Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Visual Evoked Potentials With Crossed Asymmetry in
Incomplete Congenital Stationary Night Blindness
Frangois Tremblay, Inge De Becker, Cindy Cheung, and G. Robert LaRoche
Purpose. To investigate a proposed postretinal defect in patients with the incomplete form of
congenital stationary night blindness (CSNB2) and to compare visual evoked potential (VEP)
results with those found in various forms of albinism.
Methods. Visual evoked potentials were performed in 10 patients with a diagnosis of CSNB2,
10 subjects with albinism, and 17 normal subjects. Visual evoked potentials were elicited
monocularly with diffuse flash stimulation. Scalp electrodes were placed over each hemisphere
and referred to the forehead. Interhemispheric bipolar recordings were derived, and the
correlation coefficient (CC) was calculated for various segments of the interhemispheric
responses.
Results. A crossed visual evoked potential asymmetry pattern could be demonstrated in 9 of
10 patients with CSNB2. All subjects with albinism and none of the normal subjects showed the
crossed asymmetry pattern. Statistical comparison of the CC computed for various segments of
the interhemispheric response shows that the pattern of inversion in CSNB2 is more prominent in the 25 to 100 msec range (median CC, —0.37) and in the 175 to 250 msec range
(CC, —0.27). In subjects with albinism, all segments show a negative CC (range, —0.46 to
—0.60). In normal subjects, all segments are positively correlated (range, 0.36 to 0.66).
Conclusions. Crossed visual evoked potential asymmetry was found in patients with CSNB2;
therefore, excessive decussation, as demonstrated by this testing procedure, should not be
considered as pathognomonic for albinism. Invest Ophthalmol Vis Sci. 1996; 37:1783-1792.
JL his study was triggered by the examination of a 17year-old boy thought to have ocular albinism (OA).
Visual evoked potentials (VEPs) showed a crossed
asymmetry distribution, as seen in albinism, in which
excessive contralateral decussation has been demonstrated. Surprisingly, electroretinograms (ERGs)
showed an electronegative bright-flash response and
other ERG findings characteristic of CSNB2. In a previous publication,1 we noted that VEPs obtained routinely from a central occipital lead were abnormal in
four patients with CSNB2, raising the suspicion of abnormal postretinal visual pathways.
CSNB2 is a retinal condition first described by
From the Department of Ophthalmology, Dalhousie University, and the fWK- Grace
Health Center, Halifax, Nova Scotia, Canada.
Supported by Dalhousie Medical Research Foundation (CC).
Submitted for publication December 22, 1995; revised March 25, 1996; accepted
April 3, 1996.
/Proprietary interest category: N.
liefmnt requests: Francois Tremblay, Department of Ophthalmology, Izaak Walton
Killam Children's Hospital, 5850 University Avenue, P. O. Box 3070, Halifax,
Nova Scotia, Canada B3J 3C9.
Investigative Ophthalmology & Visual Science, August 1996, Vol. 37, No. 9
Copyright © Association for Research in Vision and Ophthalmology
Downloaded From: http://iovs.arvojournals.org/ on 05/05/2017
Miyake et al.2"3 Clinical manifestations include subnormal visual acuity (range, 0.3 to 0.8), nystagmus, and
strabismus. Fundus examination results were within
normal limits, with the exception of a slightly pale
optic nerve head. However, in our previous study of
15 white patients with CSNB2, we did observe the occurrence of blond fundi (our propositus and three
patients). Clinical manifestations can be subde and
nonspecific; therefore, the diagnosis of CSNB2 is decided by electroretinographic investigations.1"3 Electroretinographic characteristics in CSNB2 are attenuated, but not extinguished, rod-related activity; electronegative bright-flash response with near-normal
early oscillatory potentials; reduced photopic cone bwave; and no response to flicker.
In albinism, the absence of ocular pigmentation
seems to be linked to a sequence of embryonic disorganization that leads to retinal dysfunction and misrouting
of the optic nerve fibers. In normally pigmented persons, fibers originating in the temporal hemiretina remain ipsilateral, whereas the fibers from the nasal hemi-
1783
1784
Investigative Ophthalmology & Visual Science, August 1996, Vol. 37, No. 9
retina decussate and reach the contralateral cortical
hemisphere. In subjects with albinism, a proportion of
the temporal fibers crosses with the nasal fibers, resulting
in excessive decussation and nonoverlapping representation at the cortical level. This pattern of decussation
results in an asymmetric distribution of the scalp potentials across the occiput; the full-field right eye stimulation
evokes a predominantly left cortical hemisphere response, and the left eye stimulation evokes a right cortical activation. Various studies have shown that this pattern of asymmetry is found in albinism but is absent in
other conditions that share certain clinical characteristics with albinism, such as nystagmus,'1 decreased stereopsis (dissociated vertical deviation),5"7 and hypopigmentation (Prader-Willi syndrome).8
For our propositus, the simultaneous occurrence
of pale fundi and crossed VEP asymmetry on the one
hand and the ERG findings characteristic of CSNB2
on the other hand motivated us to investigate further
the chiasmatic decussation in patients with CSNB2.
The current study reports a VEP comparative investigation in patients with CSNB2.
