Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Mol. Cells. Vol. 3. pp. 251-254
Analysis of lrmyc Restriction Fragment Length Polymorphism
in Stomach Cancer by Polymerase Chain Reaction
Hee Won Lee, Dong Wook Kim t , Jae Dam Lee, Kyoo Hyung Lee l, Jung Sin Lee l,
Sang-Hee Kiml , In Chul Lee 2, Kun Chun Park\ Sachio Nomura4 , Kazuko Kawashima4 ,
Susumu Nishimura 4 and Doe Sun Na*
Department of Biochemistry, IDepartment of Oncology, 2Department of Pathology and 3Department
of Surgery, College of Medicine, University of Ulsan, Seoul 138-040, Korea; 4Biology Division,
National Cancer Center Research Institute, Tokyo, Japan
(Received on June 14, 1993)
A Polymerase Chain Reaction (PCR) method has been developed for analysis of L-myc EcoRI
RFLP (restriction fragment length polymorphism) which originates from the polymorphic EcoRI
site in the second intron of the L-myc gene. The patterns of L-myc gene polymorphism were
examined using DNAs isolated from cancer tissues and normal tissues of sixty seven patients
with stomach cancer. The patients were classified into three genotypes (L-L, L-S, S-S) according to the polymorphic patterns defined by two alleles (L, S). Cancer tissues and normal
tissues of the same patients showed the same patterns in the RFLP. Analysis of L-myc RFLP
with the clinical pattern of the malignancy showed no significant correlation with metastasis
and TNM staging. However, in contrast to other reports, a correlation was found between
the RFLP pattern and the size of the tumor (p = 0.005). The preponderance of the L fragment
was observed in the larger (>55 mm) sized tumors.
.
Th e L-myc gene was initially identified as a gene
with sequence homology to c-myc and N-myc from
a human small cell lung carcinoma cell line (Nau
et al., 1985), characterized and sequenced (Kaye et al.,
1988). All three genes have a similar three-exon structure, and encode nuclear phosphoproteins. The L-myc
gene encodes multiple DNA binding proteins translated from alternatively processed mRNAs (DeGreve et
al., 1988).
Restriction fragment length polymorphism (RFLP)
studies of the L-myc gene [ 10 kb(L) and 6 kb(S) Eco RI
fragments] have demonstrated a close association of
the S-aUele with metastatic potential in lung cancer
and breast cancer (Kawashima et al., 1988 and 1992;
Champeme et ar, 1992). Studies by other researchers
also indicated an association of L-myc RFLP to the
clinical parameters in ren al cell carcinoma (Kakehi
and Yoshida, 1989), genitourinary (Kakehi et al., 1991)
and oral cancer (Saranath et al., 1990). These studies
indicate that L-myc RFLP is potentially important for
diagnostic prognosis. In contrast to these results, other
studies did not find any correlation of L-myc RFLP
to the metastasis or other clinical parameters (Ikeda
et al., 1988; Tefre et al., 1990). For evaluation of usefulness of L-myc RFLP for diagnostic prognosis, a large
number of samples need to be a nalyzed. Analysis of
L-myc RFLP by Southern blot hybridization is laborious and inconvenient for analyzing a large number
of samples.
* To whom correspondence should be addressed.
We have developed a PCR-based method for analysis of L-myc RFLP and an alyzed a group of stomach
cancer patients for L-myc RFLP in order to investigate
the prognostic utility of L-myc polymorphism and the
correlation between L-myc RFLP and the clinical patterns.
Materials and Methods
Subjects
Sixty-seven untreated patients, diagnosed as having
squamous cell carcinoma of the stomach, were studied
for L-myc polymorphism. The diagnosis was based
on clinical examination and histological features of
the biopsy material. Cancer tissues and normal tissues
near the cancer tissues were obtained at the time of
surgery at Asan Medical Center. D ata such as age,
sex and type of pathological diagnosis are included
in Table 1. The patients included 51 men and 16
women, 31 -78 years of age.
Tumor size, tumor grade and disease extent were
evaluated pathologically. All cases were TNM classified according to the Manual for Staging of Cancer
by AJCC (Beahrs et al., 1988) by a trained clinician.
The sa mples were collected before any chemotherapeutic or radiation therapy treatment had been started.
The abbreviations used are: RFLP, Restriction fragment
length polymorphism; PCR, Polymerase Chain Reaetion.
t Present address: Biochemistry Laboratory, Genetic Engineering Research Institute, Daejon 305-333, Korea.
