Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
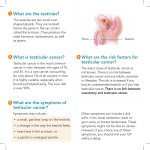
Testicular Cancer • The most common cancer affecting young men in their third or fourth decades of life. • Relatively rare: 1-1.5% of all cancer in men • Highly treatable and usually curable. • The testicles have several types of cells, each of which may develop into one or more types of cancer: they differ in the treatment and prognosis. Testicular Cancer Risk Factors • Age: commonly found in men between 20 and 45. • Family history • Personal history: Men who have had cancer in one testicle are at increased risk for developing cancer in the other testicle. • Race: white men are more likely to be diagnosed. • Cryptorchidism: men with this condition have an increased risk of developing testicular cancer. • Klinefelter's syndrome (extra X chromosom): low levels of male hormones, infertility, breast enlargement, small testicles and increases the risk of developing germ cell tumors. • Human immunodeficiency virus (HIV) infection. • Maternal oestrogen exposure Testicular Cancer Pathology • More than 90% of cancers of the testicle develop in germ cells. (cells that produce sperm). • Germ cell tumors most commonly start in the testicles but can also develop in other parts of the body: – – – – Retroperitoneum Mediastinum Lower spine Pineal gland. • Two main types of germ cell tumors occur in men: • Seminomas may be slightly more common. • Some cancers contain both seminoma and nonseminoma cells. These are treated as nonseminomas. – Seminomas – Non-Seminomas (NSGCT). Seminomas • Two main subtypes – Classical (or typical) • More than 95% of seminomas • Between late 30s and early 50s – Spermatocytic • Occur in older men (55 year old). • Tend to grow more slowly and are less likely to metastasize to other parts of the body than classical seminomas SEMINOMAS Nonseminomas (NSGCT) • Embryonal carcinoma – Present in about 40% of testicular tumors. – Pure embryonal carcinomas occur only 3% to 4% of the time. – Tends to grow rapidly and metastasize outside the testicle. • Yolk sac carcinoma – – – – Cells look like the yolk sac of an early human embryo. Is the most common form of testicular cancer in children. Respond very well to chemotherapy Releases a protein into the bloodstream known as alphafetoprotein (AFP) that helps confirm the diagnosis and is used to track the patient’s response to treatment. Nonseminomas (NSGCT) • Choriocarcinoma – Very rare and aggressive – Occurs in adults. – Is likely to metastasize rapidly to distant organs of the body: lungs, bone, and brain. – Pure choriocarcinoma is rare. – More often, choriocarcinoma cells are present with other types of nonseminoma cells in a mixed germ cell tumor. – Produces a protein, human chorionic gonadotropin (HCG), which can be used to confirm diagnosis and to track the patient’s response to treatment. EMBRYONAL CARCINOMA AND TERATOMA PREDOMINANTLY TERATOMA, WITH EMBRYONAL AND SEMINOMA HISTOLOGICALLY Nonseminomas (NSGCT) Teratomas Mature teratomas – – – – Formed by cells similar to cells of adult tissues. Rarely spread to nearby tissues and distant parts of the body. Usually be cured with surgery. Sometimes deposits of mature teratoma are found after chemotherapy to treat a mixed NSGC: part of a tumor that was left behind after chemotherapy but chemotherapy can change other types of nonseminoma into teratoma. Immature teratomas – Cells look like those of an early embryo – Is more likely to grow into surrounding tissues (invade) and to metastasize outside the testicle – Sometimes recur years after treatment. Teratoma with malignant transformation – Very rare – Have some areas that look like mature teratomas but have other areas where the cells have become a type of cancer that develops outside of the testicle: muscles, glands of the lungs or intestines, or the brain. Carcinoma in situ • Testicular germ cell cancers may begin as a noninvasive form of the disease called carcinoma in situ (CIS) or intratubular germ cell neoplasia. • CIS may not always progress to cancer • It is hard to find CIS before it develops into cancer because it generally causes no symptoms and often does not form a lump • The only way to diagnose CIS is to have a biopsy: incidentally in men who have a testicular biopsy for infertility • Since CIS doesn't always become an invasive cancer observation (watchful waiting) is the best treatment option. Stromal Tumors • They develop in the supportive and hormone-producing tissues, of the testicles. • Less than 4% of adult testicle tumors but up to 20% of childhood testicular tumors. – Leydig cell tumors – Sertoli cell tumors Leydig cell tumors • These tumors develop from the Leydig cells in the testicle (normally produce androgens) • Leydig cell tumors develop in both adults (75% of cases) and children (25% of cases). • They sometimes produce estrogens • Most Leydig cell tumors do not metastasize and are cured with surgery • If they do metastasize have a poor prognosis because they do not respond well to chemotherapy