nasal steroids is a beneficial component in postoperative patient management. Steroid-eluting implants may be placed in the ethmoid sinuses to reduce inflammation and maintain sinus patency. ANATOMY AND PHYSIOLOGY OF THE PARANASAL SINUSES In order to understand the role of drug delivery after FESS, it is helpful to first briefly review the anatomy and physiology of the paranasal sinuses and the clinical implications of CRS. Anatomy and Functions of the Paranasal Sinuses The paranasal sinuses are air-filled cavities located within the bones around the nose and eyes that allow for natural ventilation and drainage. There are four sinuses per side (or eight total), named for the facial bones in which they are located (see Figure 1)3: • The ethmoid sinuses, which are a collection of small cells in a honeycomb type structure; and • The peripheral sinuses, ie, the frontal, maxillary, and sphenoid sinuses. These are large cells with one common drainage pathway, the ethmoid sinuses. 7 The ethmoid sinuses, which are a collection of small cells in a honeycomb type structure; and The peripheral sinuses, ie, the frontal, maxillary, and sphenoid sinuses. These are large cells with one comm drainage pathway, the ethmoid sinuses. Figure Sinuses Figure11–– Paranasal Paranasal Sinuses The paranasal sinuses function to: • Humidify and warm inspired air; • Regulate intranasal pressure; • Increase surface area for olfaction; • Lighten the skull; and • Absorb shock. The paranasal sinuses are self-cleansing; goblet cells secrete mucus (up to 1 liter per day). In addition, they are lined with cilia that beat in unison to clear the sinuses (see Figure 2). Figure 2 – Cilia of the Sinuses Chronic Rhinosinusitis (CRS) Chronic rhinosinusitis is defined as persistent inflammation of the sinus membrane; it is frequently classified as with or without polyps (see Figure 3). 8 Figure 3 – Healthy and Diseased Sinus Membranes Today, CRS is a widespread, debilitating disease. It is more prevalent than heart disease and asthma in adults and affects 30 million patients in the United States alone.4 In addition; CRS has a greater impact on a patient’s quality of life than congestive heart failure or chronic back pain.5 Patients with CRS suffer from: • Facial pain and pressure; • Nasal congestion and obstruction; • Loss of smell and/or taste; • Loss of sleep; and • Post-nasal discharge. The average age of a patient with CRS is 40. CARE PATHWAY FOR CRS The CRS care pathway involves a complex combination of medical and surgical therapy (see Figure 4). involves a complex combination of medical and surgical therapy (see Figure 4). The CRS care pathway Figure – CRS Care Pathway Figure 4 – 4CRS Care Pathway Medical Therapy Nasal Steroids Oral Steroids Antibiotics Decongestants Irrigation Surgery to Open Sinuses +/- Balloons Surgical Instruments Balloons Packing 2-3 Follow-up Visits Continued Medical Therapy Nasal Steroids Oral Steroids Steroid-Eluting Implants Antibiotics Decongestants Irrigation Medical therapy consists of nasal steroids, oral steroids, antibiotics, decongestants, and irrigation. Functional endoscopic sinus surgery is performed to open the sinuses; this may require the use of surgical instruments, balloons, and packing, as well as two to three follow-up visits. After sinus surgery, continued medical therapies such as nasal and oral steroids and 9 steroid-eluting implants are often utilized. Of the 1.4 million patients offered FESS annually, only about one-third proceed. Medical therapy consists of nasal steroids, oral steroids, antibiotics, decongestants, and irrigation. Functional endoscopic sinus surgery is performed to open the sinuses; this may require the use of surgical instruments, balloons, and packing, as well as two to three follow-up visits. After sinus surgery, continued medical therapies such as nasal and oral steroids and steroid-eluting implants are often utilized. Of the 1.4 million patients offered FESS annually, only about one-third proceed. Unfortunately, 64% of the patients who have surgery will experience recurrence of symptoms within one year6; in addition, 25% of FESS patients will require more than one procedure to achieve success.7 FESS Functional Endoscopic Sinus Surgery (FESS) is performed to enlarge the sinus passageways to restore drainage and aeration. During this procedure, inflamed bone and tissue in the ethmoid (honeycomb) sinuses are surgically removed. In the peripheral sinuses, the sinus ostia are enlarged surgically or with balloons; this procedure may be performed in the operating room or the surgeon’s office. Figure 5 depicts a patient’s anatomy before and after FESS. Figure 5 – Patient Anatomy Pre-FESS (left) and Post-FESS (right) It is important to note that opening the ethmoid sinuses is key to positive patient outcomes (see Figure 6), because this is where disease originates (especially polyps) and also where the peripheral sinuses drain. Moreover, persistent disease in the ethmoid is the reason for failure of therapy directed at other sinuses.8 Obstruction after FESS is the result of: • Middle turbinate (MT) lateralization (see Figure 7) – this is present in 78% of patients who need revision procedures9. • Adhesions/scarring occur in 14% to 21% of patients within 4 weeks;10 these are present in 56% of patients needing revisions.11 • Disease recurrence of inflammation and/or polyps – this may occur in 60% of patients postoperatively (see Figure 8).12 10 Adhesions/scarring occur in 14% to 21% of patients within 4 weeks;10 these are present in 56% of patients nee revisions.11 Disease recurrence of inflammation and/or polyps – this may occur in 60% of patients postoperatively (see Fig 8).12 