© 1993 The Korean Society of Molecular Biology
Mol. Cells
L-myc Ge ne RFLP in Stomach Cancer
252
Table I. Distribution of L-myc RFLP pattern and allele frequencies of the L-myc ge ne in tumor tissues and normal
tissues of stomach cancer patients
A
EcoRI
EcoRl
RFLP pattem
S-S
S-L
L-L
Allele freq uencies
S
L
tumor tissues (%)
Normal tissues of
cancer patient (%)
17 (25.4)
31 (46.3)
19 (28.4)
17 (25.4)
31 (46.3)
19 (28.4)
0.49
0.5 1
0.49
0.51
B
I
~/:~
389
319
B
EcoRl
I
I
~
.-
-+
GAC AlT TCC lTG Ter GGA TAG AGT AAG ACA erA ere TCT GAA AGG
(~ I
GAG AAT GGT GI'G err A A A lTA TIT C IT Tel' TAG ATA GAA Ter TCC
I ~O
The RFLP pattern and allele freque ncies of the L-myc gene
in tumor tissues and the normal tissues of the cancer patients were identical to the correspond ing tumor tissues.
TGA Gee AC'G AGG C IT MC Ac r GAA AAT 'I'M AGG llT GGG ATG TAG
IRIJ
GA A AGC erG erG MT CAT TIT erA ACC TAC ccr lTA ACC l 'GA AC'C
TGT TTG l 'GA Gcr TLT AG"T TCA erc ACA GGC CAe A'I'G Gee TC.G AAC
2..l0
CAG An GGA M C AAT GAG GC'G GGG GGT GGG GAA NIT
AAA ATG CM
.1lt)
All sa mples were stored at -70
DNA.
c
U
GAT lUG CAG CAG AGC TCA CCC MT AGG GGe TAG GGG erG GGT AAG
until isolation of
3(<)
ACA GAA lTC C,\A ACA CAG CGr MT CAG C'CA ATC A1 G GGC TIT GGG
GeC AGG AGG Ger GAA TC.G TCA ("NT TTA IT
4
Analysis of L-myc RFLP by peR
Chromosomal DNA sa mples were prepared with
a method modified from the convention al DNA pUlificatio n procedures. Briefly, 2 mg of the tissue was
incubated in the 400 J.11 PC R buffer (50 mM KCI,
10 mM Tris/ HC I, pH 8.3, 2.5 mM MgCh, 0.1 mglml
gelatin, 0.45% NP40, 0.45% Tween20) with 12.5 f1l proteinase K (20 mglml) at 55 t for 16-20 h. This solu tio n was directly used for PCR after inactivation of
th e proteinase K by incubation at 95 t
for IS
mll1 .
In designing th e primers for PC R, we utilized the
nucleotide seq uence of the polymorphic L-myc genes
around the polymorphic £Co Rl site which was determined in our laboratory. The strategy for L-myc RFLP
ana lysis by PC R and the nucleotide sequence of the
primers a nd the amplified region for both L- and Sall ele are shown in Figure I. Oligonucleotides for primers were synthesized with an automatic DNA syn thesizer, deprotected and gel purified. PC R reaction
was carried out in the sta ndard PC R buffer (10 mM
Tris/ HC l, pH 8.3, 1.5 mM MgCh, 50 mM KCl, 0.1%
gelatin, 0.45% NP40, 0.45% Tween20) with 30 cycles
of 93 °c, I min, 55 °c, I min, 72 t, I min. The
amplified fragment was digested with EcoRl and ana lyzed on a 1.5% agarose gel.
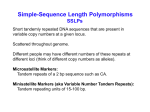
Figure I. A: Strategy for L-myc RFLP analysis by PCR-based
method. The rectangular boxes represent three exons of Lmyc ge ne. The numbers represent the sizes of the resulting
fragments after PCR amplification a nd EcoRl d igestion. B:
Nucleotide sequences of the a mplified fragment. The sequence is shown as S-allele and the polymorph ic EcoRl site
is underlined. The nucleotide "T" identified with a circle
is a "G" in the L-allele. The sequences of L- and S-allele
were identical except the si ngle base d ifference at the EcoRl
site. The primers are shown as arrows.
M123456M
............ 389 bp
-319 bp
-70bp
Results
Analysis of L-myc gene polymorphism
The strategy for a nalysis of L-myc RFLP by PCR
is illustrated in Figu re IA. The 389 bp region between
two primers is amplified by PC R. Digestion of the
389 bp fragment by EcoRl yields the origi nal 389 bp
fragment for L-alle\e, a nd two fragments of 319 bp
a nd 70 bp for S-alle\e. Figure 2 shows the typical results of the RFLP a nalysis by PCR, EcoRl digestion,
followed by agarose gel electrophoresis. The expected
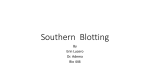
Figure 2. Ana lysis of L-myc RFLP by PCR-based method.