Scotopic ERGs
Photopic ERGs
METHODS
Subjects
Thirty-seven subjects were examined after a protocol
was approved by the Izaak Walton Killam Research
Ethics Board. The protocol follows the tenets of the
Declaration of Helsinki, and informed consent was
obtained after the nature of the study was explained.
Ten patients with a diagnosis of CSNB2, who already
had been reported in a previous publication,1 were
identified from a retrospective chart study.9 The diagnosis of CSNB2 was secured with electroretinographic
investigations based on the following criteria: attenuated, but not extinguished, rod-related activity; electronegative bright-flash response with near-normal
early oscillatory potentials; reduced photopic cone bwave; and no response to flicker (see Fig. 1). Most
patients had unexplained visual acuity reduction (0.3
or better), mild nystagmus, or family history of
CSNB2. Fundus examination results were normal except for mild temporal optic disc pallor in six patients.
Ten patients with albinism were diagnosed based on
the following criteria: pale chorioretinae, foveal hypoplasia, nystagmus, iris diaphany, family history, normal
or supernormal ERGs, and VEP-crossed asymmetry. A
summary of the clinical findings for both groups is
found in Table 1. Seventeen normal age-matched volunteers also were evaluated.
Protocol
The protocol used in this study follows the guidelines
developed for detection of the crossed cortical asym-
Downloaded From: http://iovs.arvojournals.org/ on 05/05/2017
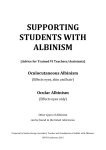
l. Representative electroretinographic recordings in
one patient with CSNB2. Dark tracings are from a representative patient, and gray traces are from an age-matched subject. Trace 1: scotopic (30 minutes of dark adaptation under
dim red room illumination) single blue flash (Kodak Wratten 47, 47a, and 47b filter 1 cd-m~v!-sec source flash; four
sweeps averaged) show a small but consistent rod response.
Trace 2: scotopic bright-flash (1 cd"m~2#sec, no interference filter; four sweeps averaged) response showing delayed
but large amplitude a-wave and a small (electronegative) bwave. Trace 3: large amplitude oscillatory potentials (100
Hz to 1 kHz filter) were derived from trace 2. Trace 4:
photopic (34 cd-m~2-sec background) single flash (10
cd • m~2 • sec; 10 sweeps averaged) response, showing a delayed a-wave and a b-wave that hardly returns to the baseline
level. Trace 5: absence of oscillatory potentials when trace
4 is derived (100 Hz to 1 kHz filter) from trace 1. Trace 6:
flicker stimulation (33.3 Hz); no response could be elicited.
Triangles = stimulus onset. Calibration: {horizontal) traces
1 to 2, 40 msec; traces 3 to 5, 20 msec; trace 6, 80 msec.
Calibration: {vertical) traces 1, 2, 6, 300 /zV; traces 3, 5, 30
/iV; trace 4, 150 //V.
FIGURE
metry resulting from optic fiber misrouting.1 Gold dermal disc electrodes were fixed on the scalp (EC2 electroconductive cream; Grass Instruments, Quincy, MA)
after skin preparation. The active electrodes were positioned over both hemispheres, 5 cm from the midline
VEPs Crossed Asymmetry in CSNB2
1785
TABLE l. Summary of Clinical Findings in Subjects With Albinism and CSNB2
Visual acuity range
Age
Sex
Nystagmus
Fundus
Stereoacuity
Electroretinograms
Visual evoked potentials
Albinism
CSNB2
0.1-0.3 (mean 0.17)
1-35 (mean 10.7)
5M.5F
8/10
Mild to definite hypopigmentation 10/10
Macular hypoplasia 6/10
Pallor of disc 0/10
Worse than 400"
Normal 6/6 (done in 6/10)
Crossed asymmetry 10/10
0.25-0.7 (mean 0.44)
4-19 (mean 8.8)
10 M
3/10
Mild hypopigmentation 4/10
Macular hypoplasia 0/10
Pallor of disc 6/10
As good as 60"
Electronegative bright-flash 10/10
Crossed asymmetry 9/10
and 3 cm above the inion (O| and O 2 ). The reference
electrode was positioned at FPz, and the left earlobe
was used as a common ground. Bandwidth of the amplifier (Spirit system; Nicolet, Madison, WI) was set at
0.1 to 1 kHz. Two to four series of 100 sweeps were
averaged. The number of series averaged was determined by the intertrial variability as judged by an experienced observer (FT). Data were stored on disk for
off-line analysis.
The evoked potential stimulus consisted of a diffuse flash presented monocularly at 2.3 Hz through
red light-emitted diodes incorporated into goggles
(S10VSB; Grass Instruments). The mean luminance
of the 5 msec duration square-wave flash was 30
cd • m~2 • sec. The first eye stimulated was selected randomly. In the pediatric population, the flash-VEP generally provides more robust and reliable responses
than the pattern-onset stimulus presentation because
no fixation is required.10 Pattern-onset stimulation
(Nicolet 1015 stimulator; Nicolet) was provided when
the flash stimulus was not generating a consistent response. Mean luminance was set at 22 cd • ~2 with a
contrast of 90%. Check size was 40 minutes of arc,
and the whole stimulation field subtended an area of
16° X 20°. Pattern was presented for 80 msec and
alternated with an equiluminant gray unpatterned
field at a rate of 2.3 Hz.