Figure 6 – Open Sinus Post-FESS Figure 7 – MT Lateralization Figure 8 – Inflammation/ Figure 6 – Open Sinus Post-FESS Figure 7 – MT Lateralization Figure 8 – Inflammation/Polyps Polyps Open ethmoid cavity MT Septum MT Septum With FESS, FESS, reducing scarring and inflammation postoperatively correlates with the absence the need for further surg With reducing scarring and inflammation postoperatively correlates withofthe absence 13 Additionally, six month outcomes correlate with positive long term outcomes, as symptom reductions attained of the need for further surgery. Additionally, six month 14outcomes correlate with positive longat six mo postoperatively have been shown to be sustained for 20 months. term outcomes, as symptom reductions attained at six months postoperatively have been 14 shown to be sustainedtechniques for 20 months. Numerous perioperative are used to maintain surgical outcomes after FESS; these techniques include mechanical (see Figure 9) and pharmaceutical approaches: Numerous perioperative techniques are used to maintain surgical outcomes after FESS; these Space filling packing material(see usedFigure to create barrier. None of these devices are approved by the United State techniques include mechanical 9)aand pharmaceutical approaches: 15 Septum Food and Drugpacking Administration (FDA) for the of medications. • Space filling material used to localized create aadministration barrier. None of these devices are Steroid-eluting implant. approved by the United States Food and Drug Administration (FDA) for the localized Medications delivered to the mucosa, e.g., antibiotics, as well as oral and topical steroids to control inflammatio 15 administration of medications. discussed below. • Steroid-eluting implant. Figure 9 – Mechanical Techniques to Maintain Surgical Outcomes after FESS • Medications delivered to the mucosa, e.g., antibiotics, as well as oral and topical steroids to control inflammation, as discussed below. Figure 9 – Mechanical Techniques to Maintain Surgical Outcomes after FESS In its January 24, 2014 position statement, the American Rhinologic Society (ARS) endorsed the use of biomaterials approved by the United States FDA; this includes implants and also stents or packing materials used to reduce complic and improve outcomes of sinonasal surgical procedures.16 This statement goes on to add that these biomaterials, amo other potential functions, may have stenting and/or local drug delivery properties and may provide hemostasis or serve surgical dressing. Biomaterials approved by the U.S. FDA for rhinologic application should not be considered investiga decision regarding use of these biomaterials be the Rhinologic responsibilitySociety of the treating physician, considering Intheitsfinal January 24, 2014 position statement, theshould American (ARS) endorsed best available scientific evidence as well as individual patient preference. the use of biomaterials approved by the United States FDA; this includes implants and also stents or packing used to reduce complications and improve outcomes of sinonasal INDICATIONS FORmaterials DRUGS POSTOPERATIVELY surgical procedures.16 This statement goes on to add that these biomaterials, among other potential functions, may have stenting and/or local drug delivery properties and may provide hemostasis or serve as a surgical dressing. Biomaterials approved by the U.S. FDA for rhinologic application should not be considered investigational; the final decision regarding use of these biomaterials should be the responsibility of the treating physician, considering the best available scientific evidence as well as individual patient preference. 11 INDICATIONS FOR DRUGS POSTOPERATIVELY While FESS has undergone major developments over the last 25 years, surgical disruption of the mucosal lining promotes scarring and crusting, which can lead to further inflammation and infection of the sinus mucosa.17 As previously noted, if sinus patency is not achieved and maintained in the early postoperative period, the long term outcome may be compromised. Postoperative care should optimally facilitate an environment which promotes remucosalization of the sinuses, while minimizing inflammation, crusting, infection, and scarring in order to maintain the patency of the surgical site. Scarring and adhesions form primarily within the first two weeks following surgery. Therefore, despite its effectiveness, sinus surgery must be integrated with long term medical therapy in CRS patients for long term success, since the procedure itself does not affect the underlying predisposing causes of the disorder.18 As noted previously, the primary objective of FESS is to restore drainage and aeration by enlarging the sinus passageways. Unfortunately, FESS may fail in a significant portion of patients and is manifested by persistent symptoms, recurrent infections, or the need for revision surgery.19 Therefore, the goals of continued medical therapy after FESS are to decrease inflammation, eradicate the infection, reduce morbidity, and prevent complications.20 Medications in the management of CRS patients after FESS include antibiotics, oral steroids, and nasal steroids; each of these classes of medications and a steroid-eluting implant for targeted delivery of steroids directly to the sinus mucosa, is discussed in greater detail below. OPTIONS FOR DRUG DELIVERY TO THE SINUSES Overview Due to the lack of a standardized approach to postoperative care following successful FESS and the various reported strategies, a debate regarding the components of an optimal postoperative care protocol remains. In addition to nasal saline irrigations and inoffice endoscopic nasal and sinus cavity