The PCR amplified DNA was separated on a 2% agarose
gel after Eco Rl digestion as described in the text. The patterns of the three representative genotypes (L-L: la ne I, 2;
L-S: lane 3, 4; S-S: lane 5, 6) are shown. Lanes I. 3. 5:
DNA from the cancer tissues and lanes 2, 4, 6: DNA fro m
the normal tissues of the same patients were used for RFLP
analysis.
Vol. 3 (1993)
Hee Won Lee
389 bp band (L) or 319 and 70 bp bands (S) were
observed after EcoRl digestion.
L-myc RFLP patterns in stomach cancers
L-myc RFLP was determined by Eco Rl digestion
of the PCR amplified DNA. The distribution of the
different genotypes among the different ages and sex
groups is shown in Table 1. The three different genotypes are represented in all ages. Nineteen patients
were genetically homozygous for the L-allele (L-L
type), 17 were homozygous for the S-allele (S-S type)
and 31 were heterozygous (L-S type). The frequencies
of the L and S alleles are 0.51 and 0.49 which is
consistent with the H ardy-Weinberg law (Table 2).
The cancer tissue and nonnal tissue DNAs from
the same patient showed th e sa me RFLP pattern in
all 67 cases (Table 2). These results indicate that Lmyc RFLP is genetically fixed and no deletion or
change of either allele occurred in squamous cell
carcinoma of the stomach so far exa mined and are
consistent with the previous obselVation with lung cancers (Kawashima et ai., 1988). The relative ratios of
the L-L, L-S and S-S fragments in the Korean stomach cancer patients were not significantly different
from those obselVed in the nonnal and cancer tissues
el
al.
25 3
of the Japanese patients (Kawashima et al., 1988) or
NOIwegian patients (Tefre et ai., 1990).
Correlation of L-myc RFLP with clinical pattern
The relationships between L-myc RFLP and the clinical parameters such as level of differentiation, nodal
metastasis, size of the primary tumor and TNM staging (Beahrs et ai., 1988), at the time of surgery for
the primary tumor are summarized in Table 1. The
relationship between tumor size and the presence or
absence of the L-allele indicated an association of the
L fragment with larger sized tumors (p = 0.005). The
L fragment was present in 29/32 (91 %) of the larger
(> 5.5 cm) tumors. Whereas for smaller tumors «
5.5 cm), only 21/34 (62%) had the L fragment. On
the other hand, stage, grade, depth invasion, and metastasis to other organs of the tumor were not associated with a specific polymorphic fragment (p > 0.5).
On comparing L-myc RFLP types with nodal metasta sis, the more advanced stage N2 exhibited an increased
proportion (19/22= 86%) of patients with L fragment
compared with stages No and N , (31 /43 = 70%). However, the difference was statistically not significant (p
= 0.156).
Discussion
Table 2. Data on patients
with stomach cancer and L-myc
RFLP patterns
RFLP pattern
Patient number
S-S
S-L
L-L
17
31
19
Age (yr) <56
9
8
10
7
13
3
7
15
16
27
4
16
15
9
6
13
3
6
5
18
2
14
6
11
6
13
14
5
5
14
5
3
7
4
2
4
10
3
7
4
8
28
3
15
4
0
5
8
6
~56
Male
Femele
tumor size (mm) <55
Sex
~55
Stage
II
III
N
T stage
N stage
T,
T2
T)
T"
No
N,
N2
Nx
M stage
Mo
M,
Gradea
I
II
III
N
7
2
3
4
9
I
7
6
3
15
2
2
11
3
12
12
5
°Grade I, well diferentiated; II, moderately differentiated; III,
poorly differentiated; N , undifferentiated.
To facilitate the analysis for L-myc RFLP, we have
developed a PCR-based method. Like all PCR methods, this method is simple, fast, requires only a portion of the specimen compared to Southern blot analysis, and does not require the use.of radioisotope. Of
67 stomach cancers S-S-type, S-L-type, and L-L-type
comprised 17 (25.4%) cases, 31 (46.3%) cases, and 19
(28.4%) cases, respectively. The distribution of three
alleles is consistent with the Hardy-Weinberg law and
is also consistent with the distribution of three genotypes in cancer patients and healthy individuals in
other countries (Kawashima et ai., 1988; Kawashima
et al., 1992; Champeme et at., 1992; Kakehi and Yoshida, 1989; Kakehi et a!., 1991; Saranath et ai., 1990;
Ikeda et ai., 1988; Tefre et ai., 1990), which was analyzed by Southern blot hybridization. This result indirectly supports the notion that the PCR-based method
can replace the Southern blot analysis, even though
we did not directly confinn the relevance of this method compared to Southern blot analysis. Also it is
reasonable to assume that the relative ratios of the
three genotypes in Korean stomach cancer patients
and healthy individuals are identical, even though we
did not analyze the Korean healthy individuals.