Data Analysis
Off-line analysis first consisted in the summation of
the averages obtained. A Gaussian smoothing function
(9 points) then was applied. After an inversion in polarity, channel O| was algebraically subtracted from
channel O2; the resultant wave was the computed interhemispheric difference during a monocular stimulation. The same procedure was applied to waves from
the other eye. However, as reported in cases of albinism," the VEP responses can be too weak and distorted to reflect clearly the crossed asymmetry when
using a calculation based on amplitude measurements.1 Therefore, we developed a technique inde-
Downloaded From: http://iovs.arvojournals.org/ on 05/05/2017
pendent of the peak amplitude detection to quantify
more objectively the interhemispheric differences.
As an index of asymmetry between the two resultant
waves, the correlation coefficient (CC) was computed.
A value of +1 is representative of an exact match between the two waves, a value of — 1 represents two identical waves of opposite polarity, and values close to 0 represent uncorrelated activity. To palliate the absence of
amplitude recognition of the CC, the covariance (CoV)
also was calculated as an index of the signal's magnitude.
The formula IAV = log I
j was developed, where
IAV is die index of amplitude variation, Covx.x is the
covariance calculated for a given segment of the interhemispheric responses, and Cov,, is the covariance calculated for the prestimulus segment of the original hemispheric responses (—40 to 0 msec). Values of IAV equal
to or lower than 0 indicate amplitude variations within
the CC segment considered in the range of the noise
level or the original data. Thus, CC values are considered
to reflect true asymmetry only when IAV is superior to
0. Segmental analysis was performed on various portions
of the waves: 25 to 100, 50 to 125, 75 to 150, 100 to 175,
125 to 200, 150 to 225, and 175 to 250 msec after the
stimulus onset. For all the segments analyzed, nonparametric statistical analysis (Mann-Whitney, Statview; Abacus Concept, Berkeley, CA) was performed on CC to
compare the significance of the group differences.
RESULTS
Qualitative Analysis
In normal subjects (Fig. 2; Nl to N12), monopolar
derivations at Ol and O2 typically produce deflections
with the main positivity in the vicinity of 80 to 120
msec. Cortical responses could have variable morphology, from typical adult-like responses to less mature,
simpler morphology. Bipolar derivations (obtained
off-line by the inversion of O2 and its addition to Oi)
could show high interhemispheric symmetry (N5 to
Investigative Ophthalmology 8c Visual Science, August 1996, Vol. 37, No. 9
1786
Normal
Q-,-02
CVO2
OD
OD
100
100
Albinism
OS
OD
100
100
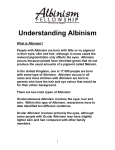
FIGURE 2. Visual evoked potentials in response to monocular stimulation in two normal
subjects with low and high interhemispheric potential variations (Nl to N6, N7 to N12) and
two patients with albinism (Al to A6, A7 to A12) and with CSNB2 (Cl to C6, C7 to C12).
Two patterns of asymmetry could be observed, interhemispheric amplitude variations (bold
arroius) and implicit time variations (dashed lines). OS = left eye stimulation; OD = right eye
stimulation. O| and O2 are recordings from electrodes overlying the left and right hemisphere, respectively, and d — O2 refers to the off-line computation of the interhemisheric
potential variations. Refer to Qualitative Analysis, Results section, for more detailed explanation. Dots = stimulus onset. Calibration as indicated.
N6) or relatively large interhemispheric differences
( N i l to N12), in spite of consistent hemispheric responses (traces 7 to 10). Consistent symmetric bipolar
recordings could be obtained even with uncooperative
children.
In albinism, a different pattern emerged. Monopolar response characteristics are the same, though
the overall amplitude can be reduced drastically in
some cases, as reported by Bouzas.'' However, the cortical distribution of the evoked responses varies in
function of the eye stimulated. In the case presented
in Figure 2 (Al to A6), contralateral responses yielded
a large biphasic wave, whereas ipsilateral responses
Downloaded From: http://iovs.arvojournals.org/ on 05/05/2017
were smaller and less wavy (bold arrows; compare Al
to A2 and A3 to A4). The crossed asymmetry could
be visualized easily by direct comparison of traces Al
and A4 (large contralateral responses) or A2 and A3
(smaller ipsilateral responses). The bipolar derivations (equivalent to O| — O2) computed from the
monocular recordings showed inverted waves characteristic of a crossed asymmetry (arrows, A5 to A6).
In other cases, waves had similar amplitudes in both
hemispheres but different culmination times regarding the main positivity (compare A7 to A9 and A8 to
A10; dashed lines). Again, this led to the characteristic
inverted interhemispheric responses (arrows; A l l to
1787
VEPs Crossed Asymmetry in CSNB2
A12). Such inversions were observed in all 10 subjects
with albinism, even in those in whom VEP amplitudes
were low. These two patterns of VEP characteristics
have been observed before.1213
In patients with CSNB2 (Fig. 2; Cl to C12), a
pattern of crossed asymmetry also was observed. In the
first example (Cl to C6), the hemispheric responses
contralateral to the eye stimulated had smaller biphasic positivity (bold arrow; C2 to C3), whereas the ipsilateral responses were simple, large positivity (compare Cl and C4). Interhemispheric comparison accomplished by wave subtraction revealed consistent
oscillatory variations of opposite polarity (arrows; C5
and C6). In another case presented in traces C7 to
C12, the crossed asymmetry was more difficult to visualize because the response differences relied more on
the temporal relationship than on wave morphology.