debridement, the drug delivery modalities most commonly described in postoperative care protocols include the use of : • Systemic antibiotic therapy; • Systemic corticosteroid therapy; • Topical corticosteroid therapies; • Middle meatal spacers infused with drug;21 and • Drug-eluting stents. Each of these is described in greater detail below. Antibiotics After FESS, antibiotics are used to facilitate healing by preventing infection.22 Antibiotic therapy is frequently started in the operating room based on preoperative culture or to provide coverage for the more commonly found organisms.23 Because there is evidence 12 that the underlying bone may become involved in the inflammatory process, long-term broad-spectrum antibiotic coverage after FESS is often necessary in cases of severe, chronic, inflammatory disease. The antibiotics generally prescribed are amoxicillin and potassium clavulanate, cephalosporin, or a quinolone. While antibiotics are used routinely in the postoperative care of FESS patients, their efficacy has not been well evaluated. Jiang, et al conducted a study of 71 patients with CRS who had undergone FESS and were randomly divided into two groups: a study group (31 patients), who took amoxicillin/clavulanate for 3 weeks after FESS and the control group (40 patients), for whom no antibiotic was given postoperatively.24 Preoperatively, all of the patients completed a symptom questionnaire and received nasal endoscopy; swab specimens were taken from the middle meati for bacterial cultures. These procedures were performed again 3 weeks after surgery. The results showed that the symptom scores significantly decreased after surgery in both groups of patients; however, the bacteria identified before and after FESS were statistically different in both groups. There were no differences in the symptom and endoscopic scores, rates of bacterial culture, and drug sensitivity to amoxicillin/clavulanate between the two groups after FESS. The authors concluded that the results of this study demonstrated that postoperative care with amoxicillin/clavulanate did not improve the short-term outcome of FESS on CRS or reduce bacterial growth 3 weeks after FESS. Patients with recurring episodes of CRS after FESS often require multiple courses of antibiotic therapy for extended durations.25 This, combined with the fact that these patients have usually been treated with multiple different antibiotics prior to surgery, makes them especially vulnerable to the development of antibiotic resistance. Therefore, the issue of increasing antibiotic resistance in sinusitis dictates that antibiotics should be used with caution.26 Topical antibiotic therapy is another management strategy for patients with CRS.27Topical therapies would seem to provide a greater concentration of medication to the nasal cavities, while at the same time lowering toxicity in comparison to systemic antibiotics. Previous studies have demonstrated nebulization of topical therapies to be clinically effective in patients with uncontrollable CRS. Vaughn and Carvalho studied 42 patients with acute exacerbation of CRS, refractory to previous FESS, who received nebulized antibiotics or standard antibiotic therapy.28 Symptomatic and endoscopic data before and after the nebulized therapy demonstrated a longer infection-free period (an average of 17 weeks) compared with standard therapy (an average of 6 weeks). Statistically significant improvements were noted for symptom scores of posterior nasal drainage, thick nasal debris, facial pressure and pain. Furthermore, the therapy resulted in clearing of the initial bacteria in 76% of the 50 treatment sessions. Uren, et al examined the efficacy and tolerability of topical mupirocin for the management of surgically recalcitrant CRS associated with Staphylococcus aureus infection in 16 patients.29 The patients were treated with twice daily nasal lavages containing 0.05% mupirocin and lactated ringers salts for a 3 week period. Patients were assessed before and after treatment in terms of nasoendoscopic findings, microbiology results, 13 and Sinonasal Outcome Test (SNOT) and visual analogue scale questionnaires. The results demonstrated that 15 of the 16 patients had improved nasoendoscopic findings after treatment; 12 of the 16 patients noted overall symptom improvement; and 15 of 16 patients had negative swab results for Staphylococcus aureus after treatment. The authors concluded that nasal lavage with 0.05% mupirocin may represent an effective and well tolerated alternative treatment for postoperative, refractory CRS. However, not all published reports support the use of topical antibiotics.30 Desrosiers and Salas-Prato studied the efficacy of nebulized topical saline-tobramycin solution in 20 patients with CRS for whom FESS had failed to relieve their symptoms.31 The patients were randomized into two groups and received either a tobramycin-saline solution or a saline-only solution administered three times a day to the nasal passages via a largeparticle nebulizer for 4 weeks, followed by a 4-week observation period. The outcome measures assessed were symptoms, quality of life, and endoscopic appearance of the sinus mucosa. The results of this study demonstrated that both treatments were well tolerated and produced equivalent improvements in symptoms, quality of life, and mucosal aspect. Treatment with a tobramycin-saline solution gave patients a more rapid improvement of pain, but led to the development of nasal congestion; therefore the addition of tobramycin appears to be of minimal benefit. Regardless of the mode of delivery or of the specific antibiotic given, if there is evidence of infection in the cavity