Prior studies on the L-myc RFLP which have been
conducted to establish a specific association of L-myc
with increased incidence and/or progression of cancers
showed discrepancies (Kawashima et al., 1988; Kawashima et ai., 1992; Champeme et ai., 1992; Kakehi and
Yoshida, 1989; Kakehi et al., 1991; Saranath et al.,
1990; Ikeda et ai., 1988; Tefre et ai., 1990). Our study
254
L-myc Gene RFLP in Stomach Cancer
was carried out to investigate the status of L-myc
RFLP in Korean stomach cancer patients. No correlation between the S-allele and the metastatic potential
was found in the 67 cases of the stomach cancer.
In contrast to the previous obseIVations in other
types of cancers (Kawashima et al., 1988; Kawashima
et al., 1992; Champeme et al., 1992; Kakehi and Yoshida, 1989; Kakehi et al. , 1991; Saranath et al., 1990;
Ikeda et az', 1988; Tefre et al., 1990), a strong correlation between L-myc L-allele and the la rge tumor size
was found in Korean stomach cancer (p = 0.005).
An increased prevalence of the L-allele in the advanced stages N 2 of the stomach cancers was also noticed. However, the number of S-S type patients in stage
N2 was small (3 patients), and hence a statistically
significant difference could not be seen on analysis
(p = 0.l56). No correlation with either L or S fragment with any other clinical parameters was found .
Previously, correlation between the presence of the
S-allele of the L-myc RFLP and clinical parameters
such as metastatic potential and larger size tumor was
found (Kawashima et al., 1988; Kawashima et al., 1992;
Champeme et az' , 1992; Kakehi and Yoshida, 1989;
Kakehi et al., 1991; Saranath et al., 1990). In our study
a correlation between L-allele and the larger size of
tumors was found in stomach cancers. Association of
L-allele with any clinical parameters has never been
obseIVed in the lung, kidney, breast, oral, and colorectal cancers. At present, it is very difficult to explain
the contradiction, and elucidation of any role of the
L or S-allele needs further studies.
Acknowledgment
This study was supported by a grant for genetic
engineering from the Ministry of Education (91-120)
of Korea to Doe Sun Na.
Mol. Cells
References
Beahrs, O. H ., Henson, D. E., Hutter, R V. P., a nd
Myers, M. H. (1988) Manual for Staging of Cancer
(Lippincott J. B., ed) 3rd Ed, Philadelphia
Champeme, M . H., Bieche, 1., Latil, A , Hacene. K ,
and Lidereau, R (1992) Inti. J Cancer 50, 6-9
DeGreve, 1., Battey, 1., Fedorko, 1., Birrer, M ., Evan,
G., Kaye, F., Sausville, E., and Minna, J. (1988) Mol.
Cell BioI. 8, 4381-4388
Kakehi, Y , and Yoshida, O. (1989) Int. J Cancer 43,
391-394
Kakehi, Y , Taki, Y , and Yoshida, O. (1991) Ural. Int.
47(suppl 1), 86-89
Kawashima, K , Shikama, H., Imoto, K , Izawa, M.,
Naruke, T , Okabayashi, K , and Nishimura, S.
(1988) ?roc. Natl. Acad. Sci. USA 85, 2353-2356
Kawashima, K , Nomura, S., Hirai, H ., Fukushi, S.,
Ka rube, T , Takeuchi, K , Naruke, T , and Nishimura, S. (1992) Inti. J Cancer. 50, 557-561
Kaye, F., Battey, J., Nau, M ., Brooks, B., Seifter, E.,
DeGreve, 1., Birrer, M., Sausville, E., and Minna,
1. (1988) Mol. Cell BioI. 8, 186-195
Nau, M . M., Brooks, B. J., Battey, 1., Sausville, E., Gazdar, A F., Kirsch, l. R , McBride, O. W., Bertness,
v., Hollis, G. F., and Minna, 1. D. (1985) Nature
318, 69-73
Saranath, D., Panchal, R G ., Nair, R , Mehta, A R ,
Sanghavi, v., and Deo, M. G . (1990) Br. J Cancer
61, 530-533
Ikeda, l., Ishizaka, Y , Ochiai, M. Sakai, R , Itabashi,
M ., Onda, M., and Sugimura, T (1988) Jpn. J Cancer
Res. 79, 674-676
Tefre, T , Brresen, A L., Aamdal, S., and Brgger, A
(1990) Br. J Cancer 61, 809-812