Here, the ipsilateral responses (C7 for the left eye and
CIO for the right eye) had monophasic, short, implicit
time peaks. Contralateral responses yielded a major
positivity with longer implicit time. The computed bipolar comparison (Cll to C12) revealed a clear inversion of waves in the early phase of the response (see
arrows). As in albinism, the two patterns of hemispheric asymmetry (wave morphology and implicit
time delay) produced the inverted interhemispheric
responses considered characteristics of chiasmatic misrouting. This inversion was observed clearly in the
early phase (between 25 and 100 msec after the stimulus onset) of the response in 6 of 10 patients with
CSNB2 and was present in the late phase of the response (between 150 and 250 msec) in two other subjects. Most of the results presented in this study were
obtained using diffuse flash stimulation. In the pediatric population, this has proven to be a sufficient stimulus; the use of the pattern-onset stimulus did not improve the magnitude of the inversion and, therefore,
was not retained for quantitative analysis. However, in
a few cases, it has been necessary to use a patternonset stimulus to prove the inversion. In two of the
oldest patients in whom the inversion could not convincingly be observed with the flash stimulation (see
Figs. 3, 5, 6; dashed arrows), a pattern-onset stimulus
resulted in a more negative CC and a more convincing
visualization of the inversion of the interhemispheric
potentials (Figs. 3,11,12; arrows). In two patients with
CSNB2, no negative correlation could be demonstrated with either stimulus.
Quantitative Analysis
Quantitative analysis was performed to measure the
degree of inversion observed in crossed asymmetry
and its distribution in the time series. For that purpose, correlation coefficients and covariations were
computed for segments of 75 msec covering the first
Downloaded From: http://iovs.arvojournals.org/ on 05/05/2017
Flash-VEPs
01
O2
OS
OD
Pattern-Onset VEPs
OS
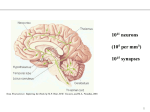
3. Visual evoked potentials in one patient with
CSNB2 with a small asymmetry with the flash-evoked response (traces 1 to 6, dashed arrows in traces 5 and 6)
and a larger asymmetry with a pattern-onset checkerboard
stimulation (traces 7 to 12, arrows in traces 11 and 12). OS
= left eye stimulation; OD = right eye stimulation. Oi and
O2 are recordings from electrodes overlying the left and
right hemisphere, respectively, and Oi — O2 refers to the
off-line computation of the interhemisheric potential variations, (traces 1 to 6) Dots = stimulus onset, (traces 7 to 12)
Line up is checkerboard presentation. Calibration as indicated.
FIGURE
250 msec after stimulus. The choice of an analysis time
of 75 msec was guided by the fact that 75 msec (»12
to 15 Hz) corresponds to a major peak of the fast
Fourier transform performed on these waves. Table 2
summarizes the results for window analysis of 75 msec,
starting at 25 msec after stimulus and covering the first
250 msec of the responses. For the group of normal
subjects, the correlation coefficient was positive and
varied between 0.36 to 0.66. This high positive correlation indicates a high degree of symmetry between the
two interhemispheric responses. In the group with albinism, the CC was strongly negative, varying between
—0.46 and —0.60, indicating the opposite pattern of
the two interhemispheric responses. The CC was fairly
constant throughout the response scanned.
In the group with CSNB2, negative CC was observed in the first and last time window analyzed, at 25
to 100 and 175 to 250 msec. These two time windows
correspond to the two main positivities observed in
normals. The other time windows yielded relatively
lower positive CC, which suggests a poorer synchronization of the signal. Statistical comparisons (MannWhitney unpaired comparison) demonstrated that
the group with CSNB2 differed significantly from the
normal group (Table 2, N/C column; P < 0.05) in
1788
Investigative Ophthalmology & Visual Science, August 1996, Vol. 37, No. 9
TABLE 2.
Median and 25th (Q25) and 75th (Q75) Percentiles for the Correlation Coefficient
Computed for Seven Time Windows From the Groups of Normal, Albinism,
and CSNB2 Patients
Statistical Comparison (P)
Albinism
Normal
Window
(msec)
Median
25-100
50-125
75-150
100-175
125-200
150-225
175-250
o»
0.62
0.65
0.63
0.36
0.55
0.64
0.66
24.5
43.2
-3.2
-17.7
12.2
47.0
14.7
Median
82.0
92.0
85.2
86.7
83.2
87.0
88.7
CSNB2
Q«
Median
Q.25
o.»
-12.0
4.2
-2.7
-13.2
27.7
73.7
28.7
-0.37
0.34
0.34
0.38
0.60
0.11
-0.27
-69.0
-43.0
-61.0
-1.0
-6.0
6.0
-63.0
32.0
70.0
73.0
64.0
72.0
44.0
5.0
Q.25
-0.54
-0.48
-0.60
-0.56
-0.46
-0.47
-0.51
-78.0
-79.5
-88.2
-87.2
-82.7
-57.0
-77.0
the two first and two last segments analyzed, whereas
the group with albinism differed from the normal
group in all the segments analyzed (N/A column).