post-operatively, the cavity should be recultured under endoscopic visualization and the antibiotic changed accordingly. Corticosteroids Synthetic corticosteroids are man-made drugs that closely resemble cortisol (a steroid hormone, or glucocorticoid, that the body produces naturally) and are used in medicine to treat diseases that are caused by an overactive immune system or inflammation. They bind to glucocorticoid receptors, activating anti-inflammatory proteins that reduce immune activity and inflammation.32 As previously discussed, oral and nasal steroids are used after FESS to control inflammation caused by surgery in an effort to maintain the patency of the open sinus cavity. When delivered topically after FESS, steroids may lead to improved wound healing by preventing granulation tissue that can lead to adhesions. Oral Steroids Steroids are the most commonly used medication in FESS protocols.33 While there have been no randomized controlled trials specifically assessing the efficacy of postoperative systemic steroid use for nasal polyposis, the consensus is that a short course of high dose prednisone is helpful for many patients. 34 A randomized, placebo-controlled trial was conducted by Rupa, et al to determine the effectiveness of postoperative oral steroids in controlling disease in 24 patients with allergic fungal sinusitis (AFS) who underwent endoscopic sinus surgery (with or without open surgery).35The results of this study found that a 12-week course of postoperative oral prednisone in a tapering dose produced significant subjective and objective improvements in these AFS patients; in addition, it is effective in preventing early recurrence. 14 It must be noted that the use of oral steroids carries multiple systemic risks, which restricts their prolonged use 36; these risks include aseptic necrosis of the femoral head, calcium demineralization, posterior cataract formation, mood changes, and increases in blood glucose levels.37 As a result, their use is limited in patients with diabetes, glaucoma and certain psychological disorders.38 Oral steroid treatment algorithms vary depending on disease state, degree of polyposis and other comorbidities. Nasal Steroids After FESS, patients are often prescribed and instructed to use nasal steroids to minimize postoperative edema. To minimize the potential of recurrence, patients are often instructed to continue their use long term.39 Nasal steroids can be administered in the form of sprays or solutions.40 Studies have shown that intranasal deposition is only 30% since 70% of the drug is washed away via mucociliary clearance.41 In addition, their benefits can be further diminished by postoperative edema, discharge, crusting, or poor adherence to the treatment regimen.42 A study of 60 CRS patients conducted by Nabi et al, evaluated patient adherence to nasal spray regimens following FESS and also studied various factors that predict adherence.43 In this randomized, blinded, controlled trial, the patients were managed with FESS and started on one of three postoperative nasal spray regimens. Structured telephone interviews were conducted after surgery over a 12-month period using a validated questionnaire that assessed both spray adherence and barriers to adherence. The results demonstrated that over half (57.4%) of the patients were nonadherent to postoperative nasal sprays, regardless of which nasal spray regimen they were on. Preoperative SNOT scores, time after FESS, and the presence of a patient adherence risk factor predicted compliance. Through knowledge of these results and the clinical implications of this study, otolaryngologists can selectively use strategies that improve adherence in high-risk patients and potentially improve surgical outcomes in CRS patients. In comparison with oral steroid administration, topical steroids are more widely used as a treatment after FESS because they can be given for longer periods of time without the associated systemic side effects.44 However, simply applying topical steroids through the nostrils does not imply delivery of the drug into the sinus; in order to effectively deliver topical agents into the sinuses, appropriate access and delivery methods are required.45 Middle Meatal Spacers Infused with Drug After FESS, early topical therapy may be limited due to retained secretions, nasal crusting, or mucosal edema. For this reason, surgeons have attempted the addition of drug to middle meatal spacers in order to deliver drug directly to the sinus in the early postoperative period and attempt to control inflammation. Because these drug-infused spacers are produced by the treating surgeon, who determines the type and dosage of steroid, the major disadvantages of this therapy are unknown drug release and limited data on systemic absorption. Therefore, the ideal dose and safety profile must be evaluated before these devices can be recommended for routine use.46 Additionally, these spacers are considered off-label as they have not been cleared by FDA. The following three studies have assessed the role of drug-infused middle meatal spacers after FESS: 15 • Cote and Wright47 (level 1b) and Kang, et al48 (level 2b) evaluated postoperative ethmoid cavity packing soaked with topical triamcinolone in CRS patients with nasal polyps. These studies demonstrated significant improvements in the endoscopic appearance in both the early and late postoperative periods, as well as a decreased recurrence of polyps. The specific protocol used in the study conducted by Cote and Wright included a triamcinolone-soaked spacer placed within the ethmoid cavity upon completion of FESS and then removed week 1 at the time of debridement. • A