Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
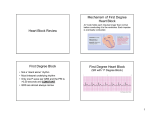
CARDIOVASCULAR PHYSIOLOGY Case 103 19 Atrioventricular Conduction Block Charles Doucette, who is 68 years old, retired from a middle management position in the automotive industry following an acute myocardial infarction. He was recovering in a local hospital, where the physicians closely monitored his electrocardiogram (ECG) [Figure 2-15]. QS Normal Prolonged PR Interval QS Nonconducted P wave Normal Figure 2-15 Effect of atrioventricular conduction block on the electrocardiogram Mr. Doucette's PR intervals were longer than normal. Although his QRS complexes had a normal configuration, there were occasional P waves that were not followed by QRS complexes (nonconducted P waves). He fainted twice in the hospital. The physicians believed that the myocardial infarction caused a block in his atrioventricular (AV) conducting system. While they were discussing the possibility of treating him with atropine, his ECG returned to normal. Mr. Doucette had no more fainting episodes, and he was sent home without further treatment. 11 QUESTIONS 1. What does the PR interval on the ECG represent? What units are used to express the PR interval? What is the normal value? 2. What does the term "conduction velocity" mean, as applied to myocardial tissue? What is the normal conduction velocity through the AV node? How does conduction velocity in the AV node compare with conduction velocity in other portions of the heart? 3. How does AV nodal conduction velocity correlate with PR interval? Why were Mr. Doucette's PR intervals longer than normal? 4. What does the QRS complex on the ECG represent? What is implied in the information that the QRS complexes on Mr. Doucette's ECG had a normal configuration? 5. How is it possible to have P waves that are not followed by QRS complexes? Explain this phenomenon in light of a presumed decreased AV node conduction velocity. 6. Why did Mr. Doucette faint? 7. How might atropine have helped Mr. Doucette? 104 PHYSIOLOGY CASES AND PROBLEMS pi ANSWERS AND EXPLANATIONS 1. The PR interval on the ECG represents the time from initial depolarization of the atria to initial depolarization of the ventricles (i.e., beginning of the P wave to beginning of the R wave). Therefore, the PR interval includes the P wave (atrial depolarization) and the PR segment, an isoelectric portion of the ECG that corresponds to conduction through the AV node, Because PR interval is a time, its units are given in seconds (sec) or milliseconds (msec). You may have needed to look up the normal value for PR interval, which is 120-200 msec (average, 160 msec). 2. Conduction velocity, as applied to myocardial tissue, has the same meaning that it has in nerve or skeletal muscle. It is the speed at which action potentials are propagated within the tissue from one site to the next. Thus, the units for conduction velocity are distance/time [e.g., meters/seconds (m/sec)]. Conduction velocity in the AV is the slowest of all of the myocardial tissues (0.01-0.05 m/sec). Compare this value in the AV node with the much faster conduction velocities in atria and ventricles (1 m/sec) and in His-Purkinje tissue (2-4 m/sec). The slow conduction velocity through the AV node, or AV delay, has a physiologic purpose: it ensures that the ventricles will not be activated "too soon" after the atria are activated, thus allowing adequate time for ventricular filling prior to ventricular contraction. 3. The slower the conduction velocity through the AV node, the longer the PR interval (because the length of the PR segment is increased). Conversely, the faster the conduction velocity through the AV node, the shorter the PR interval. Mr. Doucette's PR intervals were longer than normal because the conduction velocity through the AV node was decreased, presumably because of tissue damage caused by the myocardial infarction. 4. The QRS complex on the ECG corresponds to electrical activation of the ventricles. The normal configuration of Mr. Doucette's QRS complexes implies that his ventricles were activated in the normal sequence (i.e., the spread of activation was from the AV node through the bundle of His to the ventricular muscle). 5. Mr. Doucette's ECG showed some P waves that were not followed by QRS complexes. AV nodal conduction was slowed so much that some impulses were not conducted at all from atria to ventricles. This observation is consistent with increased AV delay and increased PR interval. 6. Mr. Doucette fainted because his arterial pressure was decreased, which caused a decrease in cerebral blood flow. The decrease in arterial pressure is likely related to the absent QRS complexes on the ECG. Each cardiac cycle without a QRS complex is a cardiac cycle in which electrical activation of the ventricles did not occur. If the ventricles were not activated electrically, they did not contract; if they did not contract, they did not eject blood, and mean arterial pressure decreased. 7. The rationale for treating Mr. Doucette with atropine is based on the effect of the parasympathetic nervous system on conduction velocity in the AV node. Parasympathetic nerves innervating the AV node release acetylcholine, which activates muscarinic receptors and decreases AV node conduction velocity. Therefore, atropine (a muscarinic receptor antagonist) opposes this parasympathetic effect and increases AV node conduction velocity. CARDIOVASCULAR PHYSIOLOGY p Key topics Atropine Atrioventricular (AV) node AV delay Conduction velocity Electrocardiogram Muscarinic receptors P wave Parasympathetic nervous system PR interval PR segment C1RS complex 105