Figure 4 illustrates the significance of CC in function
of the CoV, calculated for the same data. The knowledge
of the covariance is an important piece of information
because the CC itself can, in some circumstances, be
misleading. For instance, almost isoelectric interhemispheric recordings can produce low or even negative
CC while, in fact, the two waves are similar. When the
two waves to be compared are low in amplitude, the
noise level becomes disproportionately important and
biases the CC. To reduce this bias, the ratio between
the CoV calculated for the segment analyzed and the
25-100 MSEC
Normal
CSNB2
Albinism
CSNB2
0.001
0.001
0.005
0.004
0.004
0.04
0.009
0.007
0.06
0.53
0.51
0.97
0.03
0.02
0.29
0.01
0.04
0.02
0.003
0.20
0.23
CoV calculated from the prestimulus baseline is computed (CoV ratio). By doing this, the CC is scaled to
the level of original VEP background activity. When the
interhemispheric responses are low in amplitude compared to the original data background noise, the CoV
ratio is approximately unity (log CoV = 0); the significance of the CC is then reduced because it is influenced
primarily by the background activity. On the other hand,
when log(CoV ratio) is above 0, the CC is significant
because it measures the evoked potential differences
above the noise in the original data.
Thus, the scattergraphs in Figure 4 present the
CC as a function of log(CoV ratio) for three time
windows: from 25 to 100 msec (where the major posi-
ALBINISM
NORMAL
Normal
Albinism
CSNB2
2.5 .
2.0.
1.5-
•
1.0.
• *
•
0.5.
. .»-
•
-0.5.
•
#
-1.0
-100
-75
-50 -25
0
25
50
75
100
125
-100 -75
-50
-25
25
50
75
100
125
-100 -75
-50
25
-25
50
75
100
125
Correlation Coefficient
FIGURE 4. Scattergraph illus-
100-175 MSEC
2.5
2.5.
2.5.
•
2.0 .
2.0.
1.5 .
1.5.
V
•
1.00.5-
•
-50
-25
25
50
75
|
OS-
#
1.0.
•
*
* •
*
•
•
•
•
•
•
0.5.
100
•
1.5.
LO-
0.5-
1,0
-100 -75
2.0 •
t
0.5-
125
1.0
-100 -75
-50
-25
25
50
75
100
125
10
-100 -75
-50
-25
25
50
75
100
125
125
-100 -75
-50
-25
25
50
75
100
125
•100 -75
-50
-25
25
50
75
100
125
175-250 MSEC
2.5.
2.0.
• •
1.5.
1.0.
0.5 .
•w*
0.5.
10
100 -75
-SO
-25
25
SO
75
100
Downloaded From: http://iovs.arvojournals.org/ on 05/05/2017
trating the correlation coefficient (CC) computed for
various segments of the monocular flash-evoked interhemispheric recordings and
its relation with the log ratio
of the covariance, for the
groups of normal subjects,
subjects with albinism, and
patients with CSNB2. A log
(CoV ratio) ratio value of 0
indicates a signal amplitude
at the noise level, and any
data close to this value should
not be considered.
VEPs Crossed Asymmetry in CSNB2
tivity in the evoked response usually is found), from
100 to 175 msec, and from 175 to 250 msec (where
late evoked responses usually occur). Data from the
normal subjects, subjects with albinism, and patients
with CSNB2 are presented in three separate columns.
In the normal group, CC was high and positive, and
log(CoV ratio) was generally above 0. In some cases,
the CC could be low or even negative, but this usually
was associated with a log(CoV ratio) that was also low,
which means that this portion of the VEP signal was
almost isoelectric and was influenced primarily by the
background activity. This was particularly true in the
intermediate portion of the VEP signal (100 to 175
msec), between the two main positivities. In the group
with albinism, the CC had high negative values, and
the log(CoV ratio) generally was also high. In most
instances, the CC could be interpreted easily. For the
group of patients with CSNB2, the majority of the
early and late segments were correlated negatively,
whereas in the intermediate segment, results were
more variable. Data from the few patients presenting
with "significant" positive CC in the 25 to 100 msec
segment usually were associated with negative CC in
the 175 to 250 msec segment. Therefore, all but one
patient had at least one negative CC above the noise
level.
DISCUSSION
In patients with CSNB2, VEP-crossed asymmetry was
detected reliably through flash stimulation. This is the
first report of a postretinal dysfunction in CSNB2. In
an electroretinographic investigation previously performed on a group of 15 patients with CSNB2, we
briefly mentioned that binocular VEP anomalies were
found in 5 of them. 1
To date, few studies have demonstrated VEP asymmetry in conditions other than albinism. To our
knowledge, only one report on a family with congenital nystagmus14 and one report on patients with dissociated vertical deviation 1 ' have shown such asymmetry.
The results of these two studies were based on monocular hemifield (pattern-reversal) stimulation, a technique difficult to apply reliably because of the requirement for steady fixation. Moreover, the results of those
two studies could not be reproduced by others, who
used the same technique"' or a diffuse flash or patternonset stimulation protocol.'1'7 On the basis of the latter
studies, it seems reasonable to consider dissociated
vertical deviation as not demonstrating crossed asymmetry. Reports from patients with idiopathic congenital nystagmus4 and Prader-Willi syndrome 8 also were
negative.