recent level 1b study conducted by Rudmik, et al used an off-label mixture of carboxymethylcellulose foam and dexamethasone (4 ml of 4mg/ml) in patients without nasal polyposis, who underwent FESS for medically refractory CRS.49 While the results did not demonstrate any advantages of the steroid eluting spacer in comparison to a placebo, the outcomes must be considered in context of the authors postoperative care protocol, which utilized a short dose of systemic steroids Bioabsorbable steroid-eluting sinus stent and large volume saline irrigations. Steroid-Eluting Implants A relatively new technology after FESS is a dissolvable, steroid-eluting implant, which is designed to maintain sinus patency postoperatively. The spring-like device expands to prop open the ethmoid sinuses while locally eluting 370 μg of a glucocorticosteroid (mometasone furoate) during the 30-day postoperative period to reduce inflammation as well as the need for systemic anti-inflammatory medication (see Figure 10).50 Figure 10 10 –– Perioperative Course: FESS and Placement of Steroid-Eluting Implant Implant Figure Perioperative Course: FESS and Placement of Steroid-Eluting Pre-Surgery Pre-Surgery Surgery Complete Implant Placed Ethmoid Cavity 30 dayEthmoid Post-opCavity 30 FIGURE 2. Endoscopic photographs from a study patient. (A) Control stent placed in right postoperative ethmoid sinus cavity and (B) d Surgery Complete Implant Placed day Post-op placed in left side. (C, D) Same sinuses at day 30 (stents are no longer present). Middle turbinates remain in medial position bilaterally. change is noted in ethmoid sinus on control stent side (black arrow). Drug eluting stent side (D) is normal. (A) Control stent on right at day 0 Polyps fill ethmoid cavitystenton leftPotential forControl blockage, inflammation at day 0. (C) side at day 30. (D)Reduces Drug-eluting side at day 30. inflammation • Polyps fill ethmoid medialization • Potential for blockage, • Reduces inflammation procedures were permitted. Patients were exdisallowed in order to avoid confounding the (Catheter shown is the Maintains patency cavity cluded ifinflammation they had known history of intolerance to corticosThe use of nasal tampons adjacent to the infe device delivery system teroids, an steroid–dependent condition, a history of was permitted in some patients across all stu priororal to deployment of immune(Catheter deficiency,shown insulin-dependent diabetes, or allergic is the • Maintains patency upon the judgment of the clinician. implant.) fungal sinusitis. Follow-up assessments occurred at postpr device delivery system Oral steroidswere not permitted during a 14-day run-in 7, 14, 21, 30, 45, and 60. During follow- prior to to deployment ofIntravenous 51 period prior sinus surgery. decadron wasa common doscopic examination of administration. the surgical cavity, Prior to the development of steroid-eluting implants, oral steroids were route of steroid implant.) given prior to beginning the surgical procedure on the clots and crusts, and lysis of adhesions was eluting implants may have significant benefit in the treatment of CRS; recently, Level 1-A evidence demonstrates th day of surgery. Patients received between 4 and 20 mg these activities, lysis of adhesions was record 54 may significantly improve endoscopic medically refractory with The andextent without nasal polyposis. of decadron basedoutcomes upon their for weight. Two patients did CRSpoint. of debridement was left to Prior to the development of steroid-eluting implants, oral steroids common not receive intravenous (IV) decadron. Intranasal steroid were of theaclinician caringroute for the patient. Oral a sprays 51 were permitted up to the day before surgery. A 14tranasalbenefit steroid sprays were disallowed dur ofThe steroid administration. Steroid-eluting implants may have significant in the implant is self-expanding and conforms to the variable sinus anatomy without obstructing the cavity. The impla day course of oral antibiotics consisting of amoxicillin with follow-up period. At day 30, clinicians were treatment CRS;the recently, evidence demonstrates that they significantly expands toofcontact mucosalLevel tissue, which is important forhours effectively delivering mometasone corticos clavulonic acid at a1-A dose of 875 mg every 12 begintion tomay prescribe steroidsfuroate, if deemeda necessary 53 ning 1inday preoperatively required. Clindamycin or sprays or irrigation was permitted as neede over 30 days, and remains tissue outmedically to 60 was days, combating inflammation. improve endoscopic outcomes for refractory CRS with and without nasal levofloxacin was used if penicillin allergy was present. surgery and during follow-up. The use of th At the end of the FESS procedure, the patient’s postoperor irrigation in the study varied per physician polyposis.54 Mometasone furoate (MF) was selected as the anti-inflammatory agent among numerous evaluated compounds b ative sinus cavities were randomly assigned by envelope method to absorbability, receive either the corticosteroid-eluting three important characteristics: binding affinity and lowsinus systemic bioavailability. The compound prefe Efficacy assessments stent or an identical non-eluting control stent. Randomizaabsorbs into the sinustion lining The drug has the highest glucocorticoid rece wasinstead stratifiedofbythe sitesurrounding and followedmucous a blockedfluid. scheme The device performance and efficacy endpo 16 binding affinity, makingthat it highly in preventing inflammation tissue. are p was notpotent made known to study centers. Subjects, once physi- within sessed by Glucocorticoid direct endoscopicreceptors examination The implant