or radiation therapy. Sertoli cell tumors • These tumors develop from normal Sertoli cells, which support the spermproducing germ cells. • They are usually benign; • If they spread, they tend to be resistant to chemotherapy and radiation therapy. Secondary Testicular Tumors • Testicular lymphoma – The most common secondary testicular cancer in men older than 50. – Prognosis depends on the type and stage of lymphoma – The usual treatment is surgical removal, followed by radiation and/or chemotherapy. • In children with acute leukemia, the leukemia cells can sometimes form a tumor in the testicle. • Cancers of the prostate, lung, skin (melanoma), kidney, also can spread to the testicles. • Treatment depends on the specific type of cancer Testicular Cancer • Metastatic spread – Para aortic nodes, lung, brain and bone – Retroperitoneal nodes • Why diagnosis delayed? – Failure to self examine – Failure to visit – Delay in diagnosis Testicular Cancer • PRESENTATION – – – – – – • DD Painless lump in testicle Can “appear” after trauma Can be painful Noticed by partner Breast tenderness or growth Metastasis (back pain, Chest pain, dyspnoea) – Hydrocoele, spermatocoele, calcification of scrotal cysts, infections (orchitis, epididymitis), injury Self-Examination of the Testes Testicular Cancer Guidelines for the diagnosis and staging • • • • Physical examination Testis ultrasound Serum Markers: AFP, hCG and LDH Pathological examination – Biopsy: rarely done – Radical inguinal orchiectomy • Abdomen and chest CT scan: assessment of retroperitoneal, mediastinal and supraclavicolar nodes and visceral state • Retroperitineal Lymph Node Dissection (RPLND) Cancer Stage Grouping • Stage 0. Carcinoma in situ • Stage I. Cancer is limited to the testis • Stage II. Cancer has spread to the lymph nodes in the abdomen • Stage III. Cancer has spread to other parts of the body: lungs, liver, brain and bones . Advanced Testicular Cancer Risk Group Classification • • • • Good-Risk Intermediate-Risk Poor-Risk This is based on the ability to successfully treat patients with this disease. • Patients with poor-risk disease still have about a 50% chance of successful treatment. Testicular Cancer Prognosis and Treatment Options The prognosis and treatment options depend on the following: • Stage of the cancer (whether it is in or near the testicle or has spread to other places in the body, and blood levels of AFP, β-hCG, and LDH). • Type of cancer • Size of the tumor • Number and size of retroperitoneal lymph nodes Guidelines for the treatment Stage I • Seminoma – Para-aortic prophylactic radiotherapy (20 Gy) – Surveillance – Carboplatin-based chemotherapy • NSGCT – Clinical Stage IA (no vascular invasion) • Surveillance • Nerve-sparing RPLND or primary chemotherapy • If RPLND reveals lymph node disease, adjuvant chemotherapy (2 course of PEB) should be considered – Clinical Stage IB (vascular invasion-high risk) • Primary adjuvant chemotherapy (2 course of PEB) is recommended • If chemotherapy is not feasible, nerve-sparing RPLND or surveillance with treatment at relapse (in 50% of patients) are alternative options Guidelines for the treatment Stage II • Seminoma – Low volume: radioterapy (30-36 Gy); when necessary chemotherapy can be used as salvage therapy – High volume: 3 cycles of BEP. residual tumor resection is usually not necessary • NSGCT – Low volume with-out serum markers elevation: surveillance or nerve-sparing RPLND – Low volume with elevated serum markers: chemotherapy (3 cycles of BEP) Guidelines for the treatment: Metastatic NSGCT • Good prognosis NSGCT – BEP x 3 • Intermediate and poor prognosis – BEP x 4 • Residual mass >1cm with tumor markers normal – Surgical resection Side Effects of Cancer and Cancer Treatment • • • • • • • • Anemia Diarrhea Hormone deprivation symptoms in men Infection Nervous system disturbances Sexual dysfunction Skin problems Long-term side effects – Effects of bleomycin on lungs – Effects of chemotherapy on kidneys – Effects of chemotherapy on blood vessels and risk factors for heart disease – Effects of cisplatin on nerves and hearing – Secondary malignancies – Fertility – Effects on testosterone level – Chemobrain Testicular Cancer Follow-up • Regular follow-up is vital • Follow-up schedules depend on the histology, stage and post-orchiectomy treatment option chosen • The aim is to detect relapse as early as possible, to avoid unnecessary treatment and to detect asynchronous tumor in the controlateral testis Testicular Cancer Follow-up • Every one-three months for one-two years. • In each follow-up visit: physical examination, chest x-ray and blood tests for tumor markers • CT scan of abdomen, pelvis and chest are performed once a year. • Treatment of recurrent disease will depend on the stage and extent of the reoccurred disease: experimental chemotherapy schedules • Radiation therapy may be helpful in managing painful or symptomatic areas • For patients with advanced disease, where most treatments have failed, one could consider assistance from hospice