Because VEP asymmetry reflects abnormal decussation, it is generally accepted as diagnostic of albi-
Downloaded From: http://iovs.arvojournals.org/ on 05/05/2017
1789
nism. However, Guillery (personal communication,
cited in Regan17) "raised the point that the known
incidence of misrouting in albinos might be only the
'tip of the iceberg' in the general population and that
some non-albino individuals—especially those with
fair hair and blue eyes—might experience a lesser
degree of misrouting, possibly associated with comparatively minor visual problems." This comment, along
with some animal reports (normally pigmented cats
heterozygous for albinism) 18 also contribute to the
idea. Miswiring might not be the exclusive characteristic of albinism—it might be found in other conditions.
Crossed Asymmetry in CSNB2
In albinism, hypopigmentation is accompanied by a
slightly disorganized retina, underdevelopment of the
macular area, and a decreased number of rods and ganglion cells.19'20 Evidence is accumulating to support the
idea that the absence of retinal pigment disrupts the
development of the normal spatio-temporal sequence of
events in the developing neural retina.21"2'1 For instance,
ganglion cells from the temporal hemiretina that remain
uncrossed at the optic chiasm are generated and grow
out before ganglion cells from the same area, which are
destined to grow contralaterally to the optic chiasm. The
expression of the tyrosinase gene occurs simultaneously
with this early ganglion cell sprouting. One could hypothesize a time relationship between melanogenesis
and ganglion cell development; the disruption in melanogenesis or simply a delay in its occurrence could result
in optic tract disorganization (see references 21 and 25
for review of current concepts). Could it be that, in
CSNB2, melanogenesis is complete but is not coordinated with ganglion cell development? This would have
an impact on the timely focal axonal guidance of the
ganglion cell but not necessarily on the more extended
development of retinal organization.
Central visual acuity in CSNB2 is subnormal. Unlike central visual acuity albinism,26'27 there is no foveal
hypoplasia to explain this reduction in acuity. The
ERG is severely abnormal 1 but, as already proposed
for other retinal conditions, 28 " 32 the retinal network
may be functional and may not contribute to visual
acuity reduction. The abnormal development of the
optic tract fibers with oversampling of the crossed
pathway and subsequent reorganization of the visual
cortex topography could be considered as one contributing factor for the reduced visual acuity observed
in CSNB2.
CSNB2 Is Not Albinism
Although crossed asymmetry generally is considered
diagnostic of albinism,9 we think CSNB2 is not a form
of albinism. The clinical manifestations of CSNB2 and
1790
Investigative Ophthalmology 8c Visual Science, August 1996, Vol. 37, No. 9
mild cases of OA can be similar: mild to moderate
subnormal visual acuity, nystagmus, strabismus, and
refractive errors. Retinal pigmentation does not necessarily distinguish between CSNB2 and OA: CSNB2 indeed has normal, retinal pigmentation, and many patients with mild OA have a blond fundus that is within
normal limits for the white population.1"3 The ERG
manifestations are different in CSNB2 and OA.1"3 In
OA and oculocutaneous albinism, ERGs are normal
or supernormal.33 In CSNB2, electronegative brightflash responses and attenuated cone signal are found.'
The VEP manifestations in CSNB2 are not as severe
as in albinism; in most subjects with CSNB2, a negative
correlation was observed only at punctual locations
in the time series, whereas in albinism, the negative
correlation could be found over the entire extent of
the 250 poststimulus responses. Stereoacuity is poor
in albinism, whereas in at least some of our patients
with CSNB2, stereoacuity is relatively good (60 seconds of arc on Titmus in one of our patients). These
observations suggest that the crossed decussation may
not be as complete in CSNB2 as in albinism. The different pattern of asymmetry observed in CSNB2 may
reflect a different cortical reorganization, such as an
incomplete topographic mapping of the vertical meridian or a different pattern of intracortical suppression, as has been proposed for the Siamese cat.21 It
remains, however, a matter of speculation.
Aland Island Eye Disease
Previous reports suggest that CSNB2 and AIED (type
2 ocular albinism; MIM NO:30060) are indistinguishable clinically34"36 and that both entities are associated
with reduced visual acuity, elevated dark adaptation
threshold, and, as a frequent associated rinding, nystagmus. In addition, AIED is associated with high myopia, hypoplasic fovea, hypopigmented fundi, and
slight protanomalous-like dyschromatopsia.35'37'38 In
AIED, ERGs are strongly abnormal—electronegative
bright-flash responses with reduced a-wave amplitude,
strongly attenuated rod-isolated activity, and cone isolated responses.35'37 We agree with Glass39 that ERGs
in CSNB2 are less severely affected than in AIED; cone
activity, though severely attenuated, seems to be larger
in CSNB2, and oscillatory potentials reach almost normal amplitude when recorded in scotopic conditions.
Thus, CSNB2 and AIED overlap considerably in their
clinical and psychophysical aspects. However, in AIED,
no crossed asymmetry could be demonstrated,38"40
whereas most of our patients with CSNB2 had asymmetry. It is reasonable not to consider CSNB2 and AIED
as die same entity, though a clear clinical delineation
is sometimes difficult to establish.