is self-expanding and conforms to the variable sinus anatomy without obstructing the cavity. The implant expands to contact the mucosal tissue, which is important for effectively delivering mometasone furoate, a corticosteroid, over 30 days, and remains in tissue out to 60 days, combating inflammation.53 Mometasone furoate (MF) was selected as the anti-inflammatory agent among numerous evaluated compounds based on three important characteristics: absorbability, binding affinity and low systemic bioavailability. The compound preferentially absorbs into the sinus lining instead of the surrounding mucous fluid. The drug has the highest glucocorticoid receptor binding affinity, making it highly potent in preventing inflammation once within tissue. Glucocorticoid receptors are the molecules in the surface membranes of cells throughout the body to which corticosteroids chemically bind. Additionally, the compound has low systemic bioavailability, meaning that it has negligible systemic safety side effects. The steroid is embedded in a bioabsorbable polymer matrix, which controls the release over time; the steroid is delivered in a sustained fashion directly to the sinus mucosa. The implant dissolves over 30 to 45 days,54 therefore, no removal is required. The polylactideco-glycolide polymer is the same class of material as dissolvable sutures, but without additives, colorants or lubricants. It has been proven to be safe and biologically inert in pre-clinical histologic analysis, ie, no foreign body reaction with either steroid-coated implants or nondrug-coated implants.55 The implant is contraindicated for patients with suspected intolerance to mometasone furoate or have known hypersensitivity to lactide, glycolide or caprolactone copolymers. The steroid-eluting implant has been clinically proven to optimize postoperative patient outcomes, and as noted above, is supported by Level 1-A evidence. These clinical study results demonstrated that the implant is able to mechanically prop the post-surgical ethmoid cavity open and medically control drug delivery of mometasone furoate, thus reducing the development of granulation tissue, which is a precursor for scarring.56 Sustained delivery of mometasone furoate reduces inflammation, thereby preventing obstruction due to adhesions and edema. Adverse effects, including infection, crusting, headaches, discomfort, and granulation tissue formation, have been reported;57,58 in addition, since the implant gradually dissolves, patients may also notice thin white fragments migrating from the nose.59 Wei and Kennedy reviewed the mode of action and the evidence supporting the efficacy of this steroid eluting implant.60 They noted that three recently published clinical trials demonstrate that a mometasone furoate-eluting implant produced statistically significant reductions in inflammation, polyp formation, and postoperative adhesions. Additionally, the implant has been found to significantly decrease the need for postoperative administration of oral steroids and to also reduce the frequency of postoperative lysis of adhesions.61 Although the placement of steroid-impregnated packing, sponges, and gels has previously been utilized in the postoperative sinus cavities, a mometasone furoateeluting implant introduces a new mechanism for sustained, localized and controlled delivery of topical therapy directly to the nasal mucosa for CRS. 17 SUMMARY Chronic rhinosinusitis is a widespread, debilitating disease that can significantly affect a person’s quality of life. The care pathway for patients with CRS involves a complex combination of medical and surgical therapies. While techniques in FESS have undergone major developments over the last 25 years, this procedure is now a well-established treatment option for patients with sinus disease. However, despite these advances, both surgeons and patients are currently frustrated with the disease recurrence that takes place so soon after surgery due to inflammation, polyp recurrence, adhesions, and middle turbinate lateralization. Therefore, numerous perioperative techniques and continued medical therapy aimed at optimizing surgical outcomes are generally used to maintain the benefits of FESS. The goals of continued medical therapy after FESS are to decrease inflammation, eradicate the infection, reduce morbidity, and prevent complications. Medications used in the management of CRS patients after FESS include antibiotics, oral steroids, nasal steroids, and steroid-eluting implants. 18 GLOSSARY Antibiotics A chemical substance produced by a microorganism which has the capacity, in diluted solutions, to inhibit the growth of or to kill other microorganisms. Chronic Rhinosinusitis (CRS) A term used to describe various entities characterized by chronic symptoms of nasal and sinus inflammation or infection; this condition interferes with drainage and causes mucus to build-up. Corticosteroid A man-made drug that closely resembles cortisol (a hormone that the body produces naturally) and is used in medicine to treat diseases that are caused by an overactive immune system or inflammation. Ethmoid Sinuses One of the four paired paranasal sinuses. Functional Endoscopic Sinus A minimally invasive surgical procedure performed to enlarge the sinus Surgery (FESS) passageways to restore drainage and aeration. Nasal Steroids A corticosteroid spray treatment. The medicine in the spray is placed directly in the nose to help reduce symptoms and make breathing through the nose easier. Oral Steroids An anabolic steroidal hormone that has been manufactured in a manner that allows it to be administered in an oral fashion. Paranasal Sinuses Any of the group of four paired air-filled spaces in the bones of the face that surround the nasal cavity; they are lined with mucous membrane, which is continuous with the lining of the nasal cavities. Steroid-Eluting Implant A medical device implanted in the ethmoid sinuses to prop open the sinus cavity while providing controlled drug delivery directly to the sinus tissue. 19 REFERENCES 1. Pleis JR, Lethbridge-Cejku M. Summary health statistics for U.S. adults: National Health Interview Survey, 2006. Vital Health Stat. 2007;10(235): 1-153. http://www.cdc. gov/nchs/data/series/sr_10/sr10_235.pdf. Accessed December 1, 2014. 2. Forwith KD, Chandra RK, Yun PT, Miller SK, Jampel HD. ADVANCE: a multisite trial of bioabsorbable steroid-eluting sinus implants. Laryngoscope. 2011;121(11):2473-2480. 3. Singh A. Paranasal sinus anatomy. http://emedicine.medscape.com/article/1899145overview. Accessed December 1, 2014. 4. Lethbridge-Çejku M, Rose D, Vickerie J. Summary health statistics for U.S. adults: National Health Interview Survey, 2004. Vital Health Stat. 2006; 10(228):19-22. http:// www.cdc.gov/nchs/data/series/sr_10/sr10_229.pdf. Accessed December 1, 2014. 5. Gliklich RE, Metson R. The health impact of chronic sinusitis in patients seeking otolaryngologic care. Otolaryngol Head Neck Surg. 1995; 113 (1):104-109. 6. Jakobsen J, Svendstrup F. Functional endoscopic sinus surgery in chronic sinusitis-a series of 237 consecutively operated patients. Acta Otolaryngol Suppl. 2000; 543:158161. 7. Schaitkin B, May M, Shapiro A, Fucci M, Mester SJ. Endoscopic sinus surgery: 4-year follow-up on the first 100 patients. Laryngoscope. 1993;103(10):1117-1120. 8. Proctor DF. The nose, paranasal sinuses, and pharynx. In: Lewis-Walters Practice of Surgery, Vol. 4. Hagerstown, MD: WF Prior Co.;1966:1-37. 9. Musy PY, Kountakis SE. Anatomic findings in patients undergoing revision endoscopic sinus surgery. Am J Otolaryngol. 2004;25(6):418-422. 10. Wormald PJ, Boustred RN, Le T, Hawke L, Sacks R. A prospective single-blind randomized controlled study of use of hyaluronic acid nasal packs in patients after endoscopic sinus surgery. Am J Rhinol. 2006;20(1):7-10. 11. Ramadan HH. Surgical causes of failure in endoscopic sinus surgery. Laryngoscope. 1999; 109(1): 27-29. 12. Wynn R, Har-El G. Recurrence rates after endoscopic sinus surgery for massive sinus polyposis. Laryngoscope. 2004; 114 (5): 811-813. 13. Kennedy DW, Wright ED, Goldberg AN. Objective and subjective outcomes in surgery for chronic sinusitis. Laryngoscope. 2000;110 (3 Pt 3):29-31. 14. Soler ZM, Smith TL. Quality-of-life outcomes after endoscopic sinus surgery: how long is long enough? Otolaryngol Head Neck Surg. 2010;143(5):621-625. 15. Wei CC, Kennedy DW. Mometasone implant for chronic rhinosinusitis. Med Devices (Auckl). 2012;5:75-80. 16. American Rhinologic Society. ARS position statement on biomaterials. https://www. american-rhinologic.org/position_biomaterials. Accessed December 1, 2014. 20 17. Kim RJT, Douglas RG. Perioperative care for functional endoscopic sinus surgery. The Otorhinolaryngologist. 2012; 5(1): 27-30. http://www.greenlaneresearch.co.nz/ Portals/1/Docs/The%20Otorhinolaryngologist%202012%20Kim.pdf. Accessed December 1, 2014. 18. Stjarne P, Olsson P, Alenius M. Use of mometasone furoate to prevent polyp relapse after endoscopic sinus surgery. Arch Otolaryngol Head Neck Surg. 2009;135(3):296302. 19. Bhattacharyya N, Kepnes LJ. The microbiology of recurrent rhinosinusitis after endoscopic sinus surgery. Arch Otolaryngol Head Neck Surg. 1999;125(10):11171120. http://archotol.jamanetwork.com/article.aspx?articleid=509871. Accessed December 1, 2014. 20. Brook I, Hinthorn DR. Chronic sinusitis medication. http://emedicine.medscape.com/ article/232791-medication#8. Accessed December 1, 2014. 21. Rudmik L, Smith TL. Evidence-based practice: postoperative care in endoscopic sinus surgery. Otolaryngol Clin North Am. 2012;45(5):1019-1032. 22. Tysome J, Sharp H. Current trends in pre and postoperative management of functional endoscopic sinus surgery. The Internet Journal of Otorhinolaryngology. 2005; 5(2). https://ispub.com/IJORL/5/2/12413. Accessed December 1, 2014. 23. Kennedy DW. Functional endoscopic sinus surgery: anesthesia, technique, and postoperative management. In: Kennedy DW, Bolger WE, Zinreich SJ, eds. Diseases of the Sinuses: Diagnosis and Management. Ontario, Canada: B.C. Decker Inc.; 2001: 211-221. 24. Jiang RS, Liang KL, Yang KY, et al. Postoperative antibiotic care after functional endoscopic sinus surgery. Am J Rhinol. 2008;22(6):608-612. 25. Bhattacharyya N, Kepnes LJ. The microbiology of recurrent rhinosinusitis after endoscopic sinus surgery. http://archotol.jamanetwork.com/article. aspx?articleid=509871. Accessed December 1, 2014. 26. Tysome J, Sharp H. Current trends in pre and postoperative management of functional endoscopic sinus surgery. The Internet Journal of Otorhinolaryngology. 2005; 5(2). https://ispub.com/IJORL/5/2/12413. Accessed December 1, 2014. 27. Manes RP, Batra PS. Etiology, diagnosis and management of chronic rhinosinusitis. http://www.medscape.com/viewarticle/777378_4. Accessed December 1, 2014. 28. Vaughan WC, Carvalho G. Use of nebulized antibiotics for acute infections in chronic sinusitis. Otolaryngol Head Neck Surg. 2002;127(6):558-568. 29. Uren B, Psaltis A, Wormald PJ. Nasal lavage with mupirocin for the treatment of surgically recalcitrant chronic rhinosinusitis. Laryngoscope. 2008; 118(9):1677-1680. 30. Manes RP, Batra PS. Etiology, diagnosis and management of chronic rhinosinusitis. http://www.medscape.com/viewarticle/777378_4. Accessed December 1, 2014. 