So far, molecular analysis could not exclude the
possibility that CSNB2 and AIED are caused by muta-
Downloaded From: http://iovs.arvojournals.org/ on 05/05/2017
tions in the same gene. There is a thigh link to Xpll
loci in AIED, and, for now, its association with Xp21
(complex glycerol kinase deficiency, including Duchenne muscular dystrophy, for which electronegative
bright flash responses were demonstrated30'31"41) could
not be corroborated.39'42 CSNB2 has been reported to
link with the Xpll loci,43'44 though it is unclear from
the existing literature whether CSNB2 and CSNB1
have been segregated completely. The question of allelism or linked genes between AIED, CSNB1, and
CSNB2 remains open.
Interestingly, several retinal conditions result in
an electronegative bright-flash response that originates from the Xpll.3 to Zp22.3 segment. Patients
with Duchenne muscular dystrophy (Xp21.2) and retinoschisis (Xp22.3) also have severely abnormal ERGs
though most of their psychophysical functions remain
well preserved. As with CSNB2, the inconsistency between ERG findings and psychophysical data points
toward glial cell dysfunction rather than to neuronal
involvement. Whether this association is coincidental
remains to be determined. The OA locus is located in
the same vicinity. Could the electronegative ERGs and
to crossed asymmetry result from the same gene defect
is still unknown.
In conclusion, the VEP protocol for the detection
of crossed asymmetry may not be decisive to support
the diagnosis of albinism. From a clinical point of
view, any male patient with a presumptive diagnosis
of ocular albinism based on VEP-crossed asymmetry
should undergo ERG investigation so a possible diagnosis of CSNB2 is not overlooked.
Key Words
albinism, CSNB2, optic chiasm, retinal degeneration, retinal
ganglion cells, visual evoked potentials
References
1. Tremblay F, LaRoche RG, De Becker I. The electroretinographic diagnosis of the incomplete form of congenital stationary night blindness. Vision Res. 1995;
35:2383-2393.
2. Miyake Y, Yagasaki K, Horiguchi M, Kawase Y, Kanda
T. Congenital stationary night blindness with negative
electroretinogram: A new classification. Arch Ophthalmol. 1986; 104:1013-1020.
3. Miyake Y. Incomplete type congenital stationary night
blindness. In: Heckenlively JR, Arden GB, eds. Principles and Practice of Clinical Electrophysiology of Vision. St.
Louis: CV Mosby; 1991:721-725.
4. Apkarian P, Shallo-Hoffmann J. VEP projections in
congenital nystagmus; VEP asymmetry in albinism: A
comparison study. Invest Ophthalmol Vis Set. 1991;
32:2653-2661.
5. Kriss A, Timms C, Elston, Taylor D, Gresty M. Visual
evoked potentials in dissociated vertical deviation: a
reappraisal. Br J Ophthalmol. 1989; 73:265-270.
VEPs Crossed Asymmetry in CSNB2
6. Boylan C, Clement CA, Howrie A. Normal visual pathway routing in dissociated vertical deviation. Invest
Ophthalmol Vis Sci. 1988;29:1165-1167
7. Bach M, Kommerell G. Albino-type misrouting of the
optic nerve fibers not found in dissociated vertical
deviation. Graefe's Arch Clin Exp Ophthalmol. 1992;
230:158-161.
8. Roy S. Prader-Willi syndrome: A clinical and visually
evoked potential study. ARVO Abstracts. Invest Ophthalmol Vis Sci. 1991; 32:761.
9. Apkarian P, Reits D, Spekreijse H, van Dorp D. A
decisive electrophysiological test for human albinism.
Electroencephalogr Clin Neurophysiol. 1983; 55:513-531.
10. Russell-Eggitt I, Kriss A, Taylor DSL Albinism in
childhood: A flash VEP and ERG study. BrJ Ophthalmol. 1990; 74:136-140.
11. Bouzas E, Caruso RC, Drews-Bankiewicz MA, KaiserKupfer MI. Evoked potential analysis of visual pathways in human albinism. Ophthalmology. 1994;
101:309-314.
12. Guo S, Reinecke RD, Fendick M, Calhoun JH. Visual
pathway abnormalities in albinism and infantile nystagmus: VECPs and stereoacuity measurements. JPediatr Ophthalmol Strabismus. 1989; 26:97-104.
13. Carroll WM, Jay BS, McDonald WI, Halliday AM. Two
distinct patterns of visual evoked response asymmetry
in human albinism. Nature. 1980; 286:604-606.
14. Meienberg O, Hemphill G, Rosenberg M, Hoyt WF.
Visually evoked response asymmetries in a family with
congenital nystagmus. Arch Neurol. 1980;37:397-402.
15. Fitzgerald BA, Billson FA. Dissociated vertical deviation: Evidence of abnormal visual pathway projection.
BrJ Ophthalmol. 1984; 68:801-806.
16. Krill AE, Martin D. Photopic abnormalities in congenital stationary nightblindness. Invest Ophthalmol Vis Sci.
1971; 10:625-636.
17. Regan D. Human Brain Electrophysiology. Amsterdam:
Elsevier; 1989:548-552.
18. Leventhal A, Vitek DJ, Creel DJ. Abnormal visual pathways in normally pigmented cats that are heterozygous
for albinism. Science. 1985;220:1395-1396.
19. Jeffery G, Darling K, Whitmore A. Melanin and the
regulation of mammalian photoreceptor topography.
EurJNeurosci. 1994; 6:657-667.