21 31. Desrosiers MY, Salas-Prato M. Treatment of chronic rhinosinusitis refractory to other treatments with topical antibiotic therapy delivered by means of a largeparticle nebulizer: results of a controlled trial. Otolaryngol Head Neck Surg. 2001;125(3):265-269. 32. Lipworth BJ, Jackson CM. Safety of inhaled and intranasal corticosteroids: lessons for the new millennium. Drug Safety. 2000; 23(1):11-33. 33. Tysome J, Sharp H. Current trends in pre and postoperative management of functional endoscopic sinus surgery. The Internet Journal of Otorhinolaryngology. 2005; 5(2). https://ispub.com/IJORL/5/2/12413. Accessed December 1, 2014. 34. Kim RJT, Douglas RG. Perioperative care for functional endoscopic sinus surgery. The Otorhinolaryngologist. 2012; 5(1): 27-30. http://www.greenlaneresearch.co.nz/ Portals/1/Docs/The%20Otorhinolaryngologist%202012%20Kim.pdf. Accessed December 1, 2014. 35. Rupa V, Jacob M, Mathews MS, Seshadri MS. A prospective, randomised, placebocontrolled trial of postoperative oral steroid in allergic fungal sinusitis. Eur Arch Otorhinolaryngol. 2010;267(2):233-238. 36. Wei CC, Kennedy DW. Mometasone implant for chronic rhinosinusitis. Med Devices (Auckl). 2012;5:75-80. 37. Schacke H, Döcke W, Asadullah K. Mechanisms involved in the side effects of glucocorticoids. Pharmacol Ther. 2002;96(1):23-43. 38. Campbell RG, Kennedy DW. What is new and promising with drug-eluting stents in sinus surgery? Curr Opin Otolaryngol Head Neck Surg. 2014;22(1):2-7. 39. Kennedy DW. Functional endoscopic sinus surgery: anesthesia, technique, and postoperative management. In: Kennedy DW, Bolger WE, Zinreich SJ, eds. Diseases of the Sinuses: Diagnosis and Management. Ontario, Canada: B.C. Decker Inc.; 2001: 211-221. 40. Brook I, Hinthorn DR. Chronic sinusitis medication. http://emedicine.medscape.com/ article/232791-medication#9. Accessed December 1, 2014. 41. Lipworth BJ, Jackson CM. Safety of inhaled and intranasal corticosteroids: lessons for the new millennium. Drug Safety. 2000; 23(1):11-33. 42. Joe SA, Thambi R, Huang J. A systematic review of the use of intranasal steroids in the treatment of chronic rhinosinusitis. Otolaryngol Head Neck Surg. 2008;139(3):340-347. 43. Nabi S, Rotenberg BW, Vukin I, Payton K, Bureau Y. Nasal spray adherence after sinus surgery: problems and predictors. J Otolaryngol Head Neck Surg. 2012;41 Suppl 1:S49-55. 22 44. Snidvongs K, Kalish L, Sacks R, Sivasubramaniam R, Cope D, Harvey RJ. Sinus surgery and delivery method influence the effectiveness of topical corticosteroids for chronic rhinosinusitis: systematic review and meta-analysis. Am J Rhinol Allergy. 2013;27(3):221-233. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3901441/. Accessed December 1, 2014. 45. Snidvongs K, Kalish L, Sacks R, Sivasubramaniam R, Cope D, Harvey RJ. Sinus surgery and delivery method influence the effectiveness of topical corticosteroids for chronic rhinosinusitis: systematic review and meta-analysis. Am J Rhinol Allergy. 2013;27(3):221-233. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3901441/. Accessed December 1, 2014. 46. Rudmik L, Smith TL. Evidence-based practice: postoperative care in endoscopic sinus surgery. Otolaryngol Clin North Am. 2012;45(5):1019-1032. 47. Côté DW, Wright ED. Triamcinolone-impregnated nasal dressing following endoscopic sinus surgery: a randomized, double-blind, placebo-controlled study. Laryngoscope. 2010;120(6):1269–1273. 48. Kang IG, Yoon BK, Jung JH, Cha HE, Kim ST. The effect of high-dose topical corticosteroid therapy on prevention of recurrent nasal polyps after revision endoscopic sinus surgery. Am J Rhinol. 2008;22(5):497–501. 49. Rudmik L, Mace J, Mechor B. Effect of a dexamethasone Sinu-Foam™ middle meatal spacer on endoscopic sinus surgery outcomes: A randomized, double-blind, placebo-controlled trial. Int Forum Allergy Rhinol. 2012;2(3):248–251. 50. Wei CC, Kennedy DW. Mometasone implant for chronic rhinosinusitis. Med Devices (Auckl). 2012;5:75-80. 51. Jakobsen J, Svendstrup F. Functional endoscopic sinus surgery in chronic sinusitis-a series of 237 consecutively operated patients. Acta Otolaryngol Suppl. 2000; 543:158-161. 52. Rudmik L, Smith TL. Evidence-based practice: postoperative care in endoscopic sinus surgery. Otolaryngol Clin North Am. 2012;45(5):1019-1032. 53. Li PM, Downie D, Hwang PH. Controlled steroid delivery via bioabsorbable stent: safety and performance in a rabbit model. Am J Rhinol Allergy. 2009; 23(6):591-596. 54. Han JK, Marple BF, Smith TL, et al. Effect of steroid-releasing sinus implants on postoperative medical and surgical interventions: an efficacy meta-analysis. Int Forum Allergy Rhinol. 2012;2(4):271-279. 55. Li PM, Downie D, Hwang PH. Controlled steroid delivery via bioabsorbable stent: safety and performance in a rabbit model. Am J Rhinol Allergy. 2009; 23(6):591-596. 23 56. Han JK, Marple BF, Smith TL, et al. Effect of steroid-releasing sinus implants on postoperative medical and surgical interventions: an efficacy meta-analysis. Int Forum Allergy Rhinol. 2012;2(4):271-279. 57. Wei CC, Kennedy DW. Mometasone implant for chronic rhinosinusitis. Med Devices (Auckl). 2012;5:75-80. 58. Forwith KD, Chandra RK, Yun PT, Miller SK, Jampel HD. ADVANCE: a multisite trial of bioabsorbable steroid-eluting sinus implants. Laryngoscope. 2011;121(11):24732480. 59. Intersect ENT Inc. About PROPEL® mometasone furoate implant. http://www. metroent.com/webdocuments/brochure-PROPEL-patient-information.PDF. Accessed December 2, 2014. 60. Wei CC, Kennedy DW. Mometasone implant for chronic rhinosinusitis. Med Devices (Auckl). 2012;5:75-80. 61. Wei CC, Kennedy DW. Mometasone implant for chronic rhinosinusitis. Med Devices (Auckl). 2012;5:75-80. 24 Please click here for the Post-Test and Evaluation 25