20. Guillery RW. Neural abnormalities of albinos. Trends
Neurosd. 1986; 9:366-369.
21. Sretavan DW. Specific routing of retinal ganglion cell
axons at the mammalian optic chisasm during embryonic development. J Neurosd. 1990; 10:1995-2007.
22. Drager UC. Birthdates of retinal ganglion cells giving
rise to the crossed and uncrossed optic projection in
the mouse. Proc R Soc Lond B Biol Sd. 1985; 224:5777.
23. LaVail JH, Nixon RA, Sidman RL. Genetic control of
retinal ganglion cell projections. / Comp Neurol.
1978; 182:399-422.
24. Colello RJ, Jeffery G. Evaluation of die influence of
optic stalk melanin on die chiasmatic pathways in the
developing rodent visual system. / Comp Neurol.
1991; 305:304-523.
Downloaded From: http://iovs.arvojournals.org/ on 05/05/2017
1791
25. Silver J, Sapiro J. Axonal guidance during development of the optic nerve: die role of pigmented epithelia and odier extrinsic factors. / Comp Neurol.
1981;202:521-538.
26. Kinnear PE, Jay B, Witkop CJ. Albinism. Suw Ophthalmol. 1985; 30:75-101.
27. Abadi RV, Pascal E. Visual resolution limits in human
albinism. Vision Res. 1991;7/8:1445-1447.
28. Kellner U, Foester MH. Cone dystrophies with negative electroretinogram. BrJ Ophthalmol. 1993; 77:404409.
29. Perlman I, Leibu R, Barth J. Night blindness: A new
type with abnormal properties of the electroretinogram. Clin Vision Res. 1993;8:159-169.
30. Tremblay F, De Becker I, Dooley JM, Riddell DC.
Duchenne muscular dystrophy: Negative scotopic
bright-flash electroretinogram but not congenital
stationary night blindness. Can J Ophthalmol. 1994;
29:274-279.
31. Jensen H, Warburg M, Sjo O, Schwartz M. Duchenne
muscular dystrophy: Negative electroretinograms and
normal dark adaptation: Reappraisal of assignment
of X linked incomplete congenital stationary night
blindness. J Med Genet. 1995; 32:348-351.
32. Peachey NS, Fishman GA, Derlaki DJ, Bringell MG.
Psychophysical and electroretinographic findings in
X-Linked juvenile retinoschisis. Arch Ophthalvwl. 1987;
105:513-516.
33. Wack MA, Peachey NS, Fishman GA. Electroretinographic findings in human oculocutaneous albinism.
Ophthalmology. 1989;96:1778-1785.
34. Krill A. Congenital stationary night blindness. In:
Krill's Hereditary Retinal and Choroidal Diseases. Vol. II.
New York: Harper & Row; 1977:391 -420.
35. Rosenberg T, Schwartz M, Simonsen SE? Aland eye
disease (Forsius-Eriksason-Miyake syndrome) with
probability established in a Danish family. Ada Ophthalmol. 1990; 68:281-291.
36. Weleber RG, Pillers D-AM, Powell BR, Hanna CE, Magenis RE, Buist NRM. Aland Island eye disease (Forscius-Eriksson syndrome) associated with contiguous
deletion syndrome at Xp21: Similarity to congenital
stationary night blindness. Arch Ophthalmol. 1989;
107:1170-1179.
37. Carlson S, Vesti E, Raitta C, Donner M, Eriksson AW,
Forsius H. Clinical and electroretinographic comparison between Aland island eye disease and a newly
found related disease with X-chromosomal inheritance. Ada Ophthalmol. 1991;69:703-710.
38. O'Donnell FE, Green WR, McKusick VA, Forsius H,
Eriksson AW. Forsius-Eriksson syndrome: Its relation
to die Nettleship-Falls X-linked ocular albinism. Clin
Genet. 1980; 17:403-408.
39. Glass IA, Good P, Coleman MP, Fullwood P, Giles MG,
Lindsay S, et al. Genetic mapping of a cone and rod
dysfunction (Aland Island eye disease) to the proximal short arm of the human X chromosome. / Med
Genet. 1993; 30:1044-1051.
1792
Investigative Ophthalmology 8c Visual Science, August 1996, Vol. 37, No. 9
40. van Dorp DB, Eriksson AW, Delleman JW, et al. Aland
eye disease: No albino misrouting. Clin Genet. 1985;
28:526-530.
41. Pillers D-AM, Bulman DE, Weleber RG, et al. Dystrophin expression in the human retina is required
for normal function as defined by electroretinography. Nat Genet. 1993;4:82-86.
42. Alitalo T, Kruse TA, Forsius H, Eriksson AW, de la Chapelle A Localization of the Aland Island eye disease locus
Downloaded From: http://iovs.arvojournals.org/ on 05/05/2017
to the pericentric region of the X chromosome by linkage
analysis. Am J Hum Genet. 1991;48:31-38.
43. Musarella MA, Weleber RG, Murphey WH, et al. Assignment of the gene for complete X-linked congenital stationary night blindness (CSNB1) to Xpll.3. Genomics. 1989; 5:727-737.
44. Pearce WG, Reedyk M, Couplan dSG. Variable expressivity in X-linked congenital stationary night blindness. Can J Ophthalmol. 